Thanks RapAdmin,
Yes, I was wondering if it was the trough that was perhaps more important, ensuring a low enough dose to not activate mTOR 2.
I know Dr Green has suggested to go for 5 halvings from the peak, and I know the minimum trough value that transplant patients are meant keep above is 5ng/mL. Presumably this is because at least 5ng/mL is required to keep mTOR2 activated (which is what a transplant patient wants).
Allowing for some graduation this suggests to me you’d want well under 5ng/mL for the trough for anti-aging e.g. <1ng/mL.
On that logic I’m puzzled that 6mg weekly seems to be the ‘standard’ dosing.
I took 20mg and got 34ng/mL (no grapefruit juice). This suggests (for me at least) 1.7ng/mL per 1mg.
So (if the dose to blood level works linearly) 6mg would give (me at least) a peak level of 10.2 ng/mL.
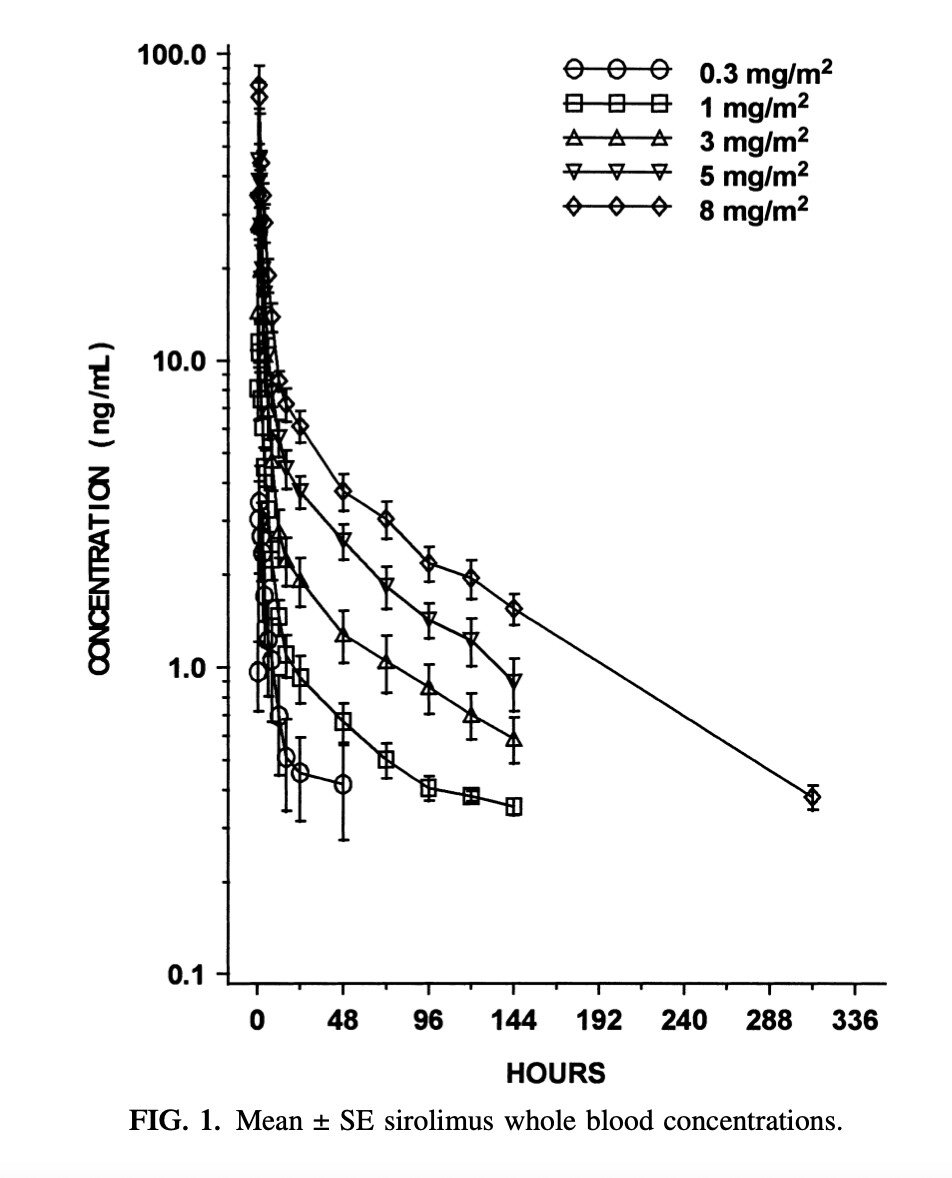
I understand half-life of sirolimus is considered to be about 60 hours (although some have suggested could be 80 hours in non-transplant patients). This means 7 days would give 2.8 half-lives, which means a trough of 14% peak levels. If peak levels were 10.2 then this gives a trough of 1.5 ng/mL. This is below 5ng/mL, but not much below and doesn’t leave much room for error. For example if the half-life is actually 80 hrs the trough will be 2.4ng/mL.
If someone actually takes 10mg a week (as I understood nearly 10% of survey respondents said they did) then the troughs would be 2.5ng/mL (or 4ng/mL with 80 hrs half-life). Very close to the level for keeping mTOR2 activated.
However, if you were to take 12mg (or 20mg) fortnightly, the trough changes dramatically to 0.4ng/mL (instead of 1.5ng/mL) and in the worst case above, to 0.7ng/mL (instead of 2.5ng/mL).
This seems a much safer ‘stop activating mTOR2’ level to me.
2 weeks is the only way to get Dr Green’s recommended 5 halvings (5.6 at 60 hrs, 4.2 at 80 hrs).
Of course, perhaps my blood conversion level of 1.7ng/mL per 1mg of sirolimus is unusually high.