Would agree with what you’ve briefly summarized. Also some indication Everolimus better at crossing BBB. Is perhaps taking more frequently a con? The harder TOR2 perhaps at very high doses…cancer/transplant, not at lower doses? Dysregulating TOR2 would more amplify side effects, including TOR2 specific insulin signalling/hyperglycemia. Of the comparative studies, not many report higher hyperglycemia with Everolimus…but similar range of side effects as rapamycin.
Re cost, I was quoted by an Indian supplier $0.7/mg for Rapamycin ($7 for 10 x 1mg/tabs), and Everolimus $.95/mg ($95 for 10 x 10mg tabs). If you’ve got to take 2X the Everolimus dose for same potency, then effectively $1.80/mg vs $0.70/mg, 250% more. On a total cost basis over a year if it really increased lifespan…meaningless.
It’s slightly better side effects profile, that could be the lure/incentive.
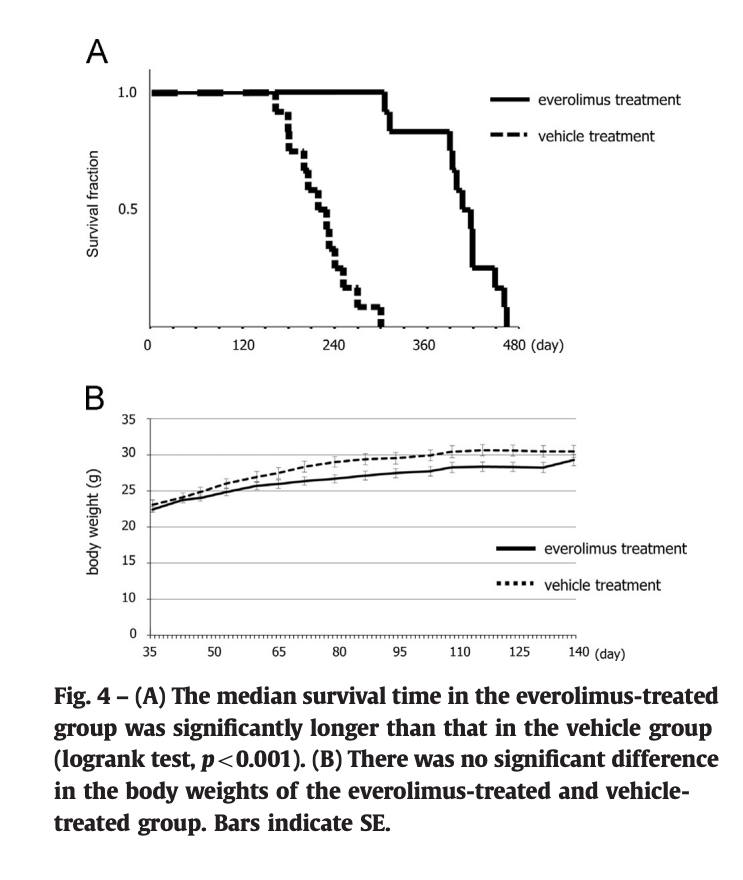
I’ve only found a few longevity studies on Everolimus. One showed an increased lifespan of 85% (1). Everolimus works so VERY similarly mechanistically to rapamycin, and according to Dr B, would deliver “equal lifespan enhancements” to Rapamycin, potency equivalent. More clinical trials seem to be using Everolimus and Tacromilus recently over rapamycin…better side effect profile as a chemo/immuno adjuvant. And in reality, rapamcyin has a poor record in existing cancer trials in terms of cancer mitigation or transplant rejection.
The article also says that c/w rapamycin, everolimus stimulates mitochondrial oxidation. What am I missing here? Do they mean increased mitochondrial stress from reactive oxygen species?
The increase in propensity for TOR 2 inhibition is also concerning.
