Here’s the lab report for monocytes. I have both a percentage and absolute numbers.

1 Like
@adssx do you how big the HDL effect is from flozinz? Do you think it’s helpful HDL up or just spurious (like the first gen CETP drugs seem to have perhaps been)
The effect of SGLT2i on HDL does not seem to be clinically significant: https://www.atherosclerosis-journal.com/article/S0021-9150(23)05153-5/fulltext
6 Likes
New treatment cuts cholesterol by nearly 50%, without statins or side effects
Inhibition of PCSK9 with polypurine reverse hoogsteen hairpins: A novel gene therapy approach
https://www.sciencedirect.com/science/article/pii/S0006295225002382?via%3Dihub
3 Likes
Just wanted to report that my insurance covers Nexlizet with NO prior authorization for $10/month ($25 for 90 days). I could have saved so much money by asking my doc years ago to “just prescribe it and see what happens”.
I figured for sure they wouldn’t do it since my LDL is already low and I’m on Repatha. Lesson is, don’t assume your insurance won’t cover it if you want to try bempedoic acid. And now I’ll be using the branded med rather than a foreign generic with the associated potential risks.
4 Likes
6 Likes
Consensus is that statins have a material effect on lifespan and healthspan.
Curious thoughts about this study that seems tl suggest they do for people who already have CAD but dont have a significant effect for those who dont.
