Yes I forgot to mention that you probably should have a glucose monitor to check that you are not depleting your sugar level. I have a chocolate addiction so … I am not saying you should eat large amounts of chocolates… maybe take 12.5mg instead of 25mg. My HBa1C was on the high side of 6.7% so I needed it to come down.
1 Like
What sort of chocolate. I can get 85% cocoa chocolate from my local co-op. Sadly today they had run out so I have had to settle for 70%.
I love the milk choclate… not into dark chocolates… LOL. I take between 100mg to 200mg of melatonin at night before I sleep. My sleep has improved from previously… but possibly lots of other factors.
4 Likes
Re. chocolate to raise blood sugar levels. I think the issue here is to keep as constant as possible the sugar levels without causing spikes, so the best choice would be to drink a solution of raw starch and water at intervals, what people affected by insulinoma do. Raw starch does raise blood sugar but is absorbed slowly, so no or little spikes.
2 Likes
Interesting. I remember fasting for 5 days on water, my glucose level was 3.8. Very borderline. Any lower and I might be in trouble. Anyway soon I’ll use the glucose monitor. I want to settle into my 3 week cycle of rapamycin. 2 weeks on and 1 week off. 2 day water fast after rapamycin. 3rd day no carb. And on the week off no carb for 3 days. I’m going to see if my sirolimus level is more consistent at 12 hours, 36 hours and 60 hours and after 180 hours. Each cycle with 4mg and 750ml GFJ 2 hours earlier. Need to get rid of my pot belly.
After 6 weeks I’ll start monitor my glucose variation. Anyway that is the plan lol. I’ve many plans before this.
5 Likes
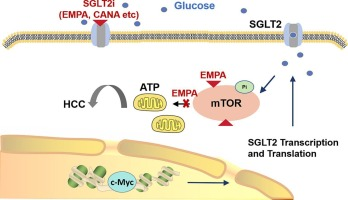
SGLT2i delays c-Myc-induced HCC progression via targeting mTOR 2025
Network pharmacology, molecular docking analyses, CETSA experiments, and additional western blot experiments were used to reveal EMPA’s interaction inhibition with mTOR.
7 Likes
Chinese paper. Hopefully good work. One thing I found odd, was that they established the presence of tumors by palpating the mice. Seems it would have to be pretty advanced to be felt by palpating. What about small tumors? How does this impact the statistics. I’m curious to see if there’s differential impact from cana vs empa.
That’s a lot of melatonin! When do you take it? Any daytime sleepiness? That dose.reputedly has anti-cancer effects.
Melatonin half life is short. Usually doesn’t stay more than 5 hours in your body
1 Like
We have a dedicated topic about melatonin: Melatonin megadoses? (And some people here take more than 1,000 mg/day btw)
4 Likes
Treatment with SGLT2i and ACEi improved cardiac function but failed to attenuate cognitive impairment, synaptic dysplasticity, and loss of dendritic spine density in MI rats. A decrease in brain glutamate level was found following MI, which can be restored by SGLT2i and ACEi. Surprisingly, only SGLT2i partially improved brain mitochondrial function.
They used dapagliflozin. Interesting @John_Hemming.
6 Likes
Have we discussed this new paper yet? The results in the abstract are pretty scary:
Conclusion and relevance: No significant effect of SGLT2 inhibitors on nervous system disorders was observed. There was reduced risk for Parkinson’s Disease observed in some specific populations. In addition, the risks of empagliflozin and dapagliflozin concerning syncope and carotid artery occlusion/carotid artery stenosis are worth attention.
3 Likes
Interesting…
1 Like
We discussed it here (and after): Canagliflozin - Another Top Longevity Drug - #1438 by CronosTempi
Chinese paper from a Tier 4 Chinese uni (ranked 201 in China: ShanghaiRanking-Univiersities ). Weird findings. For instance “dementia (RR = 1.29; 95% CI = 0.78-2.12; P = 0.32)” whereas all the papers I saw found a neutral or protective effect on dementia, so unlikely to be 1.29. I would discard the paper entirely.
6 Likes
Turkish review: SGLT-2 inhibitors on cardiac autonomic function in individuals with and without type 2 diabetes mellitus 2025
SGLT-2 inhibitors reduce sympathetic overactivity and enhance parasympathetic tone.
SGLT-2 inhibitors boost RMSSD and SDNN and lower the LF/HF ratio.
Use of SGLT-2 inhibitors offers anti-inflammatory, endothelial, and baroreceptor benefits.
Standardized HRV studies and nonlinear analysis required
4 Likes
I wonder if they ever explore how long and at what dose of any given SGLT2i do you have to be exposed to in order to register these various effects. Example, 2 years of 25mg/day empagliflozin results in 0.83 HR for heart failure or whatnot. And so on for each effect. It stands to reason that the time of exposure will differ for various effects. I also wonder if the time is different for diabetics and nondiabetics.
1 Like
Did your HRV change after starting SGLT2i?
Anyone else have the before after date on that?
Unfortunately I don’t have the before/after. But @Davin8r ran the test the other way around: Canagliflozin - Another Top Longevity Drug - #1295 by Davin8r
1 Like
Can you look back at your HRV to see if it changed when you first started emp also?
@RapAdmin - I believe you cycle on and off sglt2i, do you see anything in your HRV data?