Interesting. I appreciate the data on this.
3 Likes
Was just reviewing an interview with the Novartis exec Lloyd Klickstein who was involved with the everolimus tests and the research papers related to this topic. In the interview they mention what they believe is the dose equivalency of everolimus to sirolimus / rapamycin - see below:
In one experiment. Patients with polycystic kidney disease that were otherwise healthy, took the rapalog (RAD001) and a substantial fraction saw these biochemical changes in their blood
- The dose was 5 to 10 mg a day (equivalent to 2-8 mg of rapamycin)
4 Likes
Perfect. Thanks for the followup with those numbers. It gives me a good comparison to start at.
2 Likes
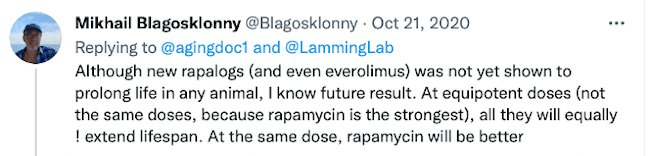
This just in today from one of the leaders in rapamycin research - no preference for rapamycin or everolimus (see tweet below). I’m going to a more in-depth analysis on the dosing and pricing comparison - will post in the next few days:
8 Likes
Good summary of side effects of everolimus:
https://chemocare.com/chemotherapy/drug-info/everolimus.aspx
3 Likes
Interesting - but misleading. Those are the side effects seen seen in the high daily doses seen in applications for cancer therapy, etc. - not the side effects seen in the weekly dosing (or once every two weeks) that is typically used in anti-aging applications.
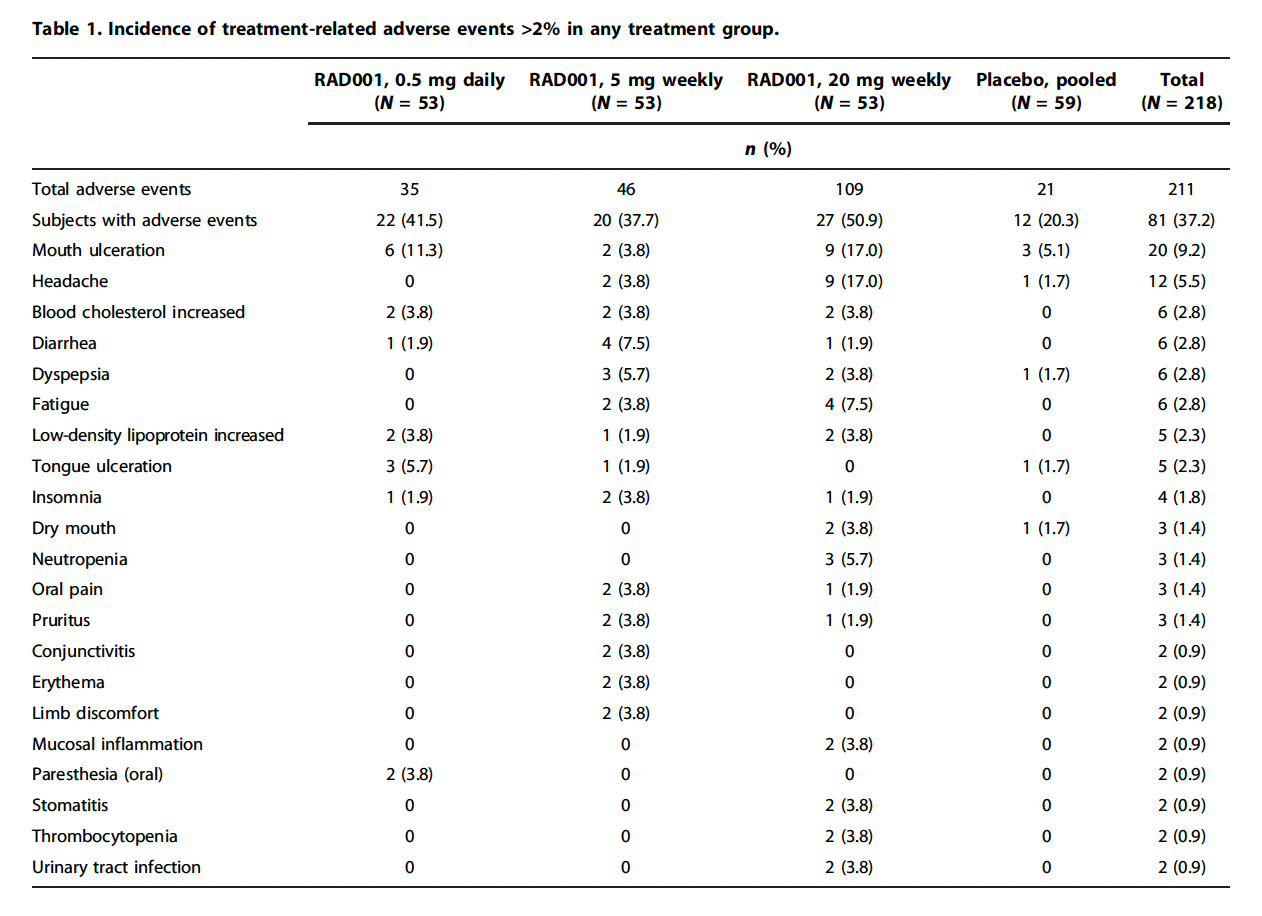
Here are the side effects seen with Everolimus (RAD001, Novartis Afinitor) in the famous Mannick 2014 clinical trial (with elderly but healthy people, dosed weekly) where it was shown to improve aging immune systems in people.