I’ve seen quotes for Everolimus from $60 for 10 x 10mg tablets ($0.60/1mg), to $107 for 10 X 10mg ($1.07/mg). As noted, dosing mg/day needs to be increased by 50% to 100% over rapamycin doses for similar efficacy (see this information from Lloyd Klickstein interview)
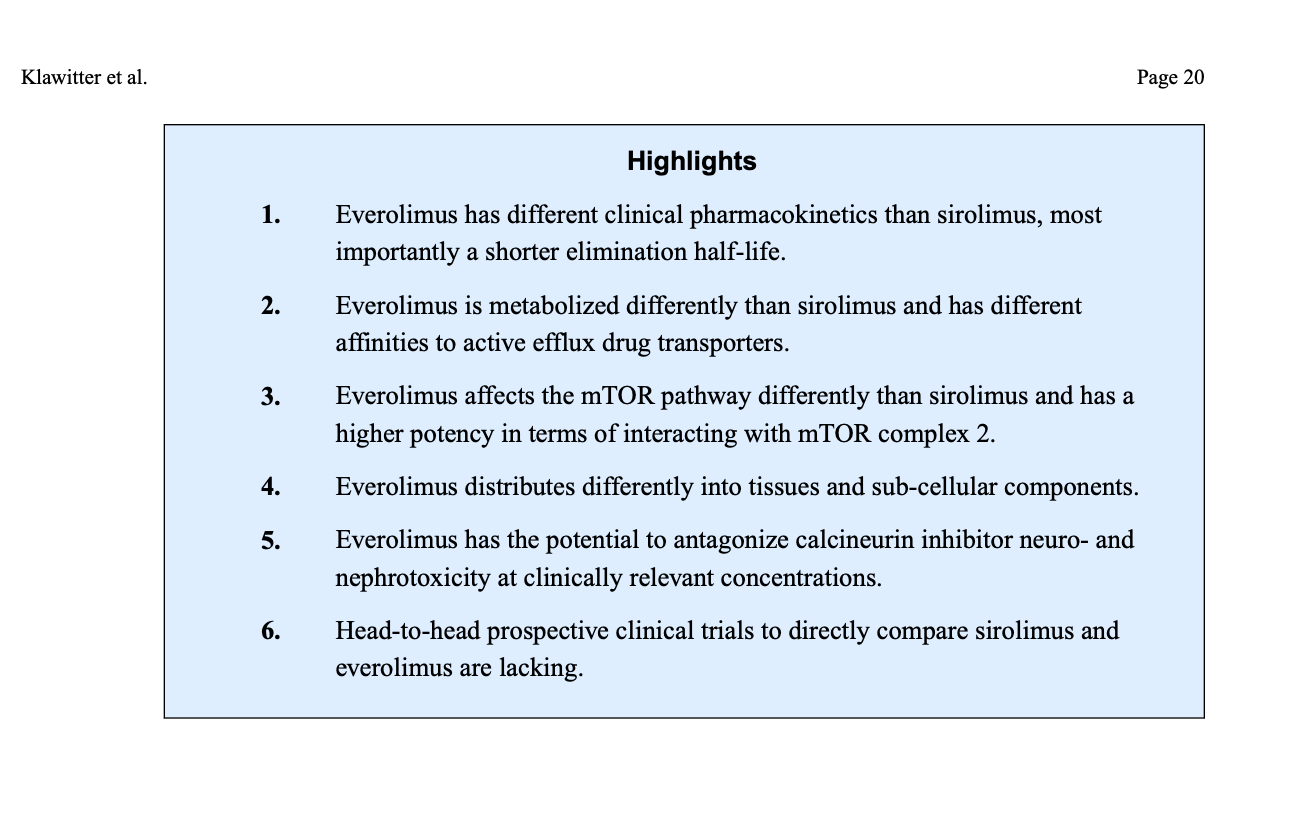
Find the note the above post by @MAC regarding the “Highlights” interesting, where 4. Everolimus distriubutes differently into tissues and sub-cellular components.
I think an argument can be made for alternating everolimus and rapamycin to get maximum tissue coverage (in terms of mTOR inhibition).
I’d never given the above review paper a good read. There are some very interesting findings/comments. If you go through it carefully, the author gives Everolimus the edge, especially clinical trials. It has superior efficacy in various important pathways, and fewer side ADE (Adverse Events) (eg. rejection, lipids).
Although there may not be many everolimus/mouse models and longevity, there are tons of clinical trials in humans (thousands++ patients), just like rapamycin. You’d think we’d know if any negative signalling by now?
Everolimus and Sirolimus in Transplantation-Related but Different
A couple of interesting findings:
The concept of needing twice the dose of Everolimus vs Sirolimus, where did this originate?
“Taking these findings into consideration, cyclosporine has a more profound effect on everolimus than sirolimus pharmacokinetics and our patients may need a considerably larger dosage of everolimus due to the lack of pharmacokinetic interaction with tacrolimus.”
So this is in the context of COMBINED Cyclosporine/Rapalog, NOT rapalog only. There is HUGE drug-drug interaction at play. What about head to head, no other immunosuppressants??
In this study:
Everolimus Inhibits Anti-HLA I Antibody-Mediated Endothelial Cell Signaling, Migration and Proliferation More Potently than Sirolimus
“Notably, the recommended levels of everolimus are lower than for sirolimus, consistent with our findings that everolimus more potently inhibits mTOR and related signaling”
So it seems lower trough levels for Everolimus than Rapamycin, which may or may not require a different dosing for same trough. But not a clinical translation impediment in any way.
