What are people’s thoughts on this?
Source: x.com
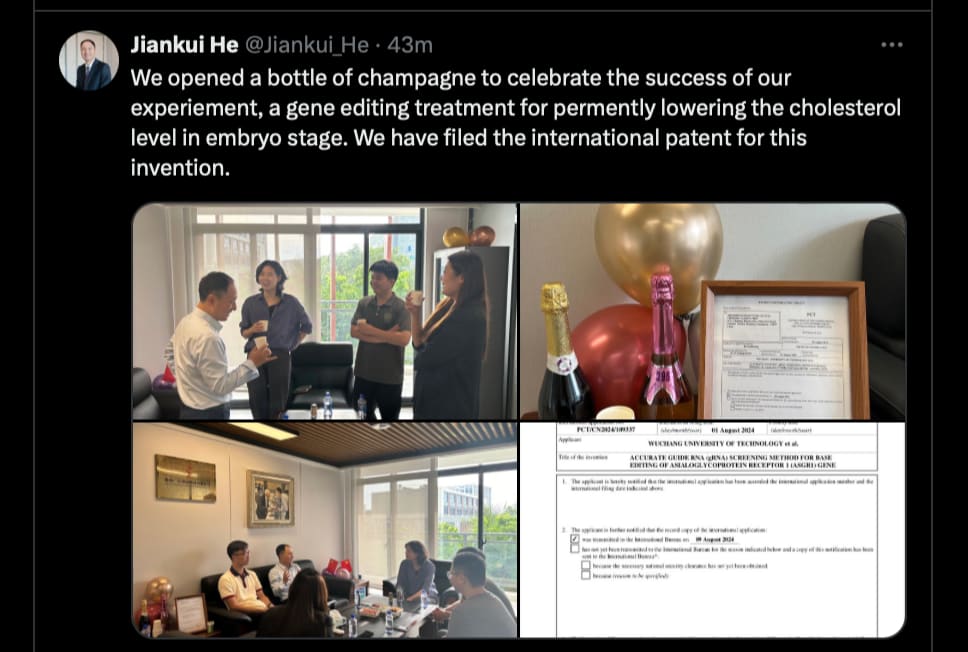
I would wait and see how the first generation turned out. ![]()
Maybe try it on marmosets first. If they all look ‘special’, then rethink it.
Chinese gene editing patent, eh? OK. Let them open the champagne (hopefully not counterfeit), but I personally will stay with my usual coffee. Wait and see, no hurry - toddlers and small kids have very low cholesterol naturally, so it won’t be apparent whether this works until much later. Furthermore, we’ll have to see whether the effect persists long term, and finally is it safe and are there any unexpected side effects of this editing - this could be a lifetime experiment… we’ll all be long dead before all that checks out. In other words I see no reason to urgently rush out to buy cases of celebratory bubbly.
That said, there’s one thing I must give the Chinese approach to science a lot of credit vs the Western approach. They have no qualms about forging ahead without being held back by non-scientific specific culturally dependent superstitions as happens far too frequently in the West (“against nature”; “against God’s plan”; “unnatural and eugenic”)… all that does is hold humanity back for moronic reasons. There’s a fine balance between legitimate safety concerns (often sadly lacking in Chinese experiments), and illegitimate obstructionism and prejudice, as happens in the West (EU bureacrats idiocy knows no bounds). YMMV.
I’m in favor of other people trying it, yes. I doubt very much whether there will be a difference that can be measured, and that’s if all it does is reduce cholesterol.
I think cyclarity has an approach that can fix the problem with a lot less chance of disaster. Did they aim for a different target to keep people from going deaf? I didn’t completely understand the last video I posted. It’s the one about clearing 7 ketocholesterol.
Physionic on the #1 cause of arteriosclerosis.
