Decades before a single memory slips, the same midlife problems that clog arteries — high blood pressure, high apoB/LDL, diabetes, belly fat, atrial fibrillation — are quietly seeding dementia, and this review argues that aggressive, timed cardiovascular prevention is one of the most powerful brain-protection strategies we have.
For most of medical history, the heart and the brain were treated as separate kingdoms with separate specialists. A new perspective from a US preventive-neurology group argues that this division is a clinical mistake we can no longer afford. Their core claim is simple and increasingly hard to dispute: cardiovascular disease and neurodegenerative disease are largely the same disease process, viewed through two different organs.
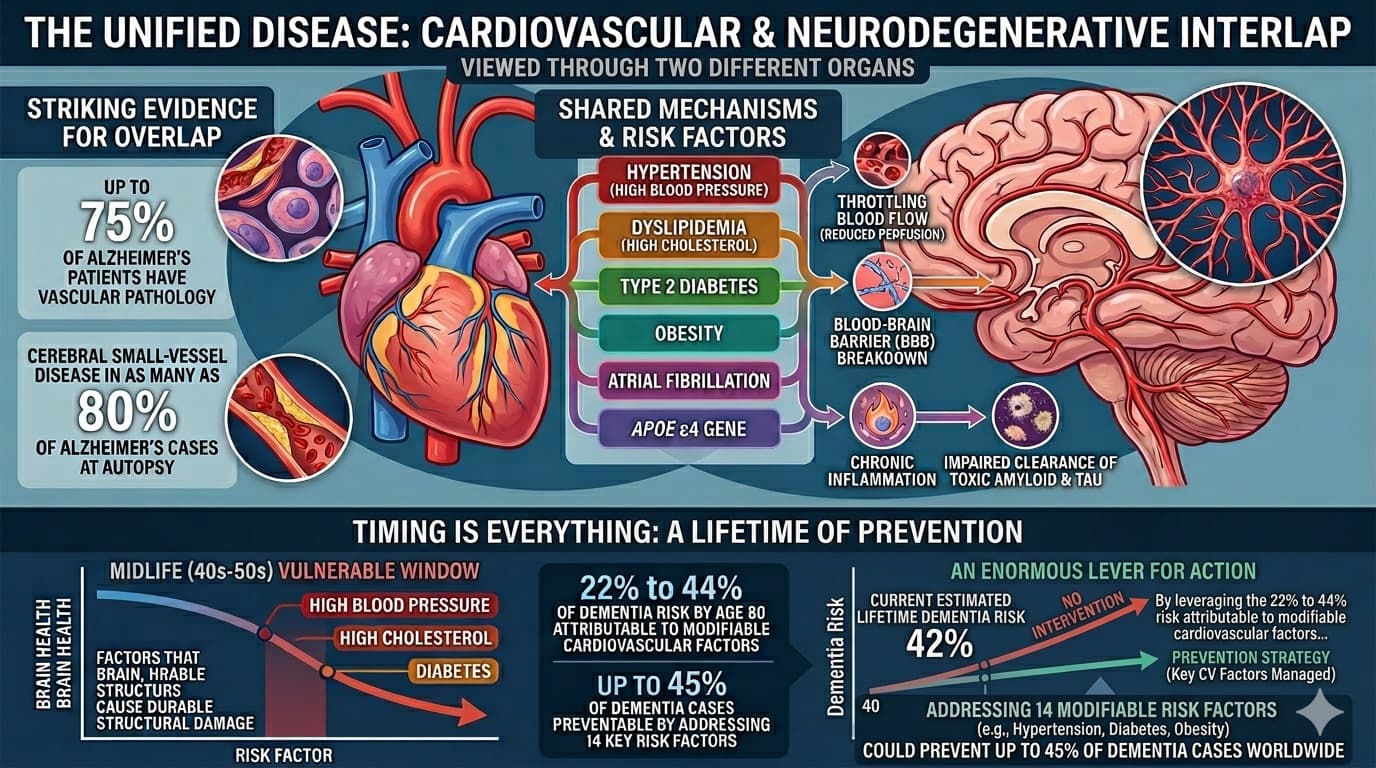
The evidence for overlap is striking. Up to 75% of people with a clinical Alzheimer’s diagnosis also carry vascular pathology in the brain, and cerebral small-vessel disease shows up in as many as 80% of Alzheimer’s cases at autopsy. The shared culprits — hypertension, dyslipidemia, type 2 diabetes, obesity, atrial fibrillation and the APOE ε4 gene — don’t just travel together; they act on the same machinery, throttling blood flow, breaking down the blood-brain barrier, igniting chronic inflammation, and impairing the brain’s ability to clear toxic amyloid and tau.