This finding I found most intriguing, from the review paper:
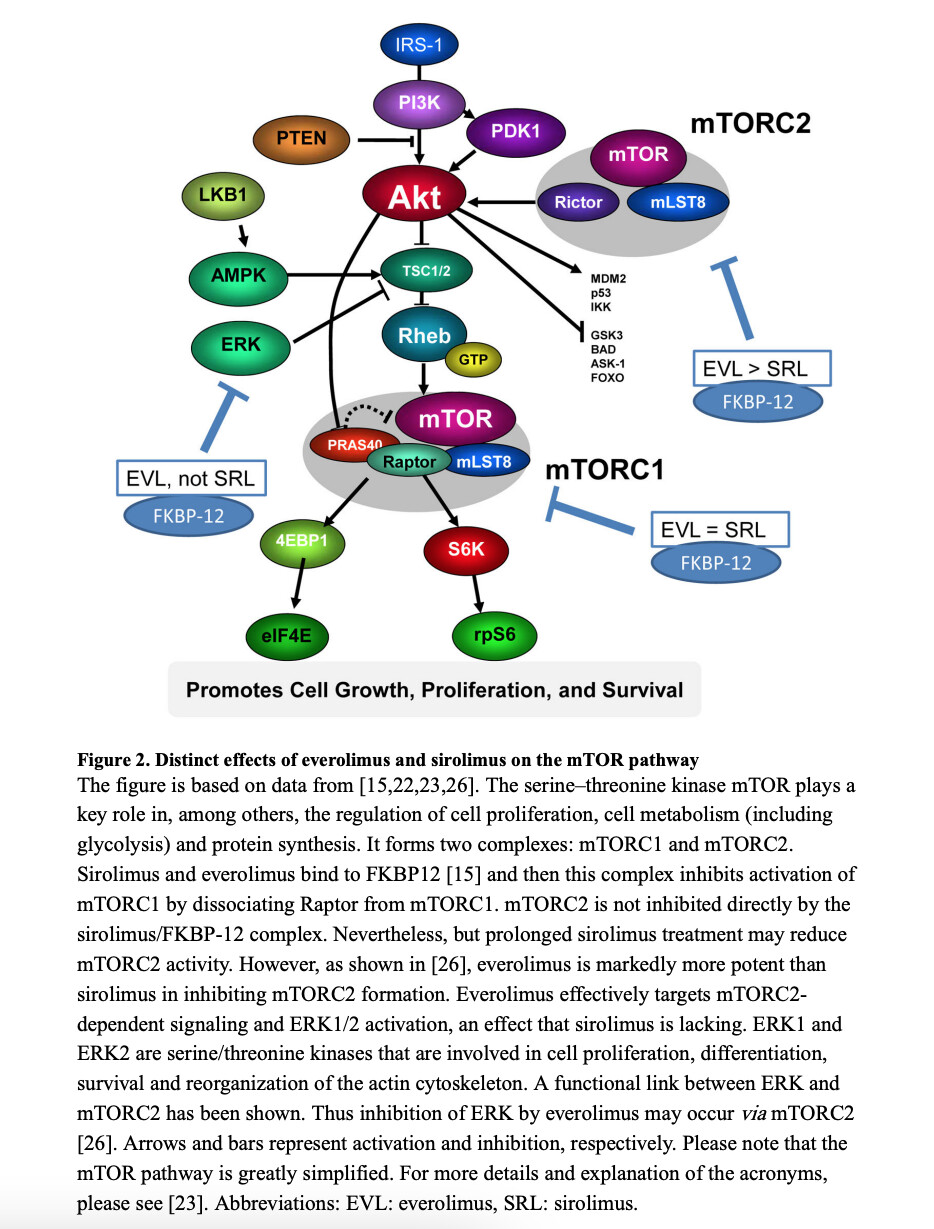
“Nevertheless, at the clinically relevant concentrations tested, everolimus was much more effective in inhibiting class-I-stimulated mTORC2 activation by dissociating Rictor and Sin1 from mTOR. This included more effective inhibition of class-I-stimulated AKT phosphorylation and inhibition of ERK phosphorylation, an ability that, remarkably, sirolimus lacked”
Animation above shows Everolimus more effectively blocking mTOR2, and ONLY Everolimus blocks AKT/ERK?!
But what is AKT/ERK?