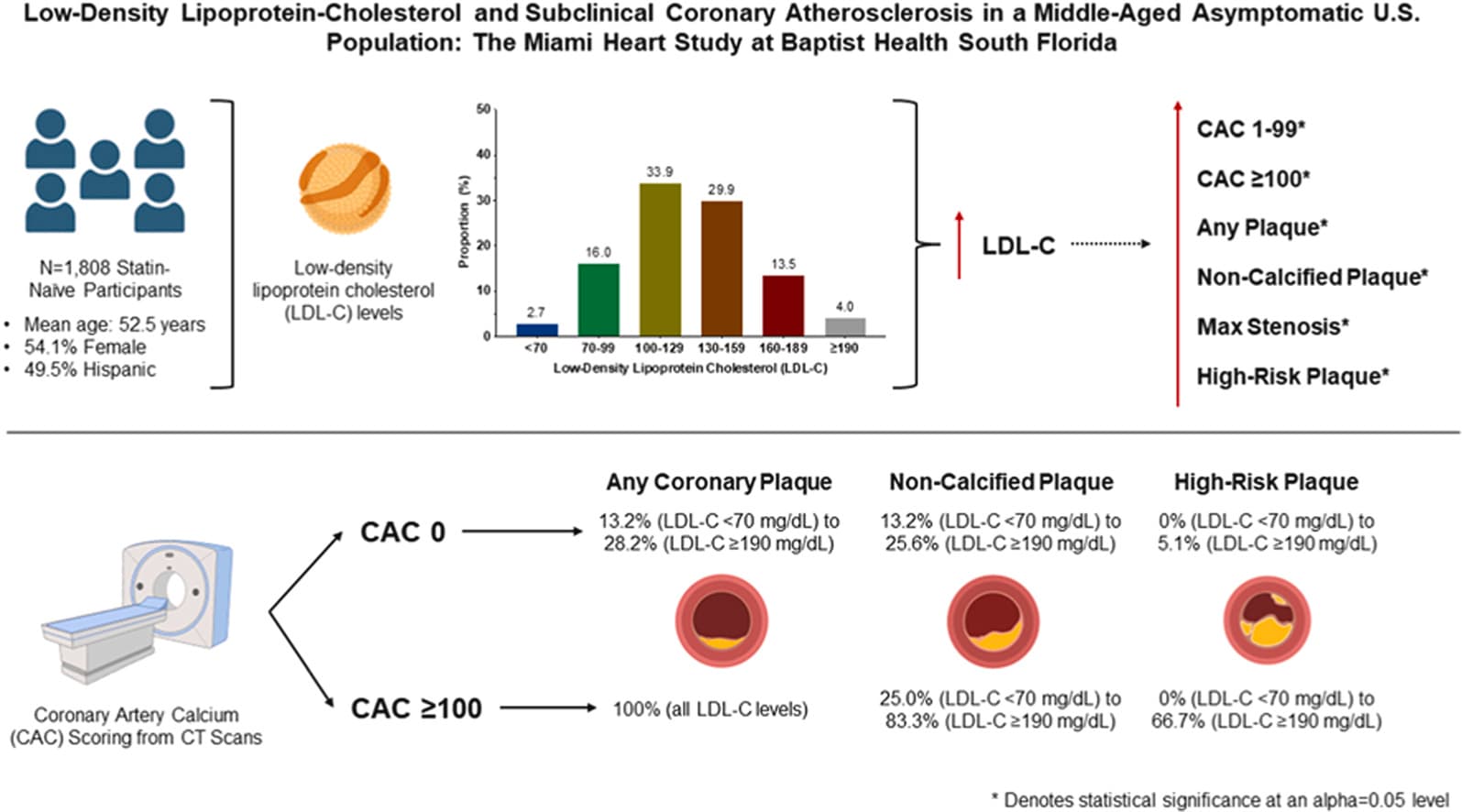
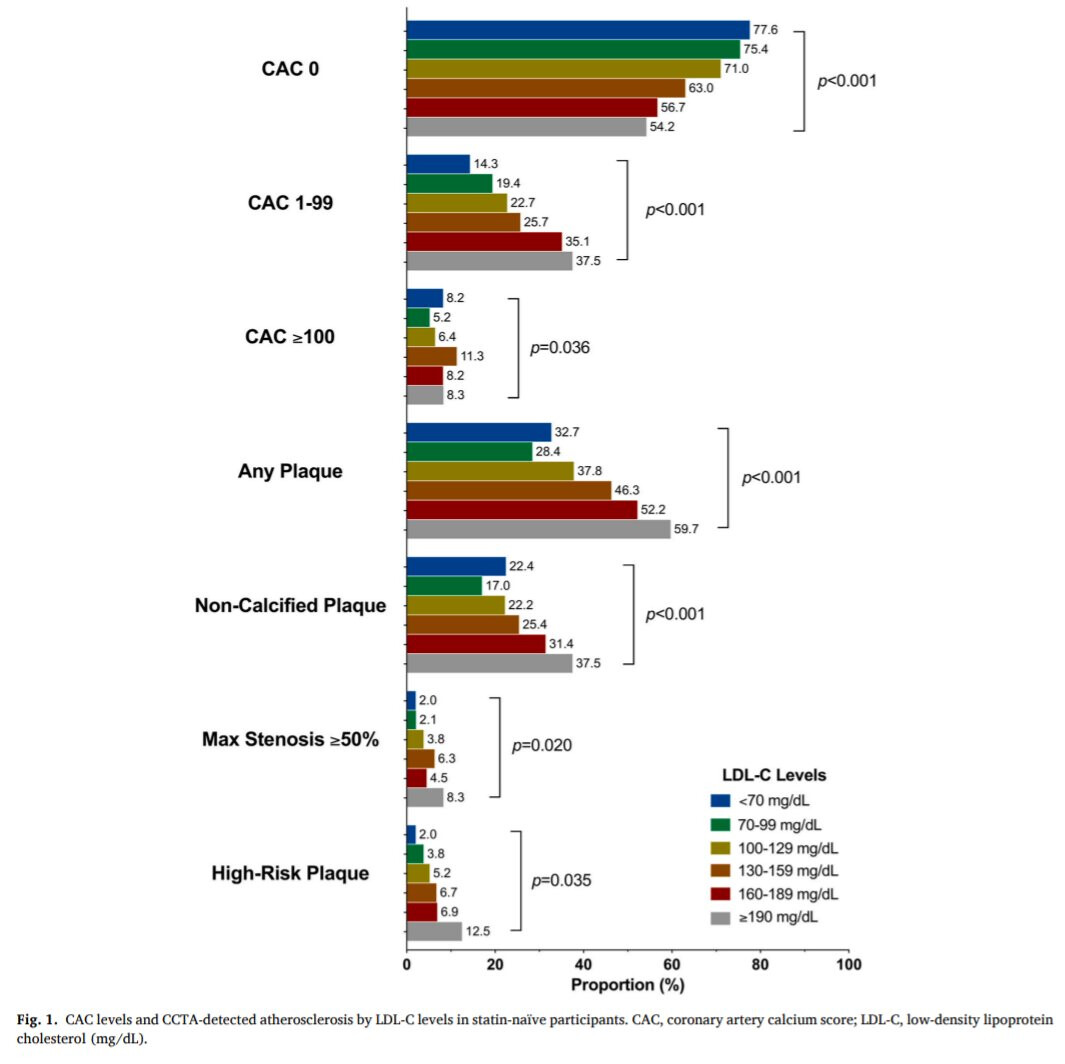
More on the Miami Heart Study: Low-density lipoprotein-cholesterol and subclinical coronary atherosclerosis in a middle-aged asymptomatic U.S. population: The Miami Heart Study at Baptist Health South Florida
Highlights:
- Coronary plaque presence increased with LDL-C and clinical risk, even in the absence of CAC.
- There is considerable atherosclerosis in statin-naïve participants with low LDL-C and clinical risk.
- About 2 in 5 statin-naïve participants with severe hypercholesterolemia did not have any plaque on CCTA imaging.