Interestingly, they reported only 1 serious adverse event in the study:
Only one severe adverse event was assessed as related to RAD001: mouth ulcers in a subject treated with 20 mg weekly RAD001.
2 Likes
Here is the packet insert for Everolimus / Afinitor (for cancer, etc. applications with daily dosing) with all the detailed product information that people might want to review, (note, all side effect info different from seen in weekly, anti-aging dosing protocols):
3 Likes
28 hrs half-life is attracting.
Sirolimus takes approximately 13 days to clear its concentration under 3%, while Everolimus only takes about 6 days, that’s a big difference
Do you know anyone in aging field using Everolimus instead of Sirolimus?
4 Likes
I’ve not heard of anyone in aging field using everolimus yet. I brought up the issue a year ago when the drug was starting to become available as a generic in India inexpensively and you can see the discussion below. Blagosklonny was interested. I think it may make sense to at least alternate with everolimus, if not go exclusively everolimus.
Also - it will be a lot easier to import higher quantities of everolimus because it comes in 5mg and 10mg tablets. In the USA - if you import 360 tablets (a reasonable number to get in for personal use, and usually not a Customs/border problem), with rapamycin / sirolimus you only get 360 mg total, whereas with everolimus @ 10mg, you get 3600mg of the drug. Even thought everolimus needs to be dosed at a slightly higher level for dose equivalency, its still easier to import in higher quantities.
The only caveat is that I’ve not seen any 3rd party lab analysis on everolimus product the different Indian manufacturers of everolimus and therefore have no idea about the quality, purity and contaminants.
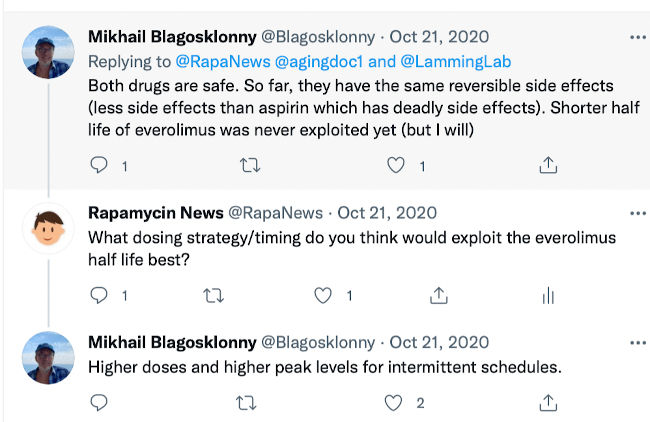
Though, one doctor focused on aging, has said this:
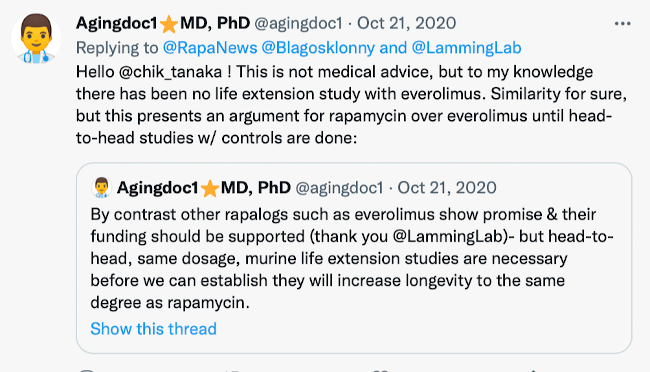
More of the twitter thread here:
4 Likes
Just noticed this important bit of information on everolimus in the new clinical study announced by Dr. Bradley Stanfield this week:
Selection of orally bioavailable Rapamycin Analogue
Pure Rapamycin has poor bioavailability, which lead to the development of the rapalogs: Sirolimus and Everolimus. Everolimus is a second generation Sirolimus derivative specifically developed to have improved pharmacokinetic properties including, but not limited to, facilitated oral formulation, higher oral bioavailability and better metabolic stability in comparison to sirolimus. As these regions of the Sirolimus and Everolimus molecules are structurally similar, it was hypothesized that both molecules have the same effects on the mTOR pathway, however this is not the case. Like Sirolimus, Everolimus inhibits mTORC1, but at the clinically relevant concentrations tested, Everolimus was much more effective at inhibiting mTORC2 [27].
