Nice problem to have though!
2 Likes
Fabulous community, and a wealth of extremely valuable information - very happy to have found this site!
It seems there’s a very heterogenous group of folks here interested in life/health extension, quite diverse in age, background and health status. However, some themes appear to weave through pretty consistenty - in particular the search for interventions, pharma interventions that may assist in health/life extension.
In this spirit, I wonder if it makes sense to pin a post centered around one agent or class of agents to which one may make continuous contributions so that all info is gathered in one place.
As an example, SGLTi agents - most of the info is naturally found regarding individuals who have some kind of morbidity - such as DMT2, HF, obesity, metabolic syndrome etc. - that’s where most of the studies are focused on, given that it’s a medication that was developed to treat a condition and not for longevity purposes.
However, most - or at least many participants here - do not have such morbidities. So, the pinned post that’s gathering info, might focus on results in humans (or mammals) who are not obese/significantly overweight, diabetic, with heart failure. Results which pertain to those who have such conditions may not apply to those who are relatively healthy.
We know that canagliflozin extends lifespan in male mice in the ITP. Great. But we cannot assume that a result that works for someone with HF will have a beneficial effect for someone with a healthy CV system. There are many examples of results that don’t apply. In one of the studies (sorry, don’t remember which, there are so many in this thread!), for example, SGLT2i slightly lowered BP in nearly normotensive individuals - a good effect, seemingly, but strikingly, that reduction in BP didn’t translate into traditional benefits associated with appropriate size decline in stroke numbers. In other words, that positive biomarker change didn’t deliver the expected benefits the way it did when the lowering of BP was achieved with traditional drugs for that purpose. So we must be very careful in making sure that we don’t simply assume benefits from biomarkers, but focus on outcomes IN HEALTHY individuals.
Thus we could try to gather in one post/place all the research which shows a positive result in HEALTHY individuals - there won’t be that many studies, so it shouldn’t be too unwieldy. As to healthy, we can give it a bit of leeway - for example, we can include results for folks who are slightly overweight (say BMI above 25) or prediabetic (I am pre-diabetic, A1c anywhere from 5.6 to 5.9 over the years, and FBG as high as 115 in the morning). Having such info all in one place might make it easier for most of us to make a decision - or make a more informed decision - as to whether it makes sense to start taking such an agent. We could make such a post centered around any given agent - SGLTi, acarbose, rapa etc.
The advantage would be that it’s all in one place and all more relevant to most of us, rather than having threads with 1000+ posts, most of which deal with results in folks with profound morbidities with doubtful/uncertain relevance. Nothing wrong with having such posts, but just throwing in a suggestion of maybe having a central place for each agent, which is more compact and more relevant. Just a thought.
However, I want to emphasize yet again, what an amazing community this is and how much relevant info there is!
FWIW, to introduce my case: I am a white male, 66 years old, healthy, but for some key numbers going in the wrong direction for the past 5 years or so. My lifelong suboptimal lipids - high LDL and ApoB, very high Lp(a), but also high HDL, trigs low/normal. I’m on atorvastatin 10mg/day. My calcium score at age 65 was 0. My blood sugar not good: A1c as high as 5.9, fasting blood glucose 115 in the morning, though no very large excursions beyond 140 post prandial. My blood sugar seems to spike dramatically after exercise. Excellent diet (if I say so myself), Mediterranian, pescatarian, avoid red meat. Regular exercise aerobic & weights.
I’m interested in life/health extension. Right now I’m only on atorvastatin 10mg. Interested in going on bempedoic acid + zetia, acarbose + emagliflozin, rapamycin. My doctor is a nice guy but ultraconservative, so I can’t get anything prescribed beyond the most conservative SOC.
It is with that in mind that I am trying to absorb as much info as I can so I can make a decision as to which agents I should focus on (and then go the India online pharmacy route). I want to get on the train sometime this year and next, as at 66 my time is running out. Thank you for reading, and my apologies for the length!
10 Likes
Hi, and welcome to the forums. Thanks for the thoughtful post. I agree that we have a problem that most of the research on all these medications that appear to be longevity drugs is on “sick” people, not in healthy people so the degree of translation is at best uncertain.