So tear it apart ![]()
Which age group makes up the overwhelming majority of deaths from ASCVD? Old people.
Which age group already mostly has CAD? Old people.
Old people who don’t have any calcified plaque in their blood vessels already either have low LDL-C or are genetically protected from the negative effect of cholesterol through various mechanisms in which case statins don’t have much of an effect.
2 Likes
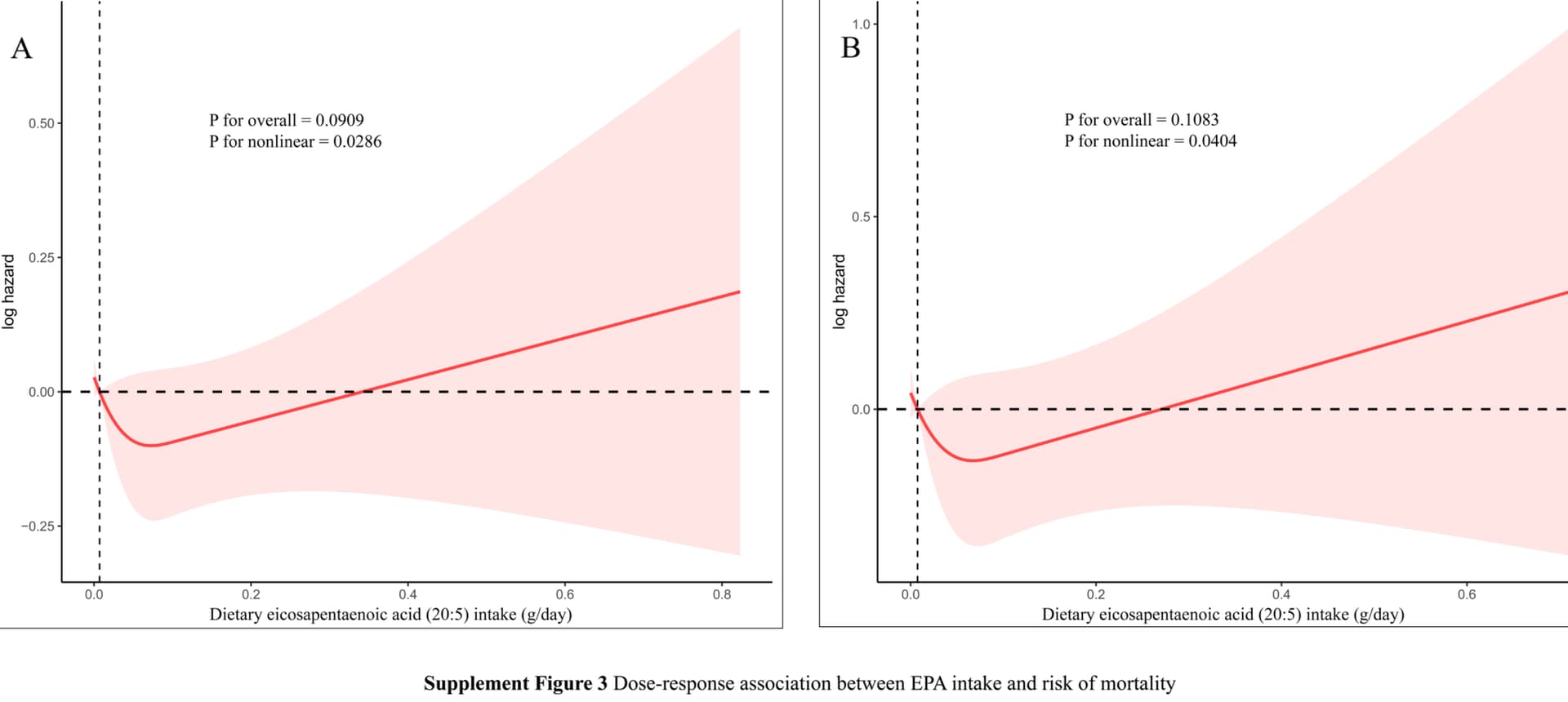
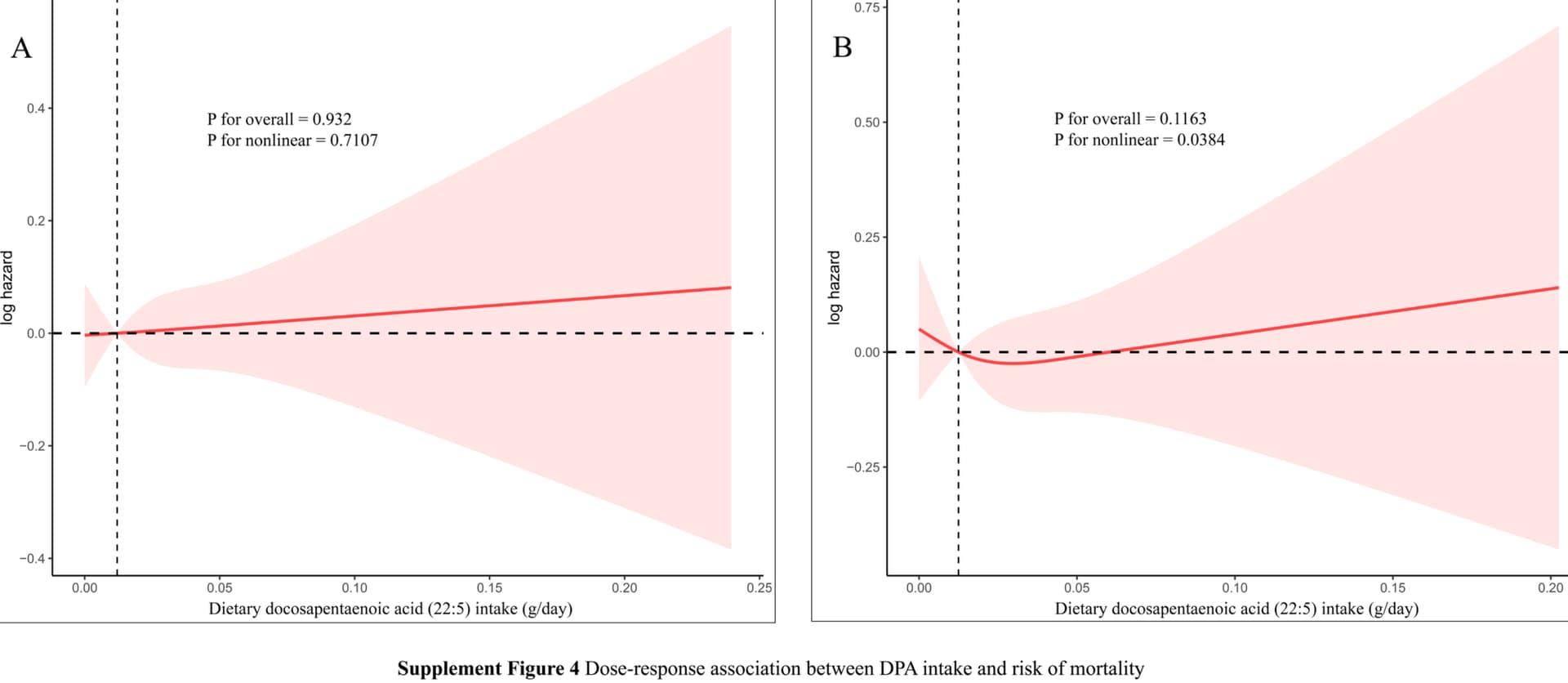
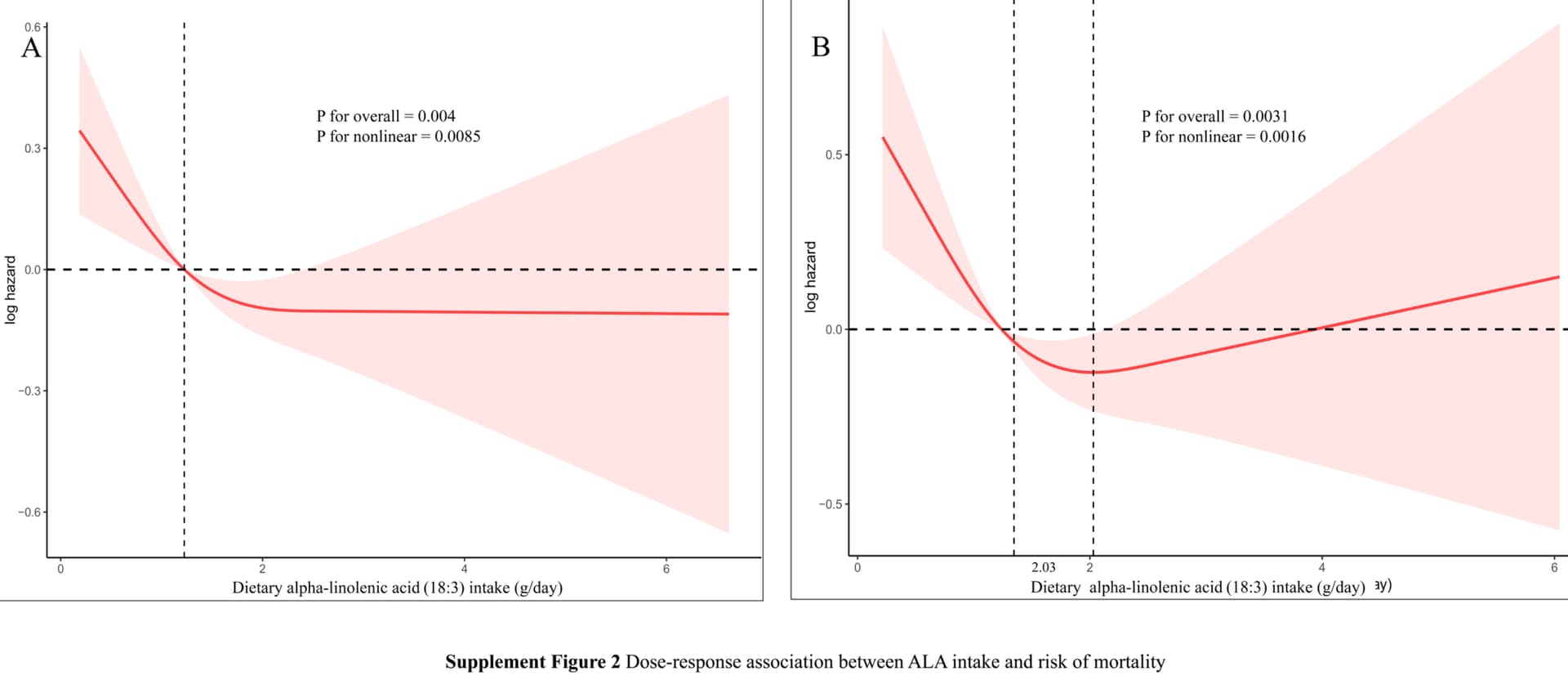
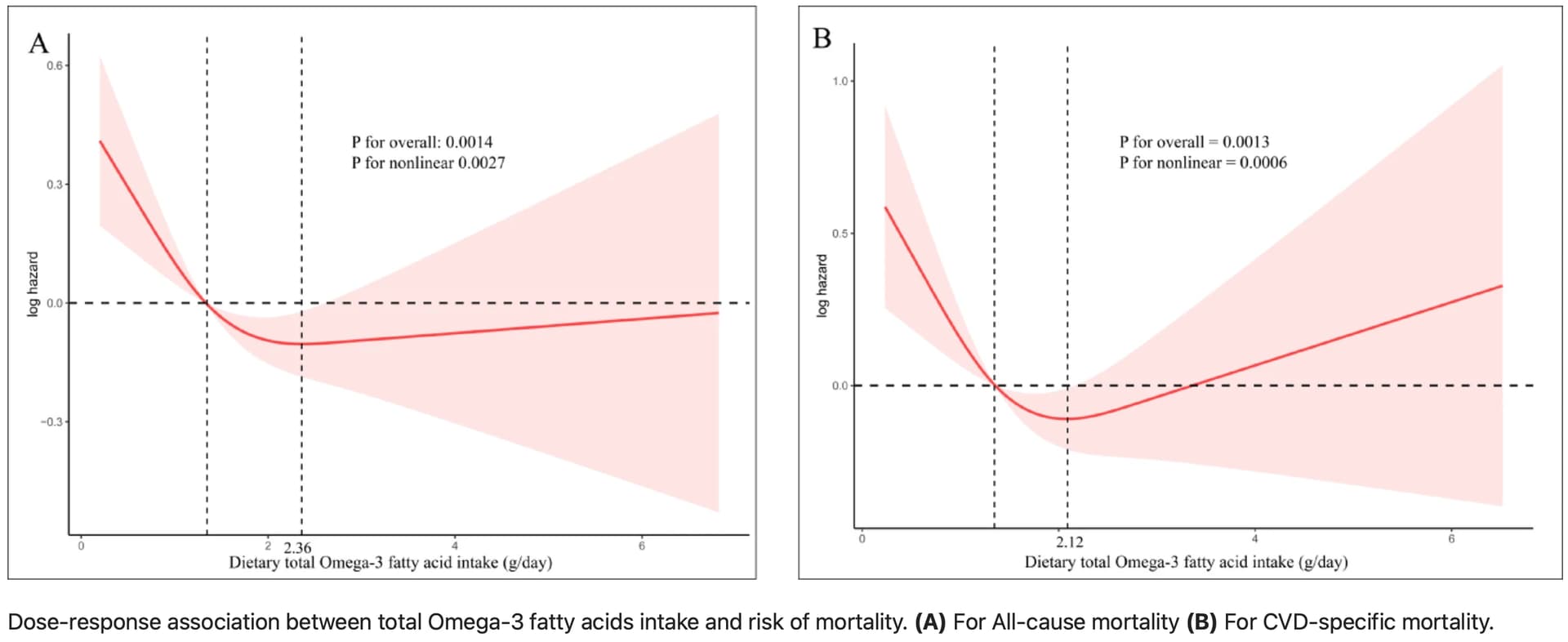
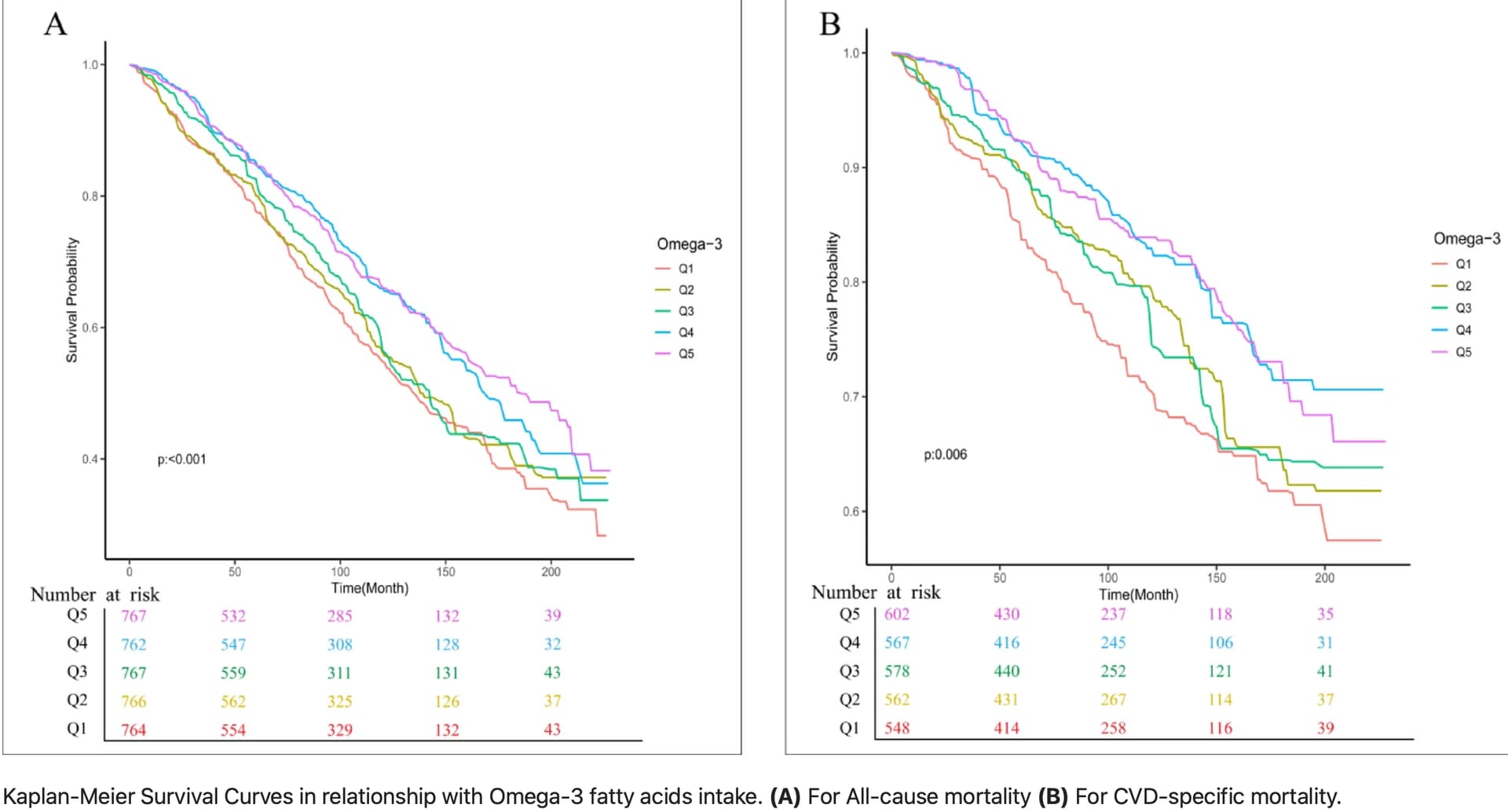