"The AKT and ERK signaling are both aberrantly activated in a wide range of human cancers and have long been targeted for cancer therapy. During the process of tumorigenesis, a cell escapes from normal control of growth and acquires capability of invasion. Aberrant activation of the PI3K/AKT and/or MAPK/ERK pathways promotes cell survival and unlimited growth and proliferation, driving carcinogenesis. Only two PI3K inhibitors (idelalisib and copanlisib) and two mTOR inhibitors (temsirolimus and everolimus) have been approved by FDA for clinical treatment of cancers "
So is this unique interaction of Everolimus vs Sirolimus clinically relevant for longevity via cancer suppression??
mTORC1 and mTORC2 in cancer and the tumor microenvironment
“Although mTORC1 signaling has been extensively studied in cancer, recent discoveries indicate a subset of human cancers harboring amplifications in mTORC2-specific genes as the only actionable genomic alterations, suggesting a distinct role for mTORC2 in cancer as well. While mTORC1 is extensively studied in cancer, recent reports also demonstrate a distinct role for mTORC2 in prostate, breast, and lung cancer, glioblastoma, and T-cell acute lymphoblastic leukemia…reinforcing the importance of mTORC2 signaling in cancer and as a potential target for inhibition”
This sounds like a meaningful signal to inhibit at some level…mice only die of cancer, so isn’t that the implicit translation to humans we are all hoping for??
