To Desertshores’s point, and against those that argue from the lower number of longevity-relevant studies in Everolimus: AFAIK, the only animal study showing preserved muscle in aging rodents from a rapalog used Everolimus, not rapa.
No, but it’s been done by weight in other longevity studies (though I doubt individualized to the specific mouse); also, in ITP they dosed in in ppm of food, so the larger a mouse was (and thus the more it ate) the higher its rapa dose would be.
Side note: Empagliflozin extends lifespan in rodents (based on one paper). And we know one mechanism as Mendelian randomization shows that SGLT2 inhibition extends male lifespan.
In the in vitro tests as I remember it they used 1 nano Molar both E and R/S. Normally people use a higher Rapamycin dose. Hence to do the comparison properly would require a higher dose. E actually has a higher molecular mass.
Sorry for not getting back, my practice has become busy.
So my thoughts would be still intermittent with this, 30 hr T1/2, but that is with daily dosing, I suspect it’ll be shorter, like rapamycin with a single big dose cyclically.
Levels are harder to get and cost more than sirolimus.
Cost of the meds, at CVS 60 x 0.75 mg are $172. It looks like equivalent potency is 0.75 mg everolimus = 1 mg of sirolimus.
My tendency would be to do a mg for mg or higher substitution with everolimus, maybe even 1.25 mg of everolimus to one’s prior 1 mg of rapamycin. E.g. if taking 8 mg of Rapamycin q7 days, I’d look at 10 mg of everolimus q7 days to account for #1 higher potency or everolimus, but then shorter half life so the time in a therapeutic level will be similar, but your peak with the everolimus would be higher by quite a bit.
These are just my thoughts on it - anyone acting on anything should consult their doctor.
I had not heard that Empagliflozin had been tested for longevity in mice. That’s good news if it also showed increase in health/life span. I’d also not seen the Mendelian randomization. I wouldn’t have thought SGLT2’s had been around long enough to power a MR study… Can you link both of these? I usually follow the mega thread on SGLT2’s pretty closely but I must have missed this interesting bit.
re rapa vs Everolim paper in kainic acid seizures
Perhaps we are having this discussion prematurely? I mean it’s one paper from a Chinese group, experiments performed in vitro and in mice, and its an induced seizure with questionable human clinical relevance. I’m just not sure it’s worth our time yet.
Answer from Jose-Alberto Palma MD PhD FAAN who led the failed trial of sirolimus in MSA:
Everolimus might work provided that it crosses the BBB in sufficient amount as to inhibit the mTOR pathways in neurons (and possibly also glia) in key brain areas involved in MSA/PD (e.g., basal ganglia).
Mouse studies and RWE studies are interesting to unveil hypotheses that should be confirmed in placebo-controlled human trials.
So… no one knows whether everolimus is better than rapa or not at crossing the BBB and being neuroprotective…
Mitochondria only spread cell-to-cell to adjacent cells via tunneling nanotubes, etc. Mitochondriopathies, Parkinson’s, aging muscle, and other diseases involving mitochondrial mutations show focal areas of high mutation burden in afflicted tissues, with other cells and tissues having low mutation burden and unaffected.
Spindler ran a huge ITP-on-steroids operation in the last few years of his research career and a lot of it wound up unpublished when he retired. He was one of the top 5 most competent lifespan study scientists and his methods and powering were robust: if he reported it in any context, it’s credible.
All but one of your studies here involve an acute inflammatory insult such as LPS, which tends to cause BBB leakiness, which might explain why rapa gets in under these circumstances and not under physiological conditions. Also, most involve repair of the brain vasculature itself, which does not require BBB transit.
Oh yeah, Spindler is a legendary name in CR and generally longevity field, I’ve been following him for decades. Extremely competent and very credible. His word counts for a lot with me, which is saying something, as I tend to be very resistant to personality driven authority. Spindler studies were always of the highest standards.
Are you referencing this paper, or is there another? In addition to being a Chinese group, the control animals were miserably short-lived (median survival 690 days) and survival was only improved 5.9% (to a still-abominable 730.8 days in Empa) in the male mice; that’s pretty much meaningless.
Looks like a really high dose if that is per mouse rather than per kilogram of mouse.
I don’t think you can read much into this.
I would assume that beyond the issue of short life and dosing the effect of inhibiting mTOR is much the same.
I am personally sticking with Rapamycin because it does what I want it to do, but at the moment I don’t want to take it until I have resolved the issue with my low WBC. I think I have resolved the issue, but I don’t have test results to prove this.