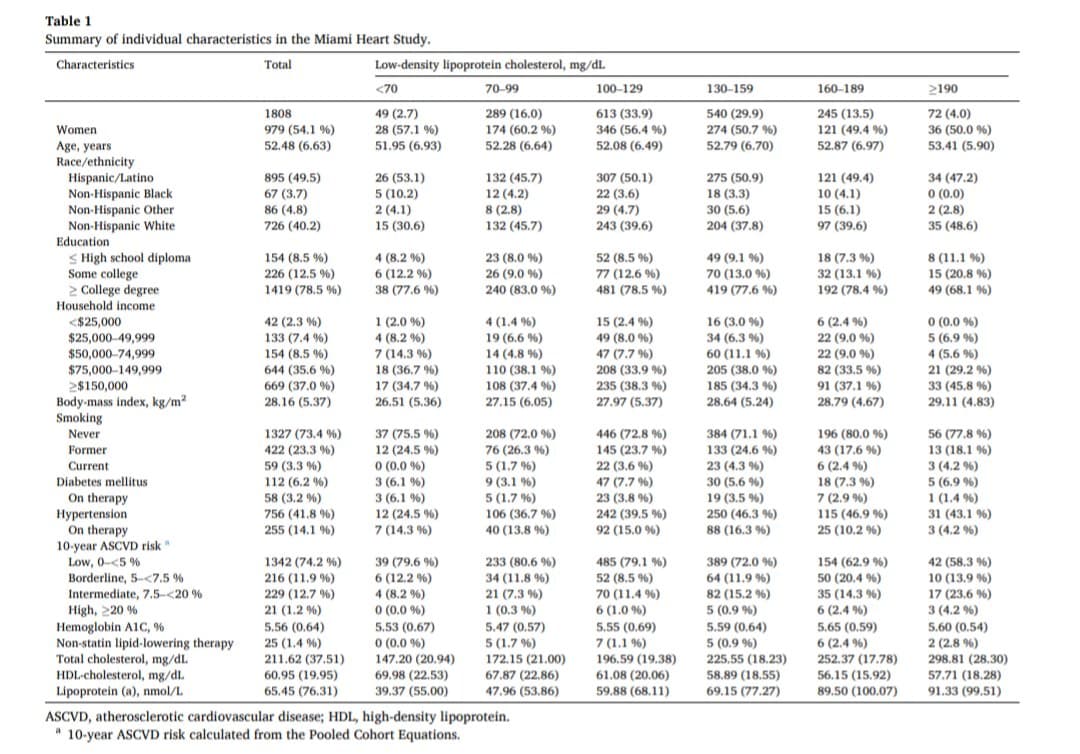
Weirdly btw, compared to people with low cholesterol (< 70 mg/dL), people with high cholesterol (> 190 mg/dL) are more likely to be wealthy (> $150k income): 46% vs 35%:
Weirdly btw, compared to people with low cholesterol (< 70 mg/dL), people with high cholesterol (> 190 mg/dL) are more likely to be wealthy (> $150k income):
Maybe related to dietary habits?
It might be non-significant. BMI increases linearly with LDL, but there’s a big jump from 190 mg/dL for income.
However, this paper says: Socioeconomic status and education level are associated with dyslipidemia in adults not taking lipid-lowering medication: a population-based study 2022:
“In men, the higher the socio-economic or educational stratum, the higher the total cholesterol, low-density lipoprotein cholesterol (LDL-c) and triglyceride (TG) levels and the lower the high-density lipoprotein cholesterol (HDL-c), after controlling for age, body mass index, hypertension, smoking habit and physical activity. In women, the higher socio-economic strata were associated with elevated total cholesterol and HDL-c, while lower total cholesterol, LDL-c and TG levels were found in those with higher education levels.”``
Did papers showing a U-curve for LDL and mortality adjust for income and education?
If I can just raise my LDL-C, maybe I could afford a new car and become a Lean Mass Hyper Provider.