It is important to note that the lifespan-enhancing effects of mTOR inhibitors have been linked to mTORC1 inhibition, whereas inhibition mTORC2 might even be detrimental, because mTORC2 controls insulin-mediated suppression of hepatic gluconeogenesis [28]. Therefore for this proposed trial, Sirolimus is the preferred rapamycin analogue as it does not inhibit mTORC2 to the same extent as Everolimus.
Relevant research papers:
and
5 Likes
Useful information that Everolimus affects the mTOR pathway differently than sirolimus and has a higher potency in terms of interacting with mTOR complex 2
Does that means it’s better stick in sirolimus
1 Like
Yes, probably not a bad idea to just stick with sirolimus for now. Its only one research study, and no full lifespan studies have been done with everolimus, but it seems that sirolimus is a slightly lower risk approach than everolimus. If I already had everolimus I would still take it, but I’m a little less enthusiastic about everolimus now that I’ve seen that data.
6 Likes
The following is quoted from FrankT.Hippo posted in LongeCity forum 2020:
I haven’t been following this threat for a while, but I wanted to give an update in case anyone was interested in this data point:
I have a poorly characterized mitochondrial disorder (“disorder of mitochondrial respiratory chain complexes”). I was in bad shape in January 2017 when I came across this thread and came into contact with Jaris.
Soon after, I started low doses of rapamycin. My condition has since stabilized and I am substantially more functional.
I was even able to travel a bit, something I have not been able to do for a decade.
I was taking Sirolimus prior, however that had terrible side effects. I have since switched over to Everolimus*, which I find much more tolerable.
Of note, I have had to increase doses to achieve the same effect, but I am still at relatively low doses (5 mg / once every three weeks).
I am going to try to boost the dose up to 10mg. I will let you know how that works.
*Note, Everolimus is Glenmark brand from India.Moreover, for whatever reason, I can tolerate the Everolimus much better. With sirolimus I am usually bedridden for a week while dosing: no energy, flu-like, weak, headaches, etc…-- but then I recover and in the following couple of weeks I feel improved relative to my baseline. I would compare the feeling to what I imagine chemotherapy to feel like. However, I will look into it.
Dec 2021-----------------------------------------------------------------------------------------------------
I have been following this thread for several years and have been taking rapamycin too.
I have a clinically diagnosed mitochondrial defect – seemingly due to a PINK1 and OPA1 mutation – which is disabling.
Sirolimus was a miracle drug for about 3 years – i was super productive with my behavioral genetics research – but the efficacy dissipated.
It is really hard to modify these conditions; nothing has panned out and my Harvard trained biomedical geneticist was somewhat black-pilled last I talked to her. So, I have realistic expectations. And in light of those, rapamycin was a stellar success.
I tried Everolimus but as predicted by those on this forum that did nothing.
I still take Sirolimus on and off but is has less potency – maybe the condition has just advanced — so I have moved on to trying other drugs including Semax, dihexa, and similar peptides to upregulate BDNF.
I am now procuring an order of SKQ1 a newly developed mitochondrial targeted anti-oxidant – since I had good experiences with MitoQ and CoQ10. And I am also experimenting with intravenous glutathione.
3 Likes
Oh I can imagine the shorter half-life to be super useful at least when it comes to exercise training and performance.
I also sometimes wonder (based only on subjective feeling) if most of the benefits of rapa are in the first day or two, and rest of time is spent on waiting for it to wash out. If that is the case, then everolimus maybe a better candidate.
High doses may also come with less side-effects if there’s a shorter half-life. It’d be somewhat of a hit and run strategy then.
7 Likes
Another potential advantage that comes to mind is that oral everolimus may have different tissue specificity when compared with rapamycin. In this scenario, alternating between the two every few months (or maybe combining them) may be a good strategy to distribute the benefits throughout the body.
3 Likes
hello, could you please tell me what brand of Everolimus did you used?
1 Like
Hi Lui, welcome to the forum and thanks for posting.
I’m thinking of adding everolimus the next time I order my rapamycin. Here are some quotes I got - see this post.
Also - I’ve recently added a list of the generic manufacturers of everolimus on this page listing all the companies offering everolimus generic medications.
1 Like
its called Evermil 5mg, made by Glenmark of an Indian pharmacy
2 Likes
thank you very much!
1 Like