The associations were separately observed among women (0.78 [0.72 to 0.84]) and men (0.90 [0.83 to 0.98]), individuals aged ≥ 65 years old (0.82 [0.78 to 0.87]) or < 65 years old (0.84 [0.70 to 1.00]), and in those initiating semaglutide (0.75 [0.67 to 0.84]), liraglutide (0.77 [0.70 to 0.84]), or dulaglutide (0.82 [0.77 to 0.88]). The hazard ratios for dementia, Alzheimer’s disease, vascular dementia, and Parkinson’s disease onset were 0.76 [0.72 to 0.81], 0.77 [0.68 to 0.87], 0.75 [0.67 to 0.85], and 1.04 [0.93 to 1.17] with GLP-1 RAs versus DPP4i, respectively.
That first study about CV risk getting worse after discontinuing GLP1’s really missed a golden opportunity not checking if those patients gained weight back once they stopped so we can have a better idea of whether their CV risk got worse because they gained the weight back or just because they stopped the drug itself.
We previously demonstrated in preclinical models that the triple incretin agonist retatrutide (RETA, LY3437943) significantly reduced PDAC tumor burden, yielding a 14-fold reduction in tumor volume compared to a 4-fold reduction with the single GLP-1 receptor agonist semaglutide. Remarkably, the anti-tumor effects of RETA persisted after treatment discontinuation and weight regain, suggesting tumor-intrinsic or immunometabolic mechanisms independent of weight loss.1 Motivated by these findings, we investigated whether RETA administered at a subtherapeutic dose insufficient to induce weight loss could achieve anti-tumor efficacy comparable to anti-PD-1 therapy
Low-dose RETA significantly reduced tumor volume by 3-fold compared to vehicle, demonstrating efficacy comparable to anti-PD-1 monotherapy, which achieved a 5-fold reduction in tumor volume. With a 4-fold reduction in tumor volume, RETA + anti-PD-1 combination therapy did not demonstrate significant additional benefit beyond either monotherapy. Importantly, body weight remained stable across all groups, while blood glucose levels were significantly lowered by RETA treatment, indicating RETA’s anti-tumor effects occurred independently of weight loss and may involve metabolic modulation.
This is very old, and inaccurate. Attia has since walked back these statements. Lean mass loss is a function of weight loss rate, it doesn’t have much to do with GLP1 use. You can expect to lose at least 66% of fat mass of on a GLP1 if you don’t go too crazy trying to lose more than 1% of your body weight. This is comparable to other weight loss methods.
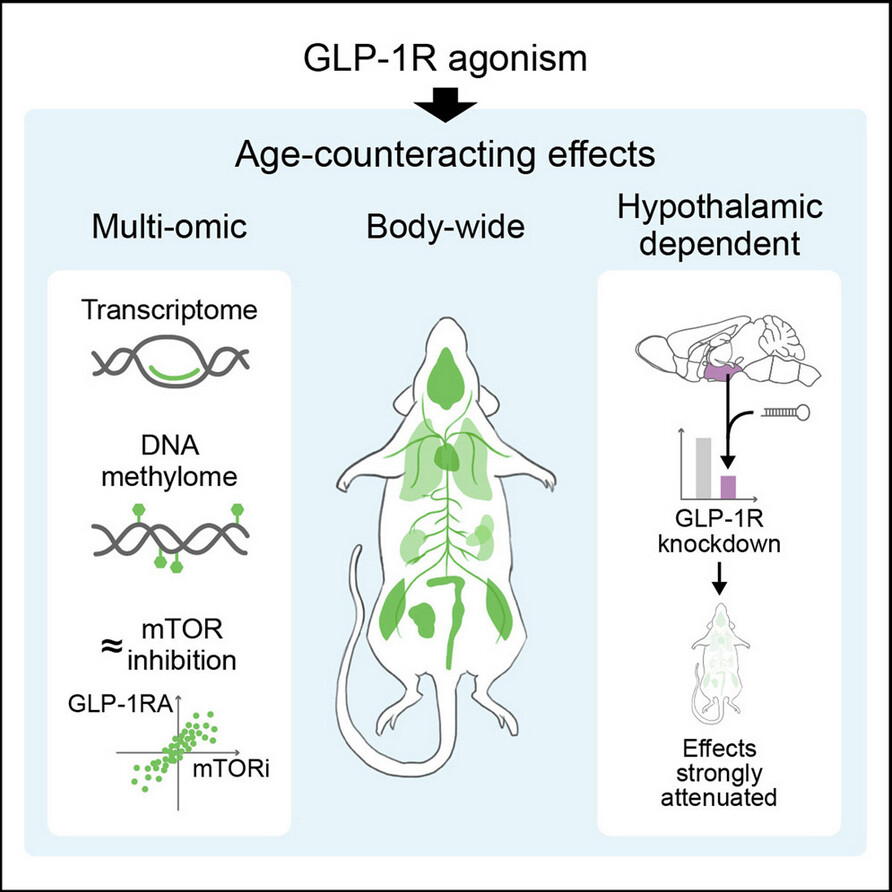
Identifying practical ways to counteract aging and associated degenerative disorders is urgently needed. We performed deep molecular profiling and functional assessments in aging male mice to show that glucagon-like peptide-1 receptor agonist (GLP-1RA) treatment broadly counteracts age-related changes. In mice treated with a GLP-1RA from 11 months for 30 weeks, we observed strong body-wide multi-omic age-counteracting effects and improved selected physical functions. Importantly, the effects were specific to aged mice, not young adults, and were attained with a relatively low dose that minimally affected food intake or body weight. With GLP-1RA treatment beginning at 18 months for 13 weeks, the molecular age-counteracting effects were even stronger and largely dependent on hypothalamic GLP-1R, pointing to a brain-body axis of aging modulation. Comparison with mammalian target of rapamycin (mTOR) inhibition, a proven anti-aging strategy, revealed strong multi-omic similarities. Our findings have broad implications for the mechanisms behind GLP-1RAs’ pleiotropic benefits, guiding clinical trials, and informing development of anti-aging-based therapeutics.