Is it possible, that the long lived mice on rapamycin are really achieving this lifespan attainment by additional to TOR1…inhibition of mTOR2? Consider they are on chronic administration, so certainly plausible? And it’s only because researchers DO NOT UNDERSTAND what TOR2 really does or READILY MEASURE, that this pathway is really underpinning some of the lifespan extension? It has been theorized by many of the leading researchers (MK/LAMMING), but dismissed as taboo due to enhanced side effects associated with interaction with TOR2. But what about harnessing some of this for human translation?
Here is a dose escalation study of Everolimus (still want to compare to a similar head to head Sirolumus)
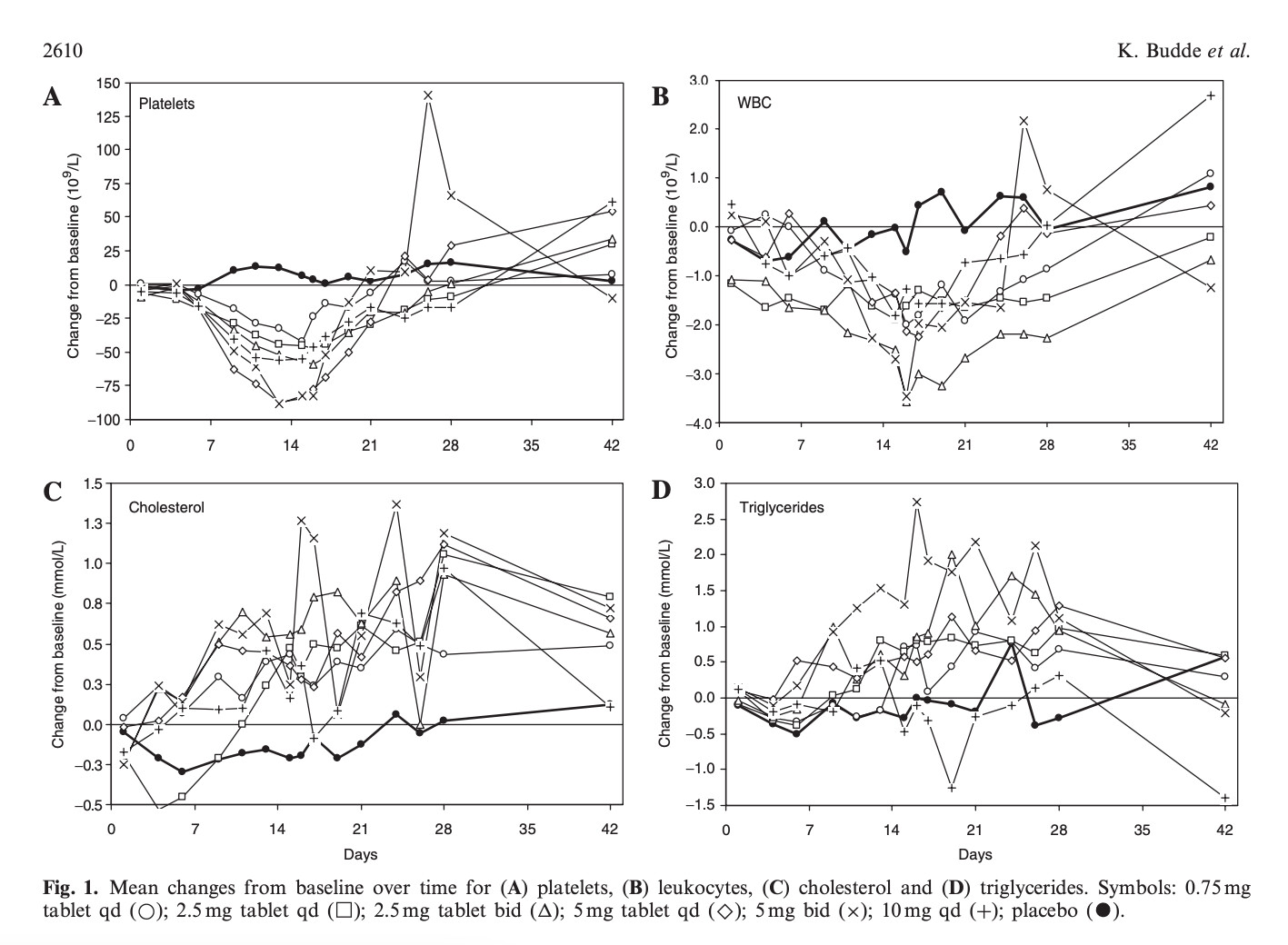
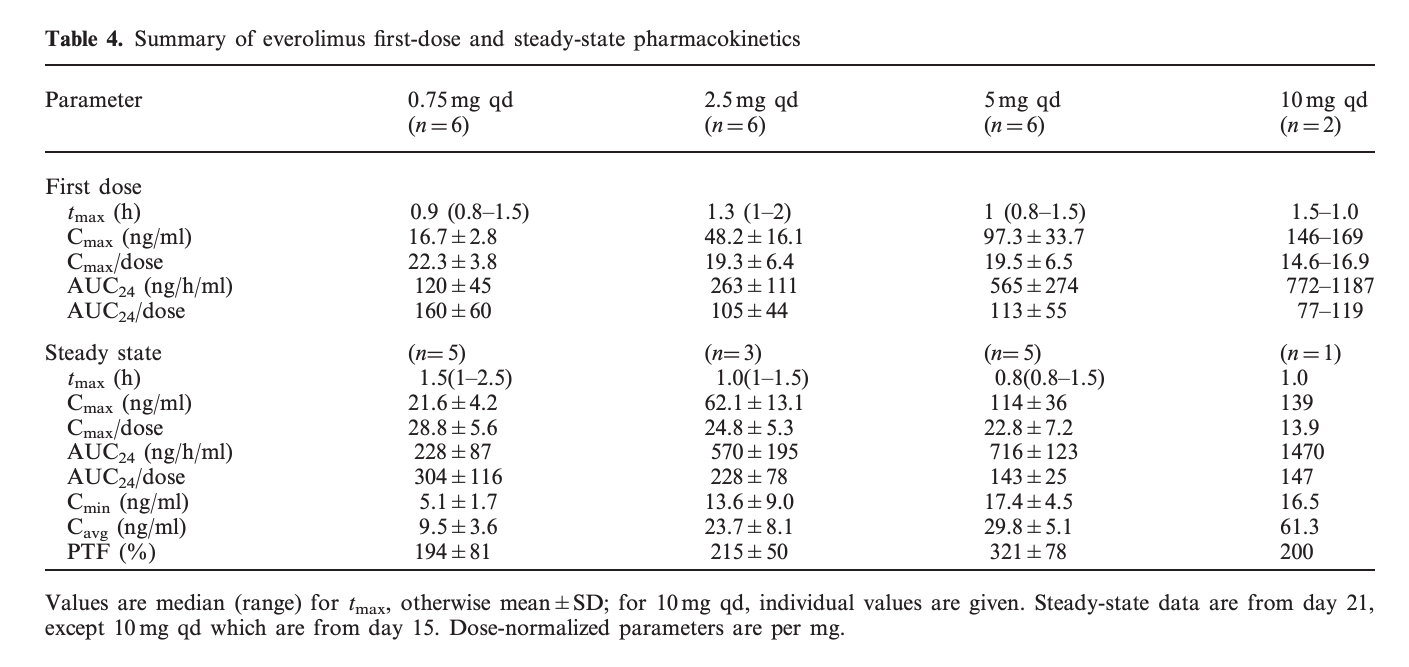
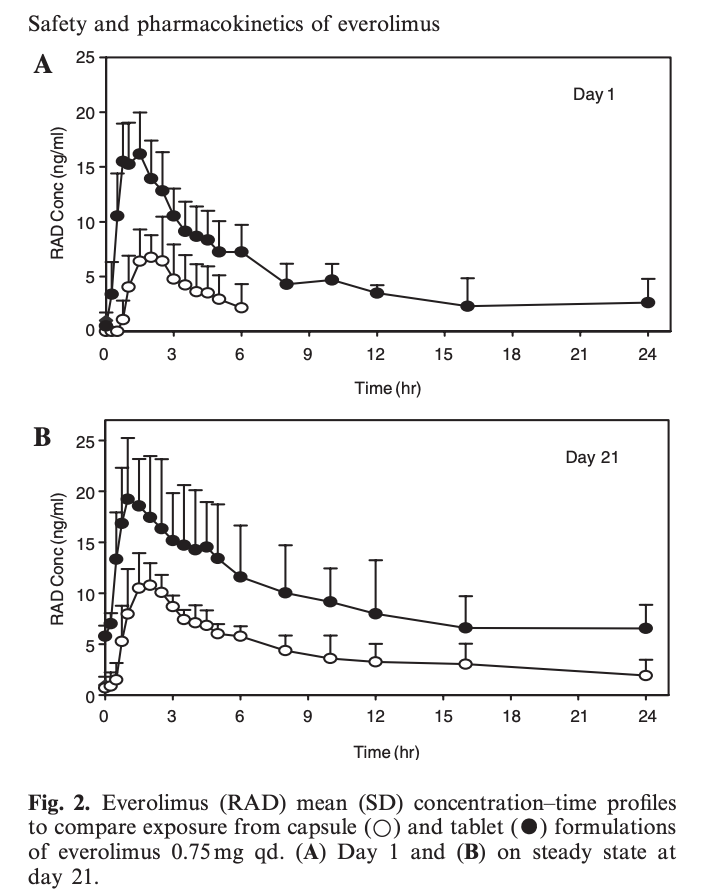
" The primary objective of this multicentre, randomized, double-blind, placebo-controlled, dose escalating phase 1 study was to evaluate the safety and tolerability of everolimus at four dose levels (0.75, 2.5, 5 and 10 mg/day) in maintenance renal transplant patients receiving cyclosporin and steroids. The secondary objective was to assess the pharmacokinetic profile of two different formulations (capsule and tablet) of everolimus."
As you can see, after an initial drop in platelets and WBC, at 42 days out, 0.75mg/day or 2.5 mg/day do NOT result in significant changes (modest?) in these parameters, as well as cholesterol and TG.
