Unfortunately, Sigma Audley was put out of business about a month ago. I’m sure the will now need to find a reliable second tier Chinese supplier and get 3rd party testing in place.
3 Likes
@BGpharmaceuticals I think your peptide page needs to be updated then for tirzepatide and retatrutide.
1 Like
I chose the cheapest “pending A-rated” single-vial source at the time: Peptide Crafters. For bulk I chose the cheapest “pending A-rated” source: Shanxi Qianyecao Biotech QYC.
1 Like
I think Ive seen close to enough to warrant switching from high dose acarbose to reta. I’m guessing no one taking jardiance (or any sglt2), a glp-1 and serious acarbose usage? might be overkill on the blood sugar. Acarbose has more studies behind it, so I still feel uneasy about it, but reta seems to be a nice substance, and many like the glp-1/glycine combination together
I take all three. 2mg Reta weekly, 150mg acarbose, and 10mg empagliflozin. A1C dropped to 4.9.
2 Likes
that may be it, scale back the acarbose… there were times when jardiance and high dose acarbose alone had me on the border (but I take other stuff in my stack that can also lower blood sugar)… I might just do 50-150mg of the acarbose, even though I believe the studies on longevity for acarbose was high dose in the famous trials?
https://www.medpagetoday.com/meetingcoverage/chest/118129
For obese patients with asthma, GLP-1 receptor agonist use was associated with substantially reduced risks of exacerbation and steroid use, a retrospective comparative outcomes analysis showed.
For type 2 diabetes patients with OSA, GLP-1 receptor agonists were associated with reduced risk of intubation compared with DPP-4 inhibitors (HR 0.603, 95% CI 0.548-0.664) and metformin (HR 0.814, 95% CI 0.73-0.906), reported Martin Borissov, MD, of the University of Maryland School of Medicine in Baltimore.
New-onset COPD was also less likely for GLP-1 drug users compared with metformin (HR 0.886, 95% CI 0.838-0.936) and sulfonylureas (HR 0.812, 95%CI 0.777-0.848). No differences were seen compared with SGLT-2 inhibitors or thiazolidinediones (TZDs).
GLP-1 receptor agonists were also associated with a little less risk of new-onset hypertension and atrial fibrillation compared to other diabetes medications, Borissov reported in a second presentation at the same session.
1 Like
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(25)01375-3/fulltext
The cardioprotective effects of semaglutide were independent of baseline adiposity and weight loss and had only a small association with waist circumference, suggesting some mechanisms for benefit beyond adiposity reduction.
In those receiving semaglutide there was no linear trend linking weight loss at week 20 to subsequent MACE risk, but greater waist circumference reduction at week 20 was associated with lower subsequent MACE risk, and waist circumference reduction by week 104 was associated with lower in-trial risk of MACE. An estimated 33% of the observed benefit on MACE was mediated through waist circumference reduction (HR 0·86 [95% CI 0·77–0·97] after adjustment for time-varying changes in waist circumference).
2 Likes
I think quite high doses are required for asthma and OSA control. Not sustainable. I’m finding the maintenance dose of tirzepatide to not control them.
What I personally have found, if your A1C is already good, interestingly, the 3 of these don’t do much to it. I was worried mine might go too low, but after checking AI, I saw that my experience was not unique (caveat, if I used a higher dose of Reta, perhaps it would be different?).
I take 150mg ish of acarbose and dapagliflozin. My guess is my low/random Reta usage is probably not enough to have any blood sugar lowering effects, but I don’t know. I take aprox 1mg but not necessarily every week.
Even with these, my post prandial glucose spikes are not too low, but my baseline is crazy high.
I started out with an A1C of 5.1… it remained that way on almost a year of taking these things, but my labs last week showed it moved to 4.9 .
3 Likes
Well, I took all that (25mg Empagliflozin, 5mg/week Tirzepatide, 100mg acarbose at the start of each meal + low carbs diet) and my HbA1C and fasting glucose are still too high so I’ve added some Pioglitazone in the mix. I will report back after my next blood tests.
4 Likes
They work in completely different ways, and I believe a lot of acarbose’s benefits also come from modulating the gut microbiome.
2 Likes
Yea they all reduce A1C but there is a floor on how long it will go, fortunately. That’s why it’s also very unlikely to be hypoglycemic by taking these either.
1 Like
Yeah, it creates a lot of farts.
2 Likes
Decidedly not beneficial to one’s coworkers/spouse/friends.