I generally don’t “pin” posts at the top of the forum because the top of the forum would quickly get filled with posts that are not of relevance to many people. But what I do is add the best and most interesting posts to the FAQ on our site so they are relatively easy to find: Rapamycin Frequently Asked Questions (FAQ)
Regarding the specifics of finding research on healthy subjects related to the use of these specific medications (e.g. SGLT2 inhibitors, rapamycin, acarbose, etc.), the issue is actually much worse than you’ve suggested (I think). It isn’t just that “most” of the research is in sick people, its that virtually all the research is in sick people. Off the top of my head I can’t think of a single research study on SGLT2 inhibitors in otherwise health individuals (perhaps @adssx can remember if there are any in healthy people). The ITP study showing greatly increased longevity (in male mice) for canagliflozin was a relatively short time ago (a few years) but prior to that I don’t think there was much reason to even consider doing an SGLT2i study in healthy populations of people. And pharma isn’t typically in the business of doing clinical trials of medications in healthy populations (I’m not sure the FDA would even allow these right now).
And, for many of these drugs the issue is even greater; they are off patent (like rapamycin, acarbose, etc.) so there is no financial incentive for anyone to do any significant clinical trials at all, let alone in healthy people. There are some small clinical trials being done by academic centers, or other groups (eg. the PEARL study of rapamycin) that are in healthy populations, but the size of these studies is tiny compared to the typical Phase 3 clinical study, so they are unlikely to “move the needle” in a clinical sense for most physicians who are used to looking at large phase 3 clinical study results.
So, while I’m all for gathering up the healthy human clinical trial results in a single thread for each of the leading compounds, I think most of us have been looking at the 99% of the research that is in sick populations with the hope that we can glean some valuable information from them despite the fact that they are not in the healthy populations as we would prefer.
In the future, if we do find or see a new study based on a healthy population, please flag them as such and as we get them I’ll definitely create a thread for the clinical studies in healthy population thread, and include the link in our FAQ.
8 Likes
Off the top of my head I can’t think of a single research study on SGLT2 inhibitors in otherwise health individuals (perhaps @adssx can remember if there are any in healthy people).
There was an AgelessRx trial on canagliflozin in healthy people earlier this year. It was a small n trial, so I don’t know if they were powered for any reasonable efficacy signal, but I suppose we’ll learn what they found eventually.
3 Likes
It stills reduces BPV, which is as important if not more than mean BP: Effects of dapagliflozin on blood pressure variability in patients with prediabetes and prehypertension without pharmacological treatment: a randomized trial 2020
“we don’t simply assume benefits from biomarkers”: then how do you measure benefits?
All drugs need to go through phase 1 with healthy volunteers. So we have data on healthy volunteers. But these are biomarkers.
SGLT2i are actually an exception, as they’re approved for three conditions: diabetes, heart failure, and chronic kidney disease. So you can see that they improve glycemia for people with CKD but without diabetes and vice versa.
3 Likes
If someone asks a doctor to prescribe a SGLT2 drug, which SGLT2 medicine should one use? There are so many links and studies that it is difficult to find out the best option. Or is it even known yet?
1 Like
Our best guesses now would be either empagliflozin (which I use), dapagliflozin or canagliflozin (ITP). Each has their own advantages and disadvantages.
6 Likes
Can one still purchase from alldaychemist without a prescription?
Yes - you can purchase from any of the online pharmacies listed on this page without prescription: Buy Rapamycin Online - List of Reliable Pharmacies
1 Like
l am slow. “When all else fails, read the directions”. Many thanks.
1 Like
@Neo, on SGLT2i and cancer: A pan-tumor description of the genomic, transcriptomic, and immunological landscape of sodium-glucose cotransporter-2 (SGLT2) and association with clinical outcomes 2024
SGLT2 has been identified as being overexpressed in a diverse set of cancers. Retrospective data has demonstrated a correlation between the use of SGLT2 inhibitors and a reduced incidence of lung cancer. We explored the association of SGLT2-coding gene SLC5A2 with the transcriptomic, genomic, immunological landscape and outcomes in a subset of solid tumors.
SCL5A2-H across all investigated tumors was associated with increased immune infiltrate and a T cell-inflamed phenotype in addition to improved survival in multiple cancer types. Future research on SGLT2 should delineate its role in cancer formation versus its association as a potential positive prognostic marker.
So high expression of SGLT2 (through the SLC5A2 gene) is associated with better immune response and improved survival in several cancers? This could imply that inhibiting SGLT2 might reduce these beneficial effects? Or did I misunderstand ![]()
2 Likes
Randomized Trial of Empagliflozin in Nondiabetic Patients With Heart Failure and Reduced Ejection Fraction: the study concludes that empagliflozin significantly improves heart function, exercise capacity, and quality of life in nondiabetic HFrEF patients, supporting the use of SGLT2 inhibitors in this population regardless of their blood sugar levels.