Possibly because people who are wealthy can afford to eat whatever they want, whenever they want it. I was super lean when I was a broke grad student, then got chunky when I got a real job. Now super lean again, thanks to tirzepatide ![]()
The best foods available at the highest prices are not chosen for cholesterol level but for taste and opulence. Think of filet mignon, foie gras, caviar, etc… LDL lowering foods are usually not the ones rich people would like to eat. Think of leafy greens, oatmeal, etc…
Also, rich people think their money will save them because they have comprehensive health care. Why take statins? A triple bypass or something better (they are immortal after all) will be available when they need it.
“Compared to the systemic delivery of similar doses of simvastatin, the nanoparticles can deliver 1000 times more of the drug to the plaques, thereby enhancing the therapeutic efficacy while minimizing systemic side effects.”
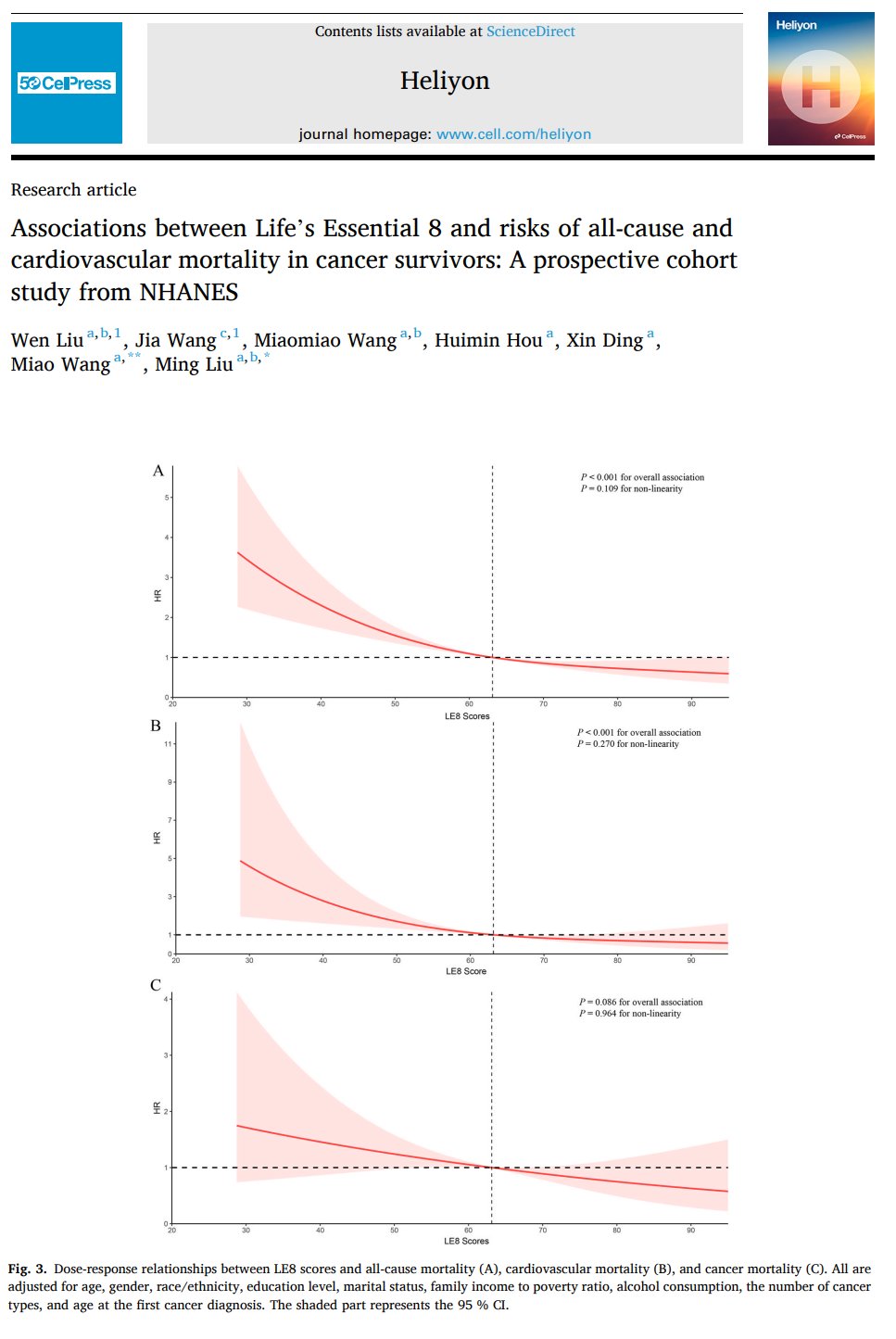
Here, a higher level of cardiovascular health, as evaluated using the American Heart Association’s Life’s Essential 8 cardiovascular health score, was associated with a lower risk of all-cause and cardiovascular disease mortality in cancer survivors living in the US.