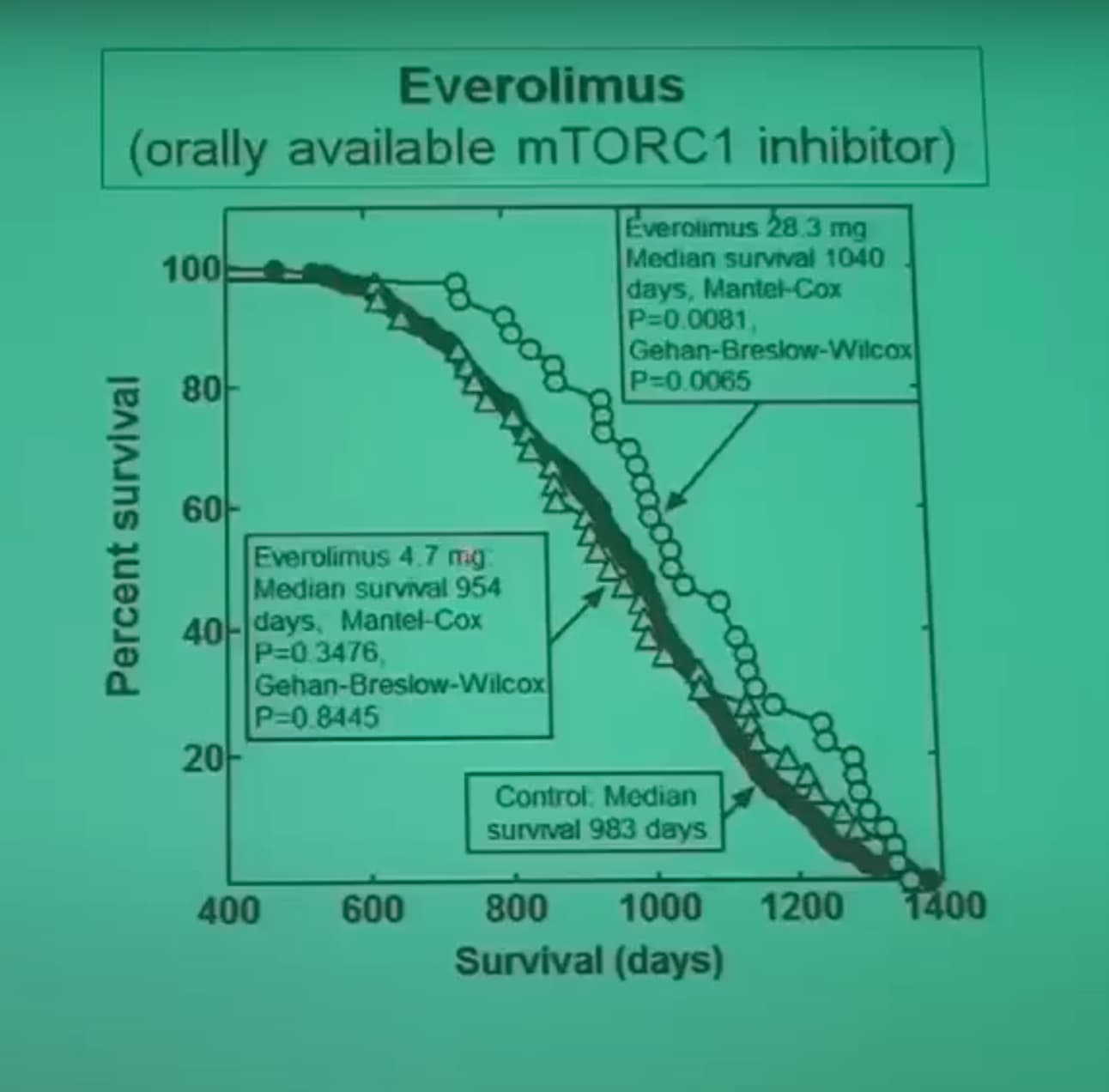
Wow! That’s a pathetically small effect! I had never gotten a clear shot of the numbers. I had assumed that the effects of rapa and everolimus would be quite similar; this is effectively a null result .
Good question. It seems unlikely it means mg/kg mouse (why would they start with double the rapa dose and then go to 10x of it?), but the other alternatives also seem unlikely (28.3 mg per mouse (definitely not), or 28.3 mg/kg food).