My n=1: after couple of weeks on empagliflozin - I have measurable progress in zone 2 training (but 10mg is too much for me).
6 Likes
Please share any measures you think you can point to…
1 Like
Yes, with pleasure. For me, it is difficult to run in zone 2 at a meaningful speed. Even a minimal slope in “my” forest, where I always run, would catapult me into zone 3 or even higher. On the days when I take empagliflozin, my heart rate in cardio mode drops by 10-15 beats per minute, allowing me to run at a higher speed or overcome slopes without having to walk or leave zone 2 (which, in my case, ends around 130 bpm). And for those, who has difficulties running in zone 2 - knows, that is big change.
6 Likes
@adssx - hmm, I read it as SGLT2i inhibiting cancer formation. If SGLT2 is overexpressed in cancer, inhibiting it seems like it should inhibit cancer rather than promote. And if SGLT2i promote T-cell infiltration of the tumor, then it’s promoting an immune response, and so increaing survival of the patient. That’s how I read it, but if course I could be wrong.
3 Likes
Have you noticed a reduction in your resting heart rate on empagliflozin?
No, no noticeable changes. My resting HR is already rather low with 53 bpm, and no further improvement. It seems, that empagliflozin improves for me efficiency or cardio system.
2 Likes
We have reported that initiation of SGLT2 inhibitors can dramatically improve severe hypomagnesemia in patients with or without diabetes. As noted in a recent review, meta-analyses of randomized clinical trials have reinforced that SGLT2 inhibitors decrease the risk of hyperkalemia and correct hypomagnesemia.
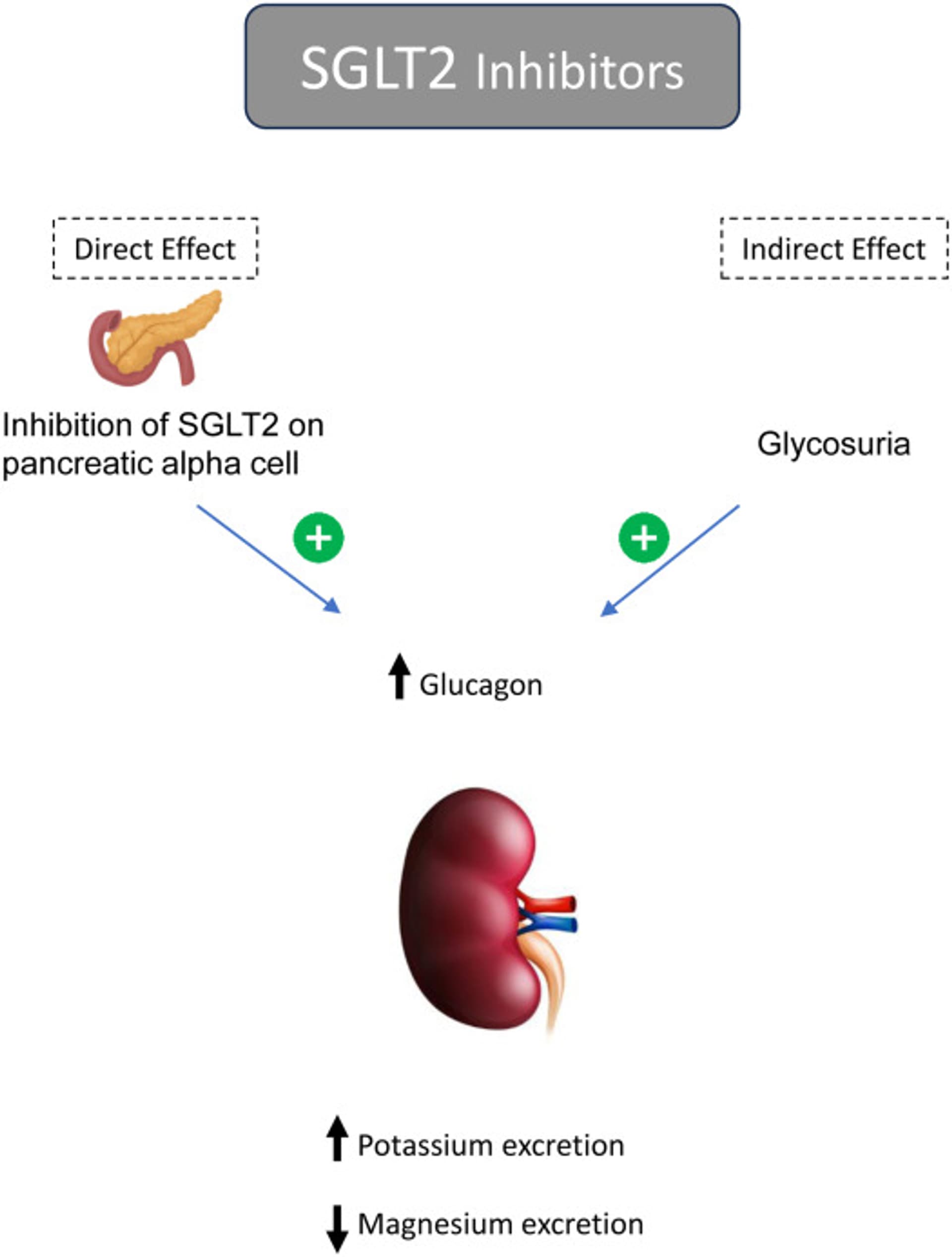
Sodium/Glucose Cotransporter 2 Inhibitors and Magnesium Homeostasis: A Review 2024