The American Heart Association’s Life’s Essential 8 cardiovascular health score consists of 8 modifiable metrics: physical activity, diet, smoking status, BMI, systolic blood pressure, fasting plasma glucose, cholesterol, and sleep.
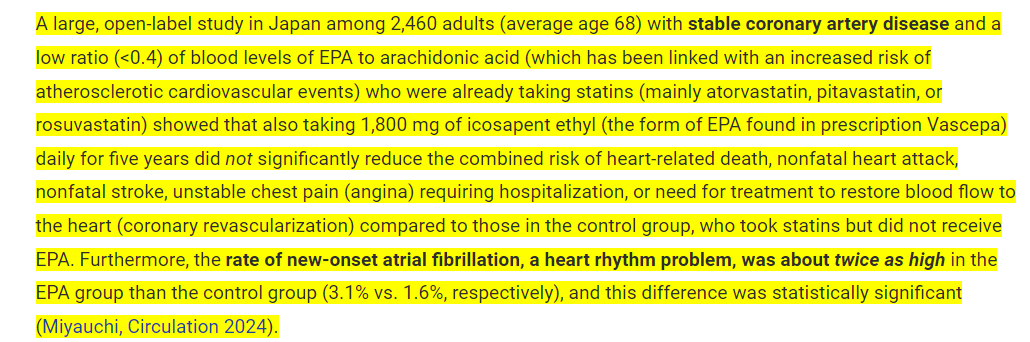
Here is one common combination that doesn’t work out. It’s better to NOT take these two together. I’ll be cutting my Omega-3 dose in half based on this to 1 g a day down from 2 g.
According to ConsumerLab, it appears that taking fish oil with a statin doesn’t convey any lower risk of CVD. In fact, it provides detriments in a doubling of the risk of Afib. So, you may want to cut back on that fish oil if you’re already taking statins. The 1,800 mg of EPA is equivalent to about 4 g of fish oil which has shown to be correlated to increased Afib in other studies. It seems that the statin provides the benefits and the Omega-3 can’t do anything else for CVD on top of the statin. A 1-2 g dose of Omega-3 daily should be fine though.
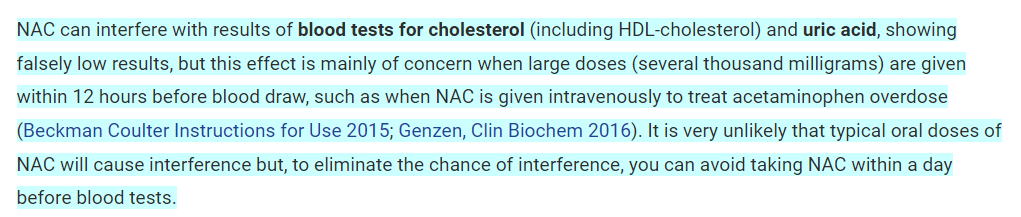
NAC can artificially lower LDL and HDL results in blood work according to ConsumerLab.
Those of you taking GLYNAC or high doses of NAC (like myself) probably have higher cholesterol than you think.