Association of dietary omega-3 fatty acids intake with all-cause and cardiovascular disease-specific mortality among individuals with cardiovascular disease
In the separate analysis of individual subtypes of the omega-3 fatty acid family, the consumption of alpha-linolenic acid (ALA) was obviously inverse-associated with CVD-specific mortality (HR of 0.64, 95% CI: 0.44–0.95). Nonetheless, the consumption of eicosapentaenoic acid (EPA), docosahexaenoic acid (DHA), and docosapentaenoic acid (DPA) did not show a significant association with mortality risk (P > 0.05).
In the dose-response relationship analysis, total omega-3 fatty acid intake and ALA intake were observed to have an “L”-shaped nonlinear relationship with cardiovascular mortality, with the inflection points at 2.12 (g/day) and 2.03 (g/day), respectively. In summary, our research indicates that both total omega-3 fatty acids and ALA are inversely linked to the risk of all-cause mortality and cardiovascular mortality in patients with CVD.
We recommend a daily intake of 2.12 g of total omega-3 fatty acids, with an optimal intake of 2.03 g/day for ALA for CVD patients.
Open access paper:
6 Likes
Does this mean we should swap out Omega-3 fish oil for ALA? I take 2 g a day of Omega 3 fish oil and I wonder if switching to ALA makes sense.
3 Likes
Another data point for @adssx 's crusade against DHA.