2 Likes
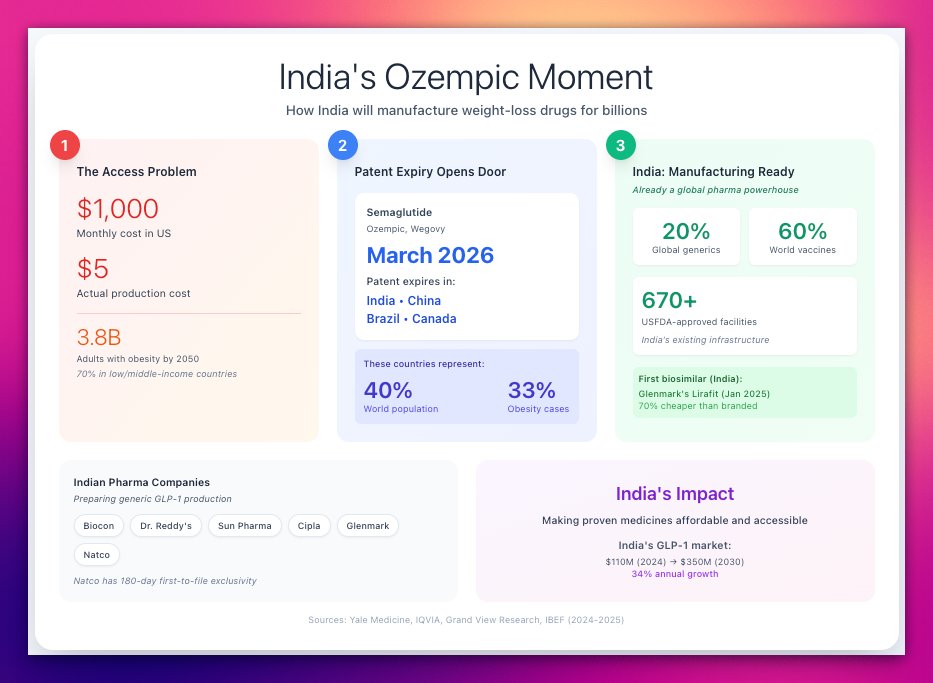
This is interesting, most of the peptide manufacturing comes from China, so it will be interesting to see how both nations make progress there.
NY Times
Obesity Drugs May Drop to as Little as $150 a Month
President Trump announced a deal with Eli Lilly and Novo Nordisk to lower prices on hugely popular weight-loss drugs for Medicare, Medicaid and American patients who pay with their own money.
Story a bit more complicated, see full article, but hopeful.
3 Likes
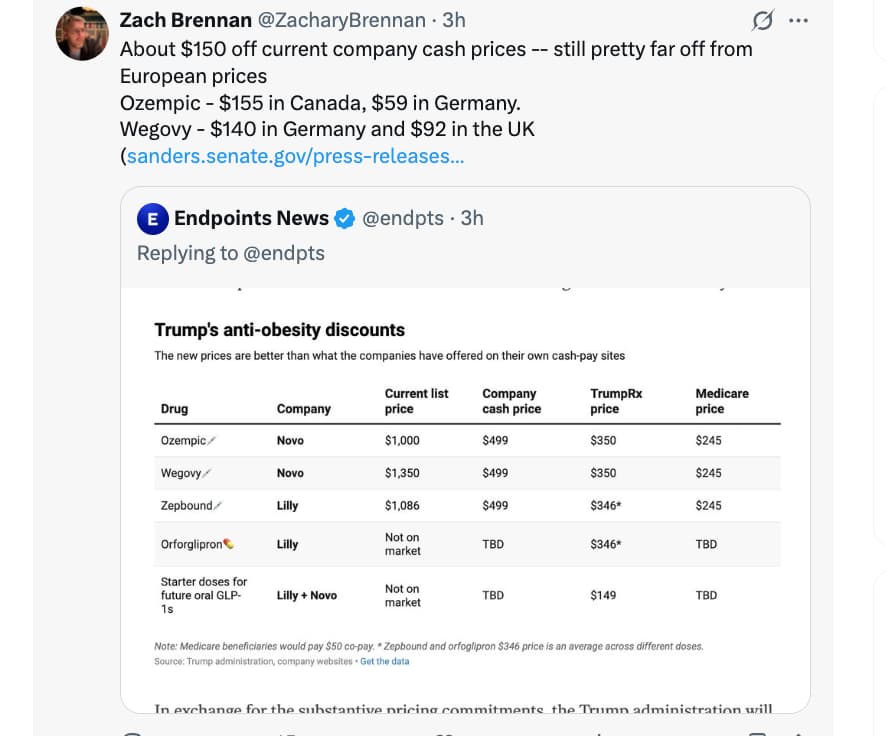
And “as low as 150/mo” for the lowest dose.
1 Like