A 0.5 mmol/L rise in cholesterol is about 20 mg/dL. A 0.5 mmol/L rise in TG is approx 45 mg/dL.
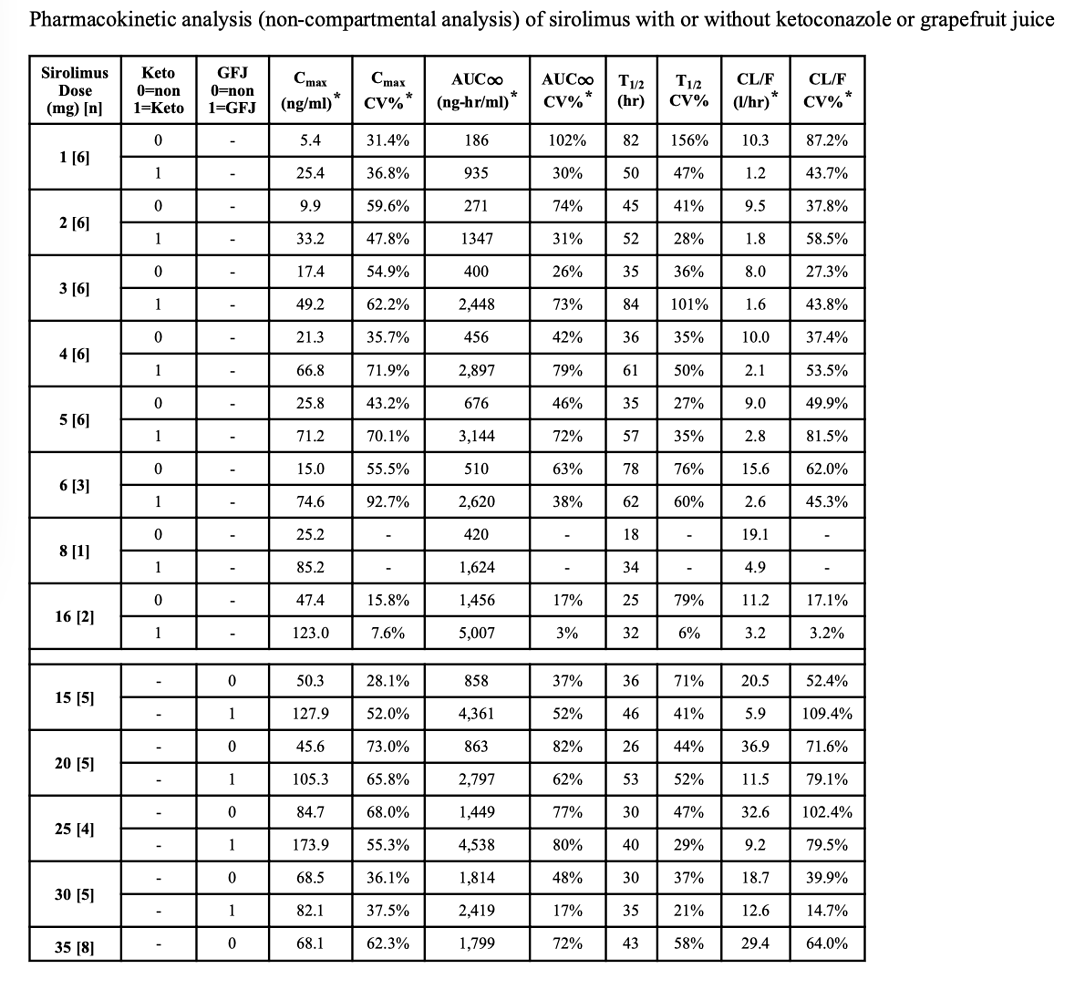
What about AUC, and comparisons to Sirolimus?
At 0.75mg/day Everolimus (5.25mg/week), this is dose equivalent to about 5mg/WEEK of Sirolimus. 5mg/week of Sirolimus (no GFJ) has an AUC-infinity of about 676 ng-hr/mL. There is not AUCinfinity reported to Everolimus at 0.75mg/day, only AUC24 of 228. Extrapolating to infinity, it would be higher. Certainly at 2.5 mg/day, AUC24 of Everolimus is already at 570 ng-hr/mL.
From what I know so far, I would have no qualms switching from Rapamycin to Everolimus. Potentially offers a better cancer suppression efficacy? Possibly lower dose/side effects? The clinical trials give it an edge over Sirolimus. Possibly higher LONGEVITY?!
Part of my rationale is a long term view…if I’m going to take this drug for potentially decades, side effects is a very big deal in terms or risking some other deleterious pathway. But I want my cake and eat it too…maximal impact on growth/cancer suppression, yet few side effects. CVD, immuno, infections, which plague high dose rapamycin, and potentially critically limit maximal human longevity translation?!
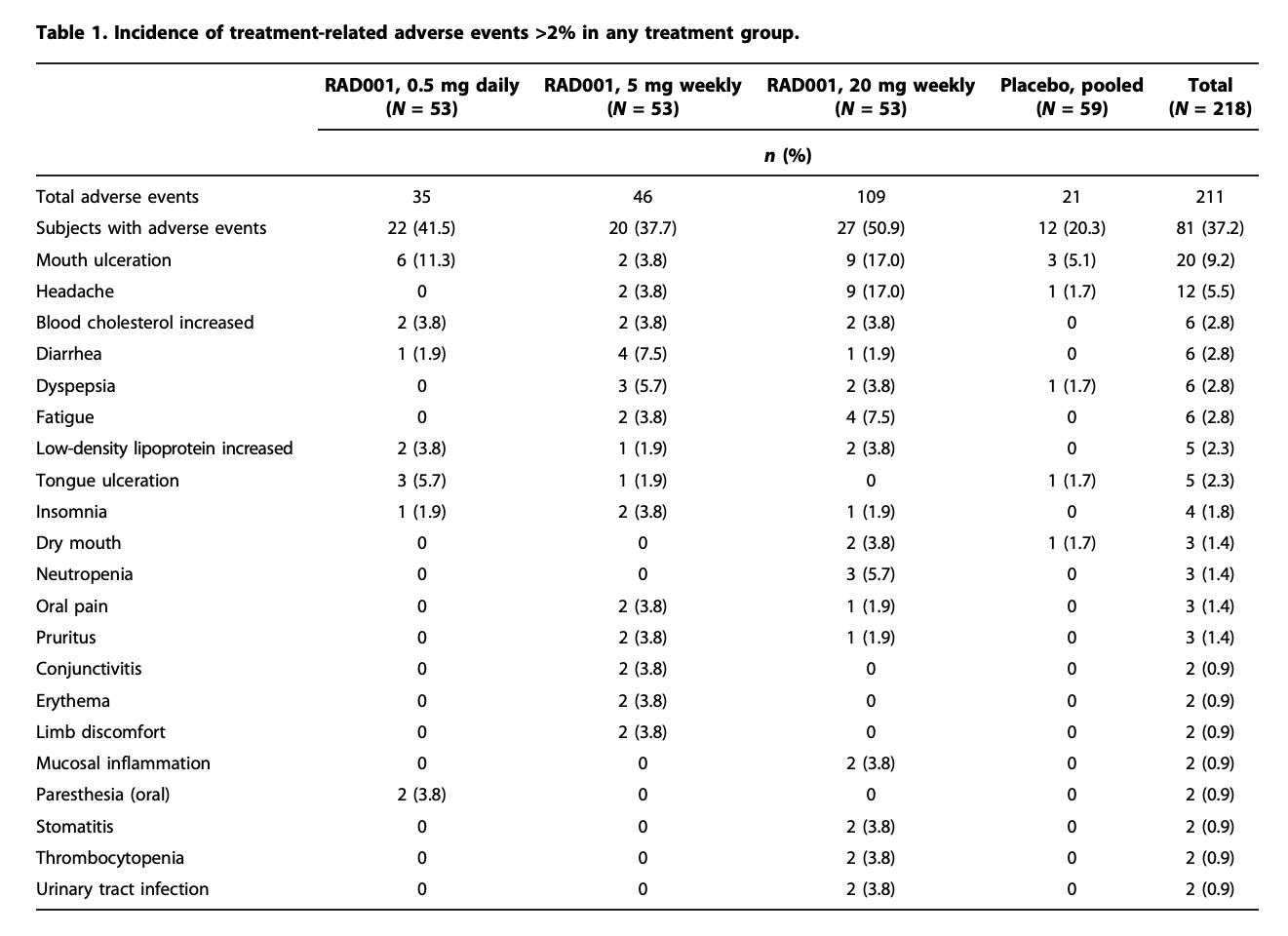
The Mannick 2014 study using Everolimus at 0.5mg/day or 5mg/week was well tolerated. You’d think if the researchers had ANY concerns about Everolimus safety, they certainly wouldn’t have chosen it for an eldery (n=1218, > 65 yo) population!