The numbers that make this actionable are the modifiable ones. The authors cite estimates that 22% to 44% of dementia risk by age 80 is attributable to modifiable cardiovascular factors, and that up to 45% of dementia cases worldwide could be prevented by addressing 14 known risk factors. Against a lifetime dementia risk now estimated at 42%, that is an enormous lever.
The “Big Idea” is not merely that prevention works — it is that timing is everything. Earlier is better. Midlife is the vulnerable window: high blood pressure, high cholesterol and diabetes in your 40s and 50s do durable structural damage. Yet the same review warns that in late life the script flips. Blood pressure that is too low (under 90/60), or overly tight glucose control can result in hypoglycemia risks, producing a U-shaped curve where both extremes can harm the aging brain.
The authors push toward precision prevention: replacing one-size-fits-all targets with individualized risk scoring (CAIDE, CogDrisk), genomics (APOE), and an emerging panel of blood biomarkers — p-tau217, p-tau181, GFAP, neurofilament light — that promise to track brain aging the way a lipid panel tracks heart risk. They also single out apoB as a more honest measure of atherogenic risk than LDL-C alone.
The take-home is a paradigm shift rather than a pill: treat the vascular system early and intelligently, and you may be running the single best dementia-prevention program currently available.
Actionable Insights
The practical message: protect your vasculature in midlife and you measurably protect your brain. Magnitudes the paper supports:
- Move. Regular physical activity is associated with ~20% lower all-cause dementia risk, ~14% lower Alzheimer’s, and ~21% lower vascular dementia; in older adults, activity tracks with 30–40% lower vascular-dementia risk. Resistance training showed 12–18% gains in cognitive control/memory. Against a 42% lifetime baseline, a 20% relative reduction implies roughly a 33–34% absolute lifetime risk — a ~8 percentage-point drop.
- Eat MIND. MIND stands for Mediterranean-DASH Intervention for Neurodegenerative Delay . It’s a hybrid of two established heart-healthy eating patterns: the Mediterranean diet and the DASH diet (Dietary Approaches to Stop Hypertension). It was designed specifically to target brain aging, not just cardiovascular risk. In practice it emphasizes foods rich in vitamins, carotenoids, and flavonoids — leafy greens, other vegetables, berries, nuts, whole grains, olive oil, beans, fish, and poultry — while minimizing saturated fat, red meat, butter, cheese, fried food, and sweets. Adherence to the MIND diet was associated with slowing brain aging by up to 7.5 years.
- Control apoB/LDL in midlife. Each 1 mmol/L (~39 mg/dL) higher LDL-C ≈ 8% higher dementia incidence; midlife high cholesterol ≈ +14% all-cause dementia and roughly doubled mild-cognitive-impairment risk.
- Treat diabetes and blood pressure early. T2D carries a 50–60% higher dementia risk; GLP-1 receptor agonists were associated with 31–45% lower dementia risk versus older agents.
- Don’t smoke (30–40% higher dementia risk; only full cessation helps). Limit alcohol to <1 drink/day.
Caveat: most numbers are associations from observational data, so real-world personal benefit is plausibly smaller.
Source:
- Paywalled Paper: A Preventive Neurology Perspective on Promoting Brain Health and Preventing Cardiovascular Disease , Published 2026 May.
- Institutions: Institute for Neurodegenerative Diseases (Boca Raton, FL); University of Michigan Medical School (Ann Arbor, MI); Early Medical (Bee Cave, TX); Department of Neurology, Weill Cornell Medicine (New York, NY).
- Country: United States.
- Journal: Clinics in Geriatric Medicine (Elsevier).
- Impact Evaluation: The 2024 Journal Impact Factor for Clinics in Geriatric Medicine is 3.39 (SJR 1.027; h-index 94; quartile Q2 within Geriatrics & Gerontology). 3.39 is low on the absolute 0–60+ general-science scale, but this is a specialty review journal(curated, invited clinical reviews)
Related Reading:
- The 115-Year-Old Brain That Escaped Aging: Supercentenarian Autopsy Challenges the Inevitability of Cognitive Decline
- The Brain's Broken Plumbing: Why Diminishing Blood Flow Drives Dementia
- The Vascular Pacemaker: How the Secretory Engine of Aging Arteries Synchronizes Whole-Body Decay
- Cardiovascular Health 2026
- The Arginine Paradox Solved: Why Citrulline is the Superior Vascular Anti-Aging Agent