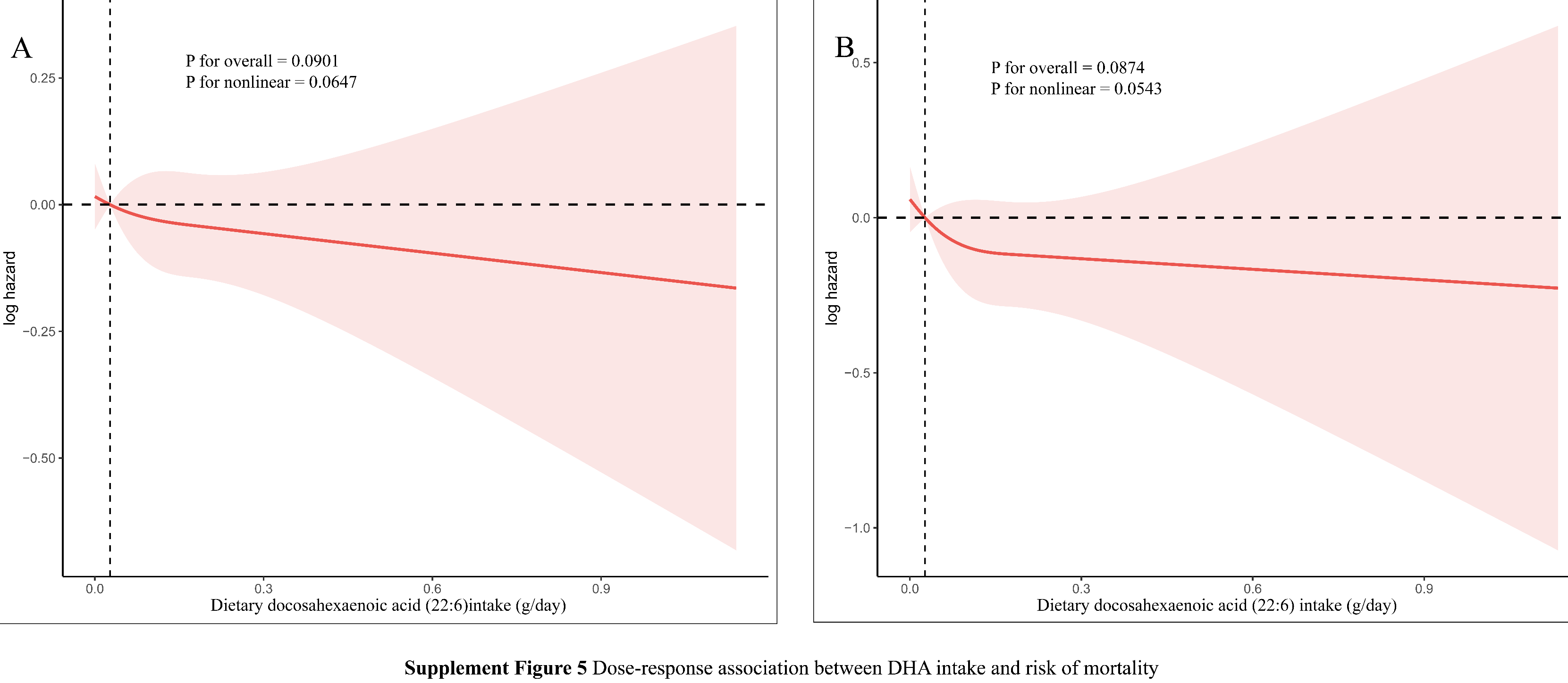
EPA looks somewhat better
DPA not so good either
Surprisingly ALA is somewhat good.
Total Omega 3 are important though.
As confirmed by the KM plots.
7 Likes
It’s easy to get enough ALA by adding 1 teaspoon of chia seeds and 1 teaspoon of flaxseeds to your smoothie.
5 Likes
…Or to eat 50-100 gr walnuts per day, providing you are not restricting calories.
3 Likes
A bit of a bummer for the men in the crowd here:
Men may need to exercise twice as much as women to achieve the same reduction in coronary heart disease risk, according to researchers, who say healthy living guidelines should take account of the sex differences.
Scientists analysed physical activity records from more than 80,000 people and found that the risk of heart disease fell 30% in women who clocked up 250 minutes of exercise each week. In contrast, men needed to reach 530 minutes, or nearly nine hours, a week to see the same effect.
The study builds on previous work that suggests women benefit more than men from the same amount of exercise, but that women are generally less physically active and less likely to meet recommended exercise targets.
3 Likes
In my opinion, this isn’t much or unattainable. A normally active day, my Apple Watch shows 75-90 minutes of exercise. I walk the dogs and take my bike to and from work. If I add intentional exercise like running, hiking, weightlifting, yoga, or Pilates, I’m way over that. So, living a normal, active life without taking a car everywhere, and climbing a fair amount of stairs would be enough.
3 Likes
How many steps does your watch show in a normally active day?
7500 or something like that, that is average. However, I take my bike to work and back, go to the gym, and basically everywhere else. Since my job is sedentary, most of my steps come from dog walking.
That’s a good baseline considering you do much else on top of it. I’m asking since my watch shows pretty high step counts even when I don’t do any treadmill or long walks, I’m talking about 15K or 20K. But probably that’s because of walking up and down the home which is not a small one, plus the garden around, rarely sitting down and somoetimes walking dogs around the garden and outside of it.
I’m amazed that simple daily activities can provide such baselines, but it seems to be pretty accurate.
3 Likes
Please, what was your dosage and protocol?
1 Like
BTW these are the papers on which I based my hypothesis about IGF-1 LR3. Can anyone get the full text of the 2023 paper??
4 Likes