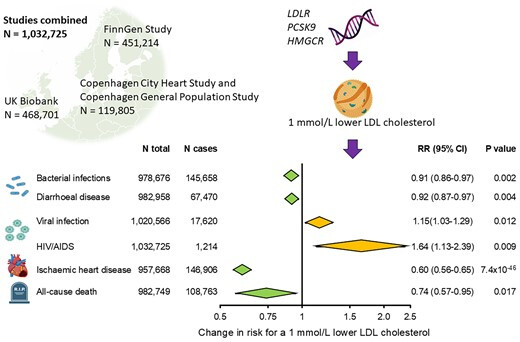
“* If you have high Lp(a): slash apoB, the lower the better, and get vaccinated”
Since Lp(a) is such a negative, perhaps it might make a difference in how you slash ApoB. It is known that PCSK9i slashes ApoB without raising Lp(a), and possibly even slashing Lp(a) levels by as much as 20% (which to be clear may not be anywhere near sufficient for those with high/very high Lp(a) levels).
However, for those at high risk of CVD who need the biggest slashing of ApoB, use of PCSK9i by itself is not enough and combination therapy is used with the addition of statin, ezetemibe (and even bempedoic acid).
Unfortunately, when recommending the most serious slashing of ApoB because of high levels of Lp(a), you may need to resort to this multiagent therapy to achieve those low ApoB numbers. And that multiagent therapy includes a statin, and statins tend to raise Lp(a) levels (modestly around 10% or so, but possibly up to 20%).
So how to avoid this paradox? Well, here again the choice of which statin becomes crucial. Pitavastatin somewhat uniquely among statins does not raise Lp(a) levels at all, and may even possibly slightly lower those levels. From the study I posted:
“Pitavastatin – effect on Lp(a)
Elevated serum Lp(a) concentration is an ASCVD risk factor independent of serum LDL-C concentration [68]. The EAS consensus indicates that the cut-off value for serum Lp(a) concentration should be 50 mg/dl (−125 nmol/l) [46]. However, there are data indicating that already at serum Lp(a) concentrations above 30 mg/dl (−75 nmol/l), CV risk increases [1, 68]. There are also indications of a preference for tests that determine the number of Lp(a) molecules in nmol/l rather than the mass in mg/dl [1].
The use of statins is associated with an increase in serum Lp(a) concentrations, although this is not clinically relevant [69, 70]. On average, the increase in serum Lp(a) concentration is 6–10% [1]. The increase in serum Lp(a) levels in patients treated with statins is part of the residual CV risk that remains, despite good control of serum LDL-C levels [69, 71].
In the context of its effect on Lp(a) concentration, pitavastatin also appears to be different from other statins (no class effect), as it does not affect, or may even slightly reduce its serum concentration. The VISION randomised clinical trial evaluated the effect of pitavastatin 2 mg/day vs. atorvastatin 10 mg/day for 12 weeks on serum Lp(a) concentrations in 42 patients with hypercholesterolaemia. It was concluded that pitavastatin showed a tendency to slightly reduce serum Lp(a) concentrations, although this effect did not reach statistical significance. No such effect was shown for atorvastatin [72]. These findings were confirmed in a meta-analysis of 20 RCTs conducted by Wang et al. involving 23,605 participants. In this meta-analysis, it was found that, of all statins, pitavastatin had the most beneficial effect on serum Lp(a) concentrations, which was manifested by a tendency to reduce these concentrations [73].
Expert recommendation
Pitavastatin, unlike other statins, appears to have a neutral effect on serum Lp(a) concentrations, and may even reduce these concentrations to a small extent. Pitavastatin may be considered for use in patients with elevated Lp(a) concentrations (IIb). Further studies are needed to confirm this relationship, as well as to assess the effect of pitavastatin on the size of apolipoprotein(a) isoforms.”