A weekly dose is what the Mannick study in 2014 found was safe and effective in humans. It’s posted in various places in these forums, but essentially 5mg once weekly was the most effective dose of three regimes tried.
Those who take rapa every fortnight seem to be taking larger does. 20mg or more. At those levels you need two weeks to cleanse it from your system, generally speaking. People who take these large doses say they do so because in the mice studies more rapa leads to more health extension and more life extension. And even more seems to lead to even more.
Thus, some experts suggest you should take the largest dose your body will tolerate without side effects. Indeed, many here have said that they keep increasing the dose over time with their upper limit being whatever causes side effects.
So you have two philosophies here.
One is to follow what has been tested as safe and effective in humans and trust the long road, where this use over years and decades will accomplish what is desired in the cells. Dr. Attia and Dr. Kaeberlein are both around 6-8mg week last time I checked. This approach seems to be followed by more people in middle age.
The other is to work up to the largest dose your body can handle, dosing at a probably two week interval. Several doctors seem to follow this approach. In my observation they are older than average, in their 70s and 80s. My guess is that they feel they have little to lose and lots to gain from high doses. Also, one of these doctors (Green?) takes a drug with competing properties on the off week; thus his two-week pattern.
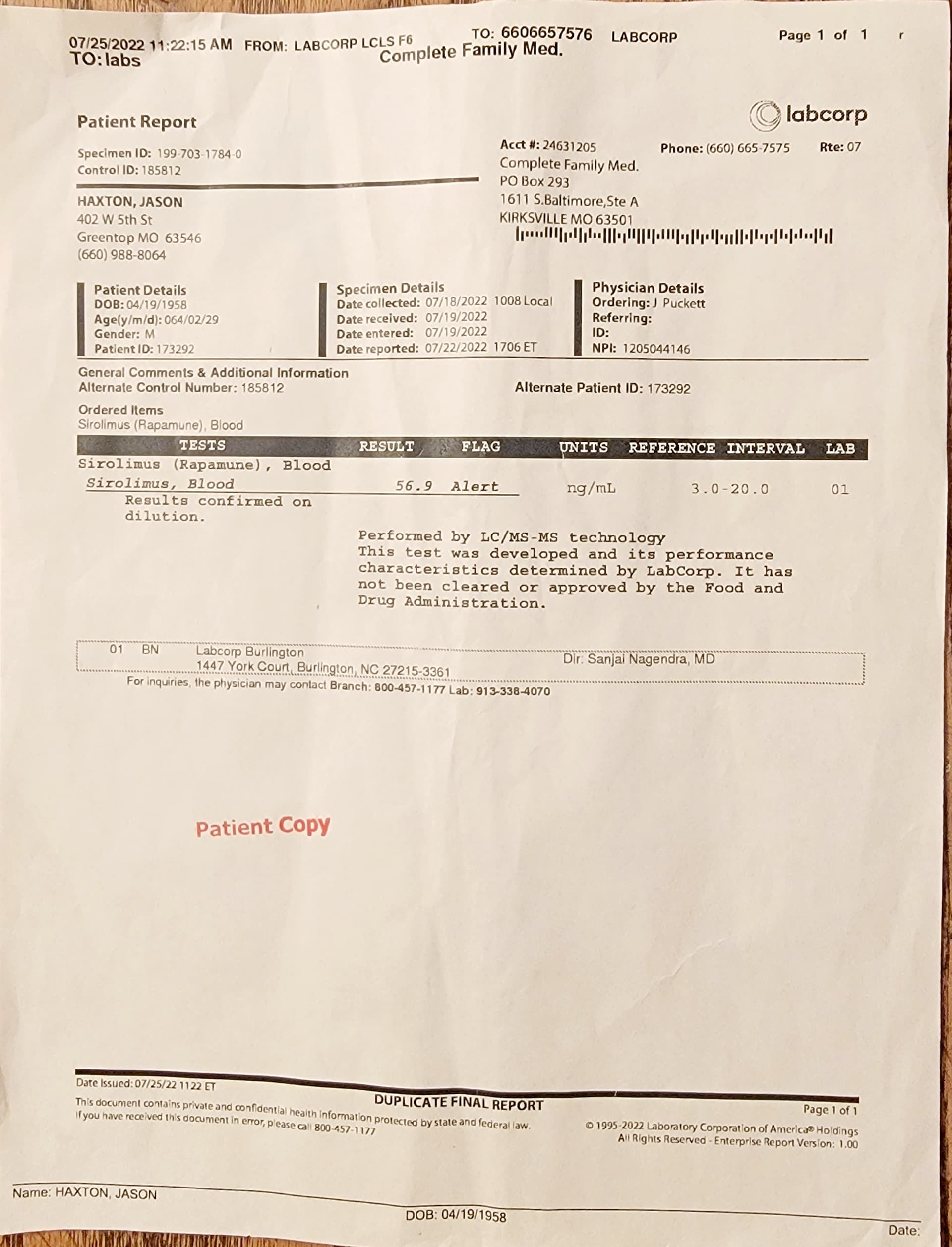
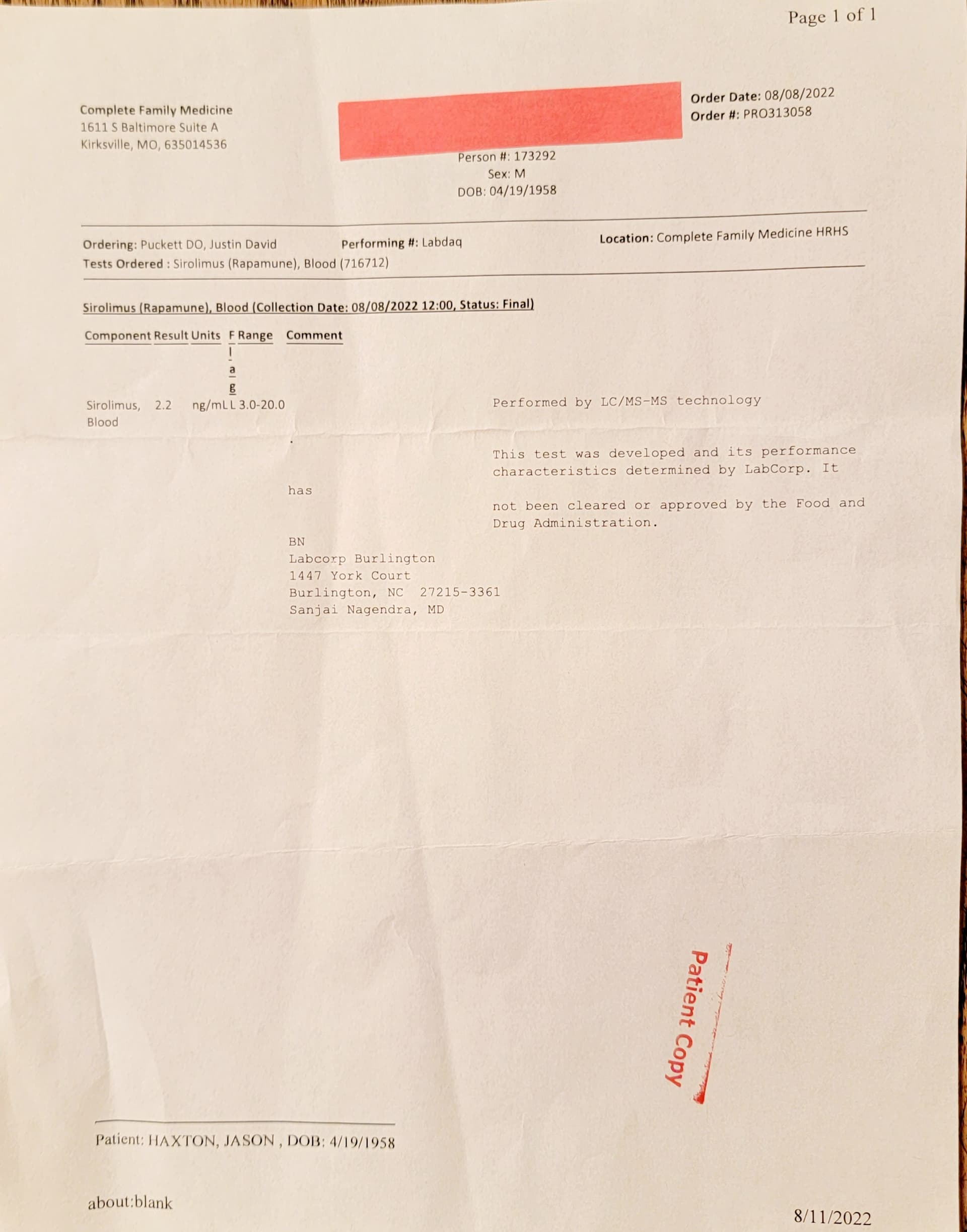
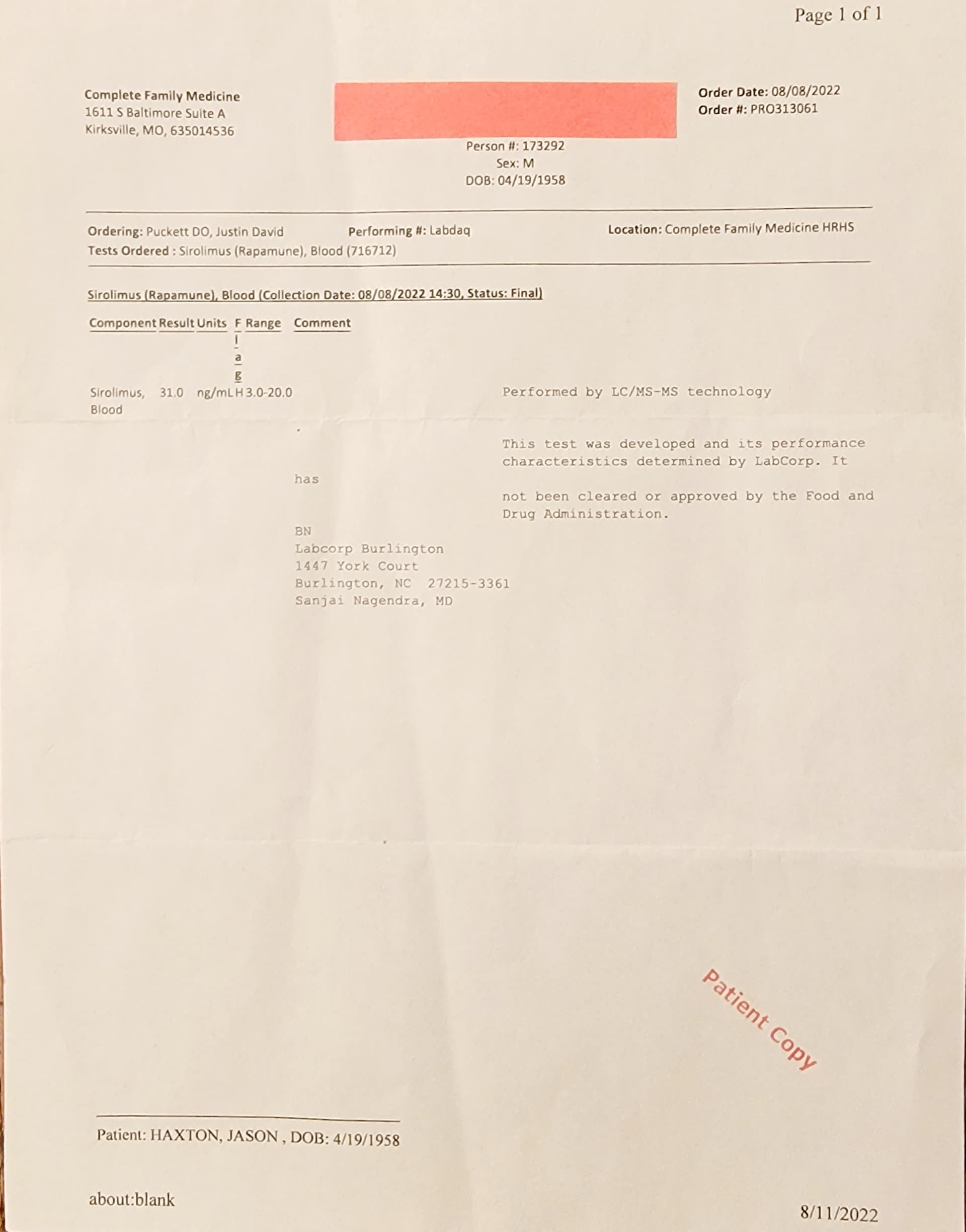
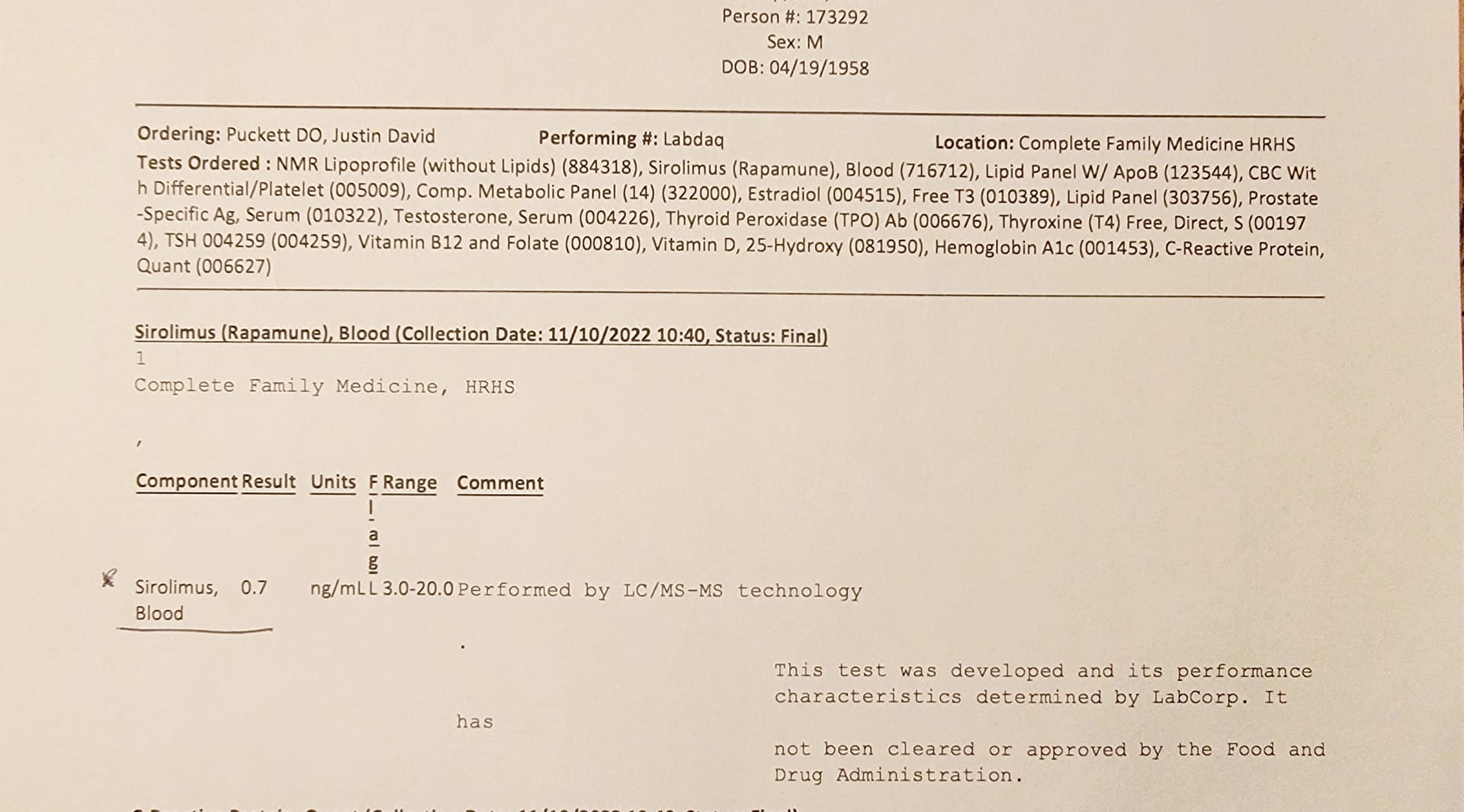
Finally, you asked about the half-life’s. It seems that moderate doses get to a low enough level in one week, while high doses need two weeks to get to the same low level. Note that some people say it’s not a week, but 6 days, or 10 days, or 12 days. As humans we’ve adopted a weekly schedule, so dosing in weekly terms is most convenient and easiest to maintain.
Again, I’m not a doctor, just a close reader who has been consuming this content constantly for the past little while. Everyone is experimenting on this front, so as they say in the States, you do you.