The beneficial effect of SGLT2 inhibitors on magnesium balance in patients with diabetes with or without hypomagnesemia has been noted as a class effect in recent meta-analysis data from randomized clinical trials. Some reports have demonstrated their role in treating refractory hypomagnesemia in patients with or without diabetes.
After propensity score matching, compared with the non-SGLT2i group (n = 2813), the SGLT2i group (n = 707) exhibited significantly lower recurrent IS rates (3.605% per year vs. 5.897% per year; hazard ratio: 0.55; 95% confidence interval: 0.34–0.88; p = 0.0131) and a significant reduction in all-cause mortality (5.396% per year vs. 7.489% per year; hazard ratio: 0.58; 95% confidence interval: 0.39–0.85; p = 0.0058). No significant differences were observed in the rates of acute myocardial infarction, cardiovascular death, heart failure hospitalization, or lower limb amputation.
Among 44 651 patients, 22 100 initiated SGLT2is, and 22 551 began DPP4is. After weighting, the incidence rate of MLO in the SGLT2i group was 3.8 per 1000 person-years, and it was 3.9 per 1000 person-years in the DPP4i group, resulting in an adjusted hazard ratio (aHR) of 0.82 (95% CI, 0.60-1.10). SGLT2i initiation was not associated with cirrhosis (aHR: 0.77; 95% CI, 0.55-1.06) or hepatocellular carcinoma (aHR: 0.99; 95% CI, 0.47-1.83) separately. Subgroup and sensitivity analyses did not yield significant results.
Our study helps fill this knowledge gap by indicating that SGLT2is do not lower the risk of cirrhosis or HCC compared with DPP4is. This finding is in contrast to previous research, including a systematic review and meta-analysis of randomized controlled trials showing that dapagliflozin improves liver studies, such as alanine aminotransferase (ALT) and aspartate aminotransferase levels,31 and the E-LIFT trial, which found that empagliflozin reduces liver fat and improves ALT levels in T2D and MASLD patients.
Disappointing paper on liver function. However, all the HR, even though not statistically significant, are on the side of SGLT2i benefits. We’ll have to wait for the ongoing trials of SGLT2i in NAFLD…