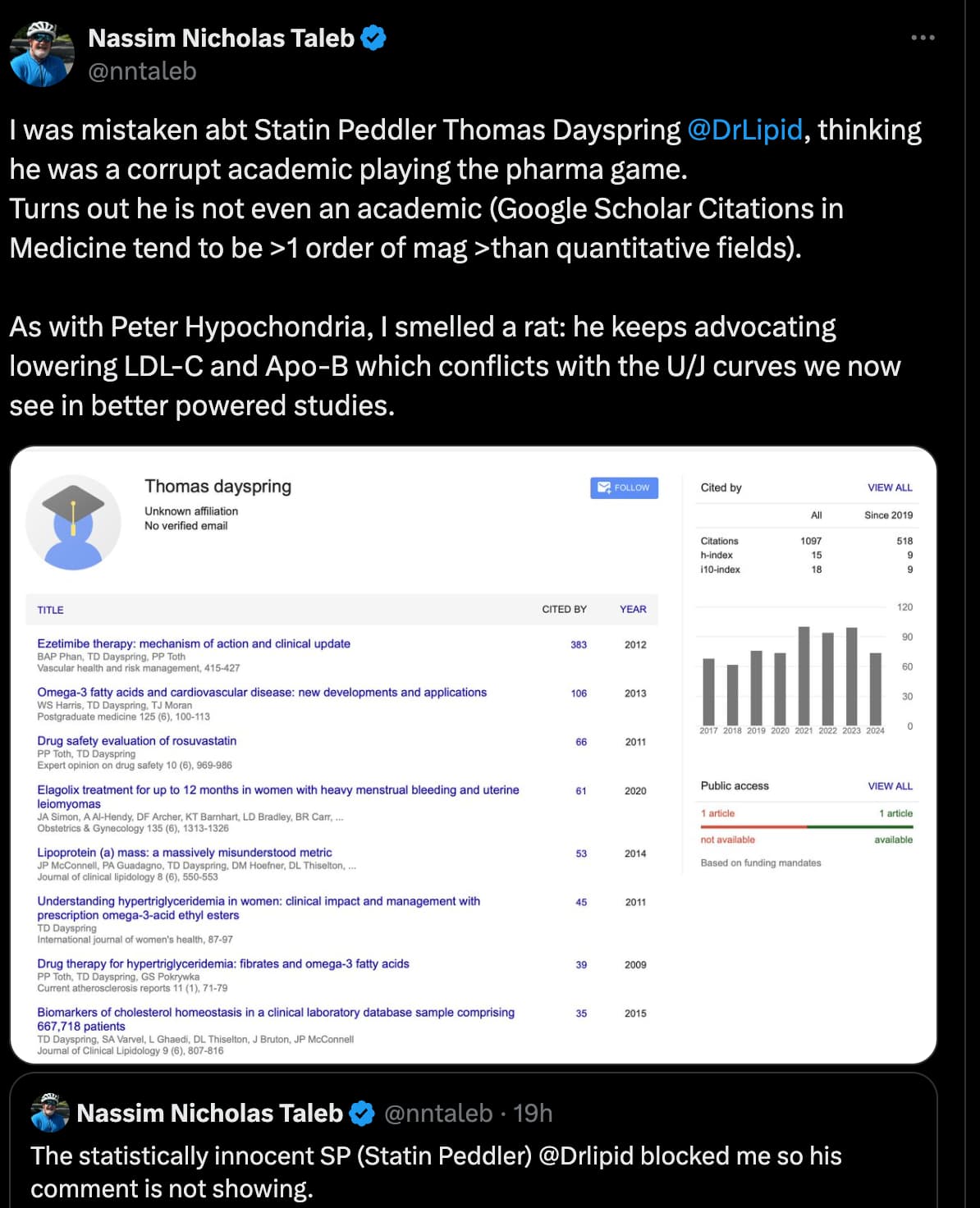
That, however, is an ad hominem attack. I am relatively open minded on statins and the lipids debate. However, if someone wishes to engage they should not use perjorative terms like statin peddler. There is a place in the uk where black swans swim in the river.
I like Nassim Taleb’s books, but I don’t necessarily follow the opinions of hedge fund managers / derivatives traders for cardiovascular advice. The name calling also doesn’t sway me towards his case.