At time of writing, I am still working through my exploration with Rapamycin, but always on the hunt for something better. Everolimus might be a better train to hop on.
Everolimus is better than rapamycin in attenuating neuroinflammation in kainic acid-induced seizures
Conclusions
“Rapamycin and everolimus can block the activation of inflammation-related molecules and attenuated the microglial activation. Everolimus had better efficacy than rapamycin, possibly mediated by the inhibition of ERK phosphorylation. Taken together, mTOR inhibitor can be a potential pharmacological target of anti-inflammation and seizure treatment.”
Very comprehensive. The graphs are very noisy but I think I get the message.
In the Mannick study, I believe that the 5 mg per week was as effective as the 20 mg. Since one reason to switch to everolimus would be to up the dose, I’m not sure that it’s necessary, at least as far as immune response is concerned.
At 5 mg only about 4% incidence of increased cholesterol. Maybe same for triglycerides? What about glucose?
With a half life close to 24 hrs, you could hit it again at 4 days I guess.
I really like zero neutropenia or thrombocytopenia with the 5 mg weekly dose, the other side effects are no big deal.
I like the cancer inhibition for prostate, lung, brain and ALL. Of course, if you eliminate All cancers it only translates to an extra 3 years longevity, but still.
Are we now thinking that we actually want some TOR 2 inhibition?
Why hasn’t Blagosklonny or Matt switched over?
It’s getting tempting. So a real life example:
Day one 5 mg everolimus. It’s practically gone by day 3-4. So do we dose it again?
Day 7 rapamycin
Day 14 everolimus again
What, all this work for 3 years…you referencing all cause mortality stats? You dismiss some of these pathways and mTOR inhibition dosen’t impact CVD or neurodegeneration?
Yes, shake things up!
What do they know…they’re in the same dart club as us. Dr B is captain mTOR, don’t think he’s got Everolimus qualms. Might just be access/cost?
We have no data here…speculation on pharmacological/kinetic differences.
Everolimus is plenty efficacious, I don’t see why you’d need to complicate with both. Everolimus has better BBB penetration supposedly. You can simply up frequency of dosing with Everolimus and achieve targets.
If you look at All age related diseases the longevity impact is very significant, but if you isolate just one of them, not so much.
Yeah, I’d still like to get one of them to offer an opinion. Seems to me that Matt once said that he’s hesitant because all of the longevity work has been done on rapamycin. Might be wrong about that but that’s what I think he said.
But aren’t we hopeful we are hitting all aging and mortality pathways with mTOR? There are a zillion studies of mTOR inhibition and all manner of aging pathways…pretty much all beneficial.