6 Likes
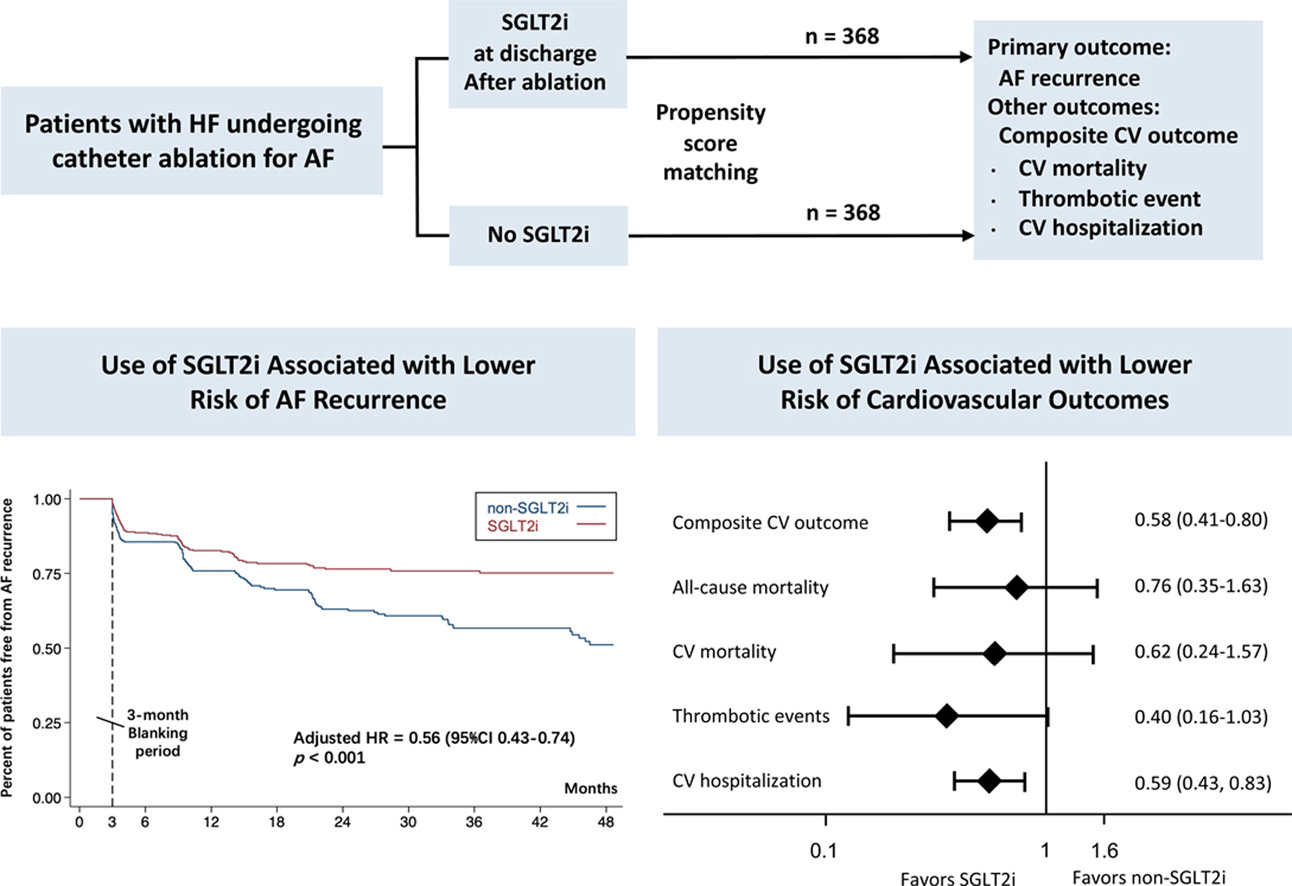
SGLT2i was associated with a lower risk of AF recurrence (adjusted HR = 0.56, 95% CI: 0.43-0.74, P<0.001). The composite risk of cardiovascular death, thrombotic events, or cardiovascular hospitalization was significantly lower in the SGLT2i group compared with those without SGLT2i (adjusted HR = 0.58, 95%CI: 0.41-0.80, p = 0.001). Although there was a trend toward benefits, the differences in all-cause mortality, cardiovascular death, or thrombotic events were insignificant between the 2 groups.
In European populations, SGLT2 inhibitors were significantly negatively associated with TC (OR 0.051, 95% CI 0.006–0.465, P = 0.0082) as well as PTC (OR 0.034, 95% CI 0.003–0.411, P = 0.0079), while no correlation was found with FTC. These findings remained consistent even after applying the Bonferroni correction.
That OR!!!
Five RCTs reporting data for 11,211 patients were included in our study. The mean follow-up duration was 43.8 weeks. Our pooled analysis showed that SGLT2 inhibitors significantly reduced the risk of hospitalisations for heart failure (HHF) (RR = 0.76, 95% CI: 0.61–0.88, p = 0.001) in patients with MI. However, the risk of all-cause mortality (RR = 1.05, 95% CI: 0.78–1.41, p = 0.76), CV mortality (RR = 1.04, 95% CI = 0.84–1.29, p = 0.73) and all-cause hospitalisations (RR = 1.06, 95% CI: 0.96–1.17, p = 0.25) remained comparable across the two groups.
6 Likes
on a potentially negative note, I think one of the meds I’ve been taking out of jardiance/rapa/telmisartan/simvastatin/ezetimibe/acarbose may have been contributing to some noticeable muscle loss for me. I’m suspecting the jardiance?
https://www.nature.com/articles/s41598-022-21486-9
I’ve read statins could potentially be at play as well. is this something to watch for?
1 Like