Btw, he can’t stand being referred to like that. ![]() He hasn’t been either of those in a really long time.
He hasn’t been either of those in a really long time.
When it comes to probabilities, statistics, and mathematics, he is very intelligent, but as a person, he is extremely aggressive and makes things personal.
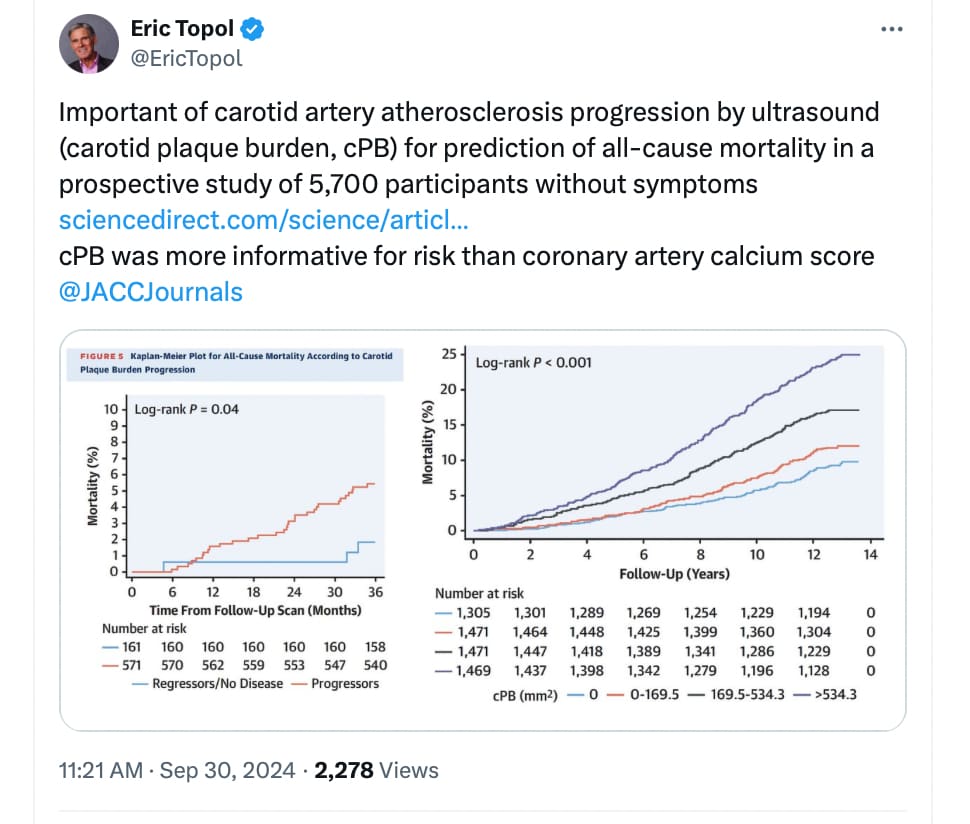
Over a median 12.4 years’ follow-up, 901 (16%) participants died. After adjustment for cardiovascular risk factors and background medication, baseline cPB and CAC score were both significantly associated with all-cause mortality (fully adjusted trend HR: 1.23; 95% CI: 1.16-1.32; and HR: 1.15; 95% CI: 1.08-1.23), respectively (both P < 0.001), thus providing additional prognostic value. cPB performed better than CAC score. In participants with a second vascular ultrasound evaluation, median cPB progressed from 29.2 to 91.3 mm3. cPB progression was significantly associated with all-cause mortality after adjusting for cardiovascular risk factors and baseline cPB (HR: 1.03; 95% CI: 1.01-1.04 per absolute 10-mm3 change; P = 0.01).
Subclinical atherosclerosis burden (cPB and CAC) in asymptomatic individuals was independently associated with all-cause mortality. Moreover, atherosclerosis progression was independently associated with all-cause mortality.
https://www.sciencedirect.com/science/article/pii/S0735109724080963?via%3Dihub