At 1 mg of retatrutide per week, I lost about eight pounds from a frame with little to lose. I went down from 138 to 130, and the loss was all fat, not muscle. I didn’t take it to lose weight but rather to increase my GFR, which I haven’t tested yet. In any case, it looks like I gained muscle–not in bulk but in definition.
I don’t want to lose any more weight, so I reduced my weekly dose to 0.5 mg per week. I’ll check on the GFR in a week or so.
I wouldn’t worry about the eGFR as it bounces a round a lot day to day from a lot of factors. (unless it’s really critically low). I’d check the far superior Cystatin C kidney test to know how your kidneys are really doing.
@LukeMV (or anyone for that matter) you seem like you’re well versed (one of many great minds on these boards) when it comes to health indicators and which one matters more or less, and I have a specific issue/question.
I did my blood work last week and one of the areas of concern was the fact that my Anion Gap was out of range at 15 from 13 last year. Anecdotally the only thing that I could make any connection to it going out of range was the fact that I’ve been doing Tirzepatide for last 9 months or so and during this period I’ve experienced uncomfortable levels of acid reflux plus some uncomfortable (almost constantly) pain on my lower back on both sides of the spine but I little more so on the right side, which I’m guessing might have to do with a kidney issue thus concerned about Anion Gap. All my other markers (except my lipids, but that’s an easy fix with meds that have been expansively discussed on these boards) were optimal or normal.
My question is, would you know of a remedy for bringing Anion Gap back to normal? As a footnote, I did stop all GLP1’s for about 2 months (a while back) and the pain on my lower back went away almost entirely, so in worst case scenario I will just quit Glp1’s but I do like some other benefits I seem to have from Tirze or Reta (i.e. less inflammation, lower overall Glucose, and the big one appetite suppression).
Thanks,
From what I know about anion gap, it can easily be thrown off from a recent workout (I have experienced this several times so I never really pay much attention) or mild dehydration so if it’s mildly high, it probably isn’t something to really worry about if all your labs look normal otherwise. Other than that, I don’t want to play expert on Anion Gap. If there are other labs that could show you’re in lactic acidosis or ketoacidosis, then I would be more worried. As far as I’m aware, I don’t know if there is some kind of supplement or anything that can make the number look how you want it to look.
Thanks. I might be overthinking it (to connect the lower back pain to anion gap) so I guess I’ll just keep an eye going forward. I’ve had some amazing relief from LDN on pains everywhere in my body, but more specifically my lower back pain, as well as reduction of acid reflux, so I’ll continue with it for a while and see what happens.
You might want to try a low dose of Cagrilintide. I’ve found it to be an effective appetite suppressor. We have been slowly ramping up from 0.1mg weekly to 0.3mg in conjunction with Reta, will probably go to 1.0mg over the next few weeks. Our Reta dose is fairly low 2.5mg weekly and the appetite suppression at that dose is moderate. I’d like a bit more to curb the “munchies” in the evening after our THC dose
We are both maintaining ideal weight but the munchies win out too often LoL! That is one of the benefits of Reta, a bit of overeating is easily handled by Reta. I’d just like to have a bit more self control LoL!
A couple months ago we tried 1.0mg for 2 weeks and it completely killed our appetites. Had to really focus on food to even eat enough. Did not like it and stopped after the 2 weeks. That’s why we re-started with such a low dose, I’d like to sneak up on the most comfortable and effective dose.
eGFR (estimated glomerular filtration rate) can be obtained via creatinine, cystatin C, or a combination of both using the CKD-EPI equations. So you definitely want to watch eGFR, but deriving it from cystatin C is superior in multiple ways, especially if you do a lot of exercise training, carry a lot of muscle mass, and/or take creatine supplements.