Thanks for the link. Nice to see I’m not as bad as I thought I was.
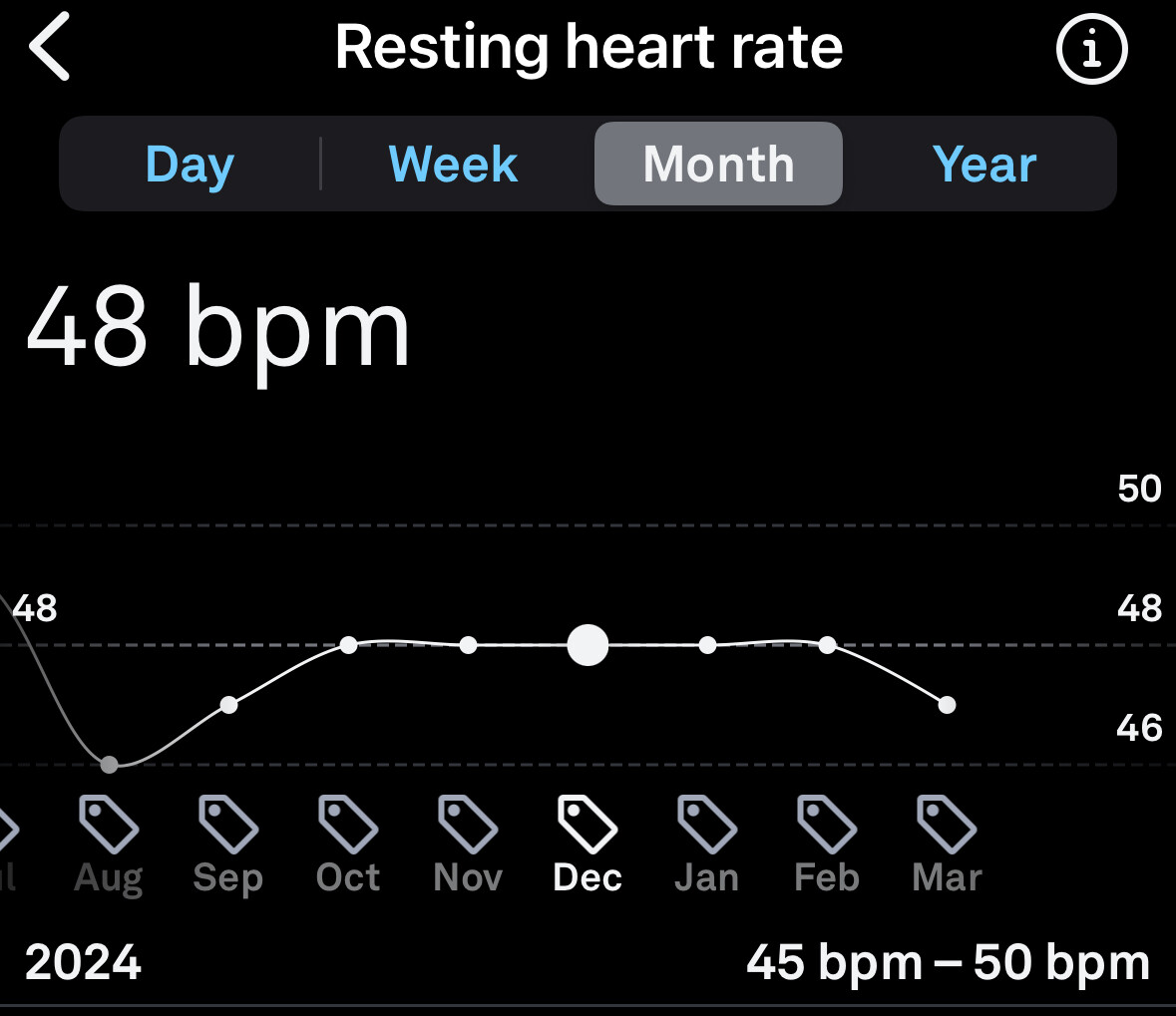
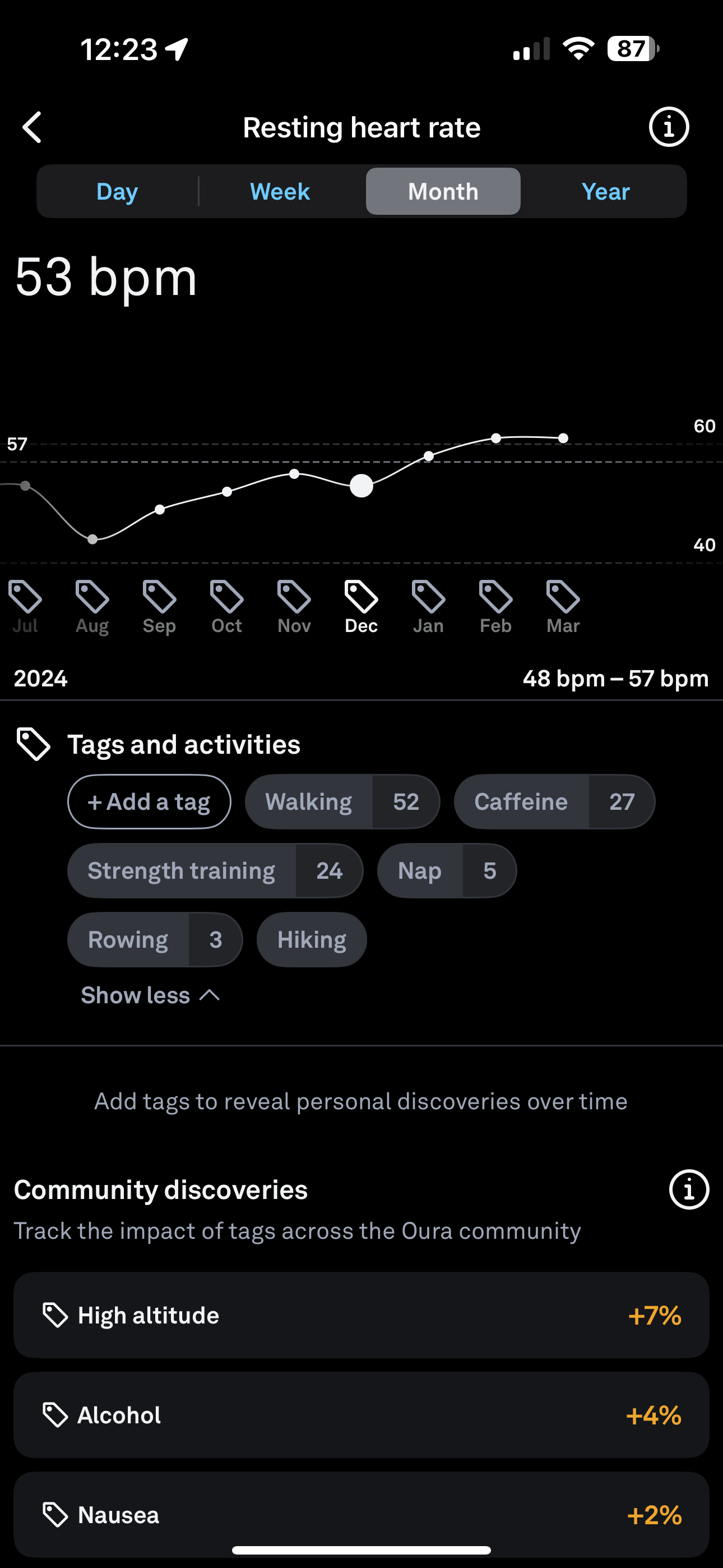
My lowest HR during sleep, as shown in your chart, is higher than the average (sometimes in the high 50’s but usually low 60s), but my average HR seems to be exactly average… never has being average sounded so good
And your HR is incredible!!! Along with @John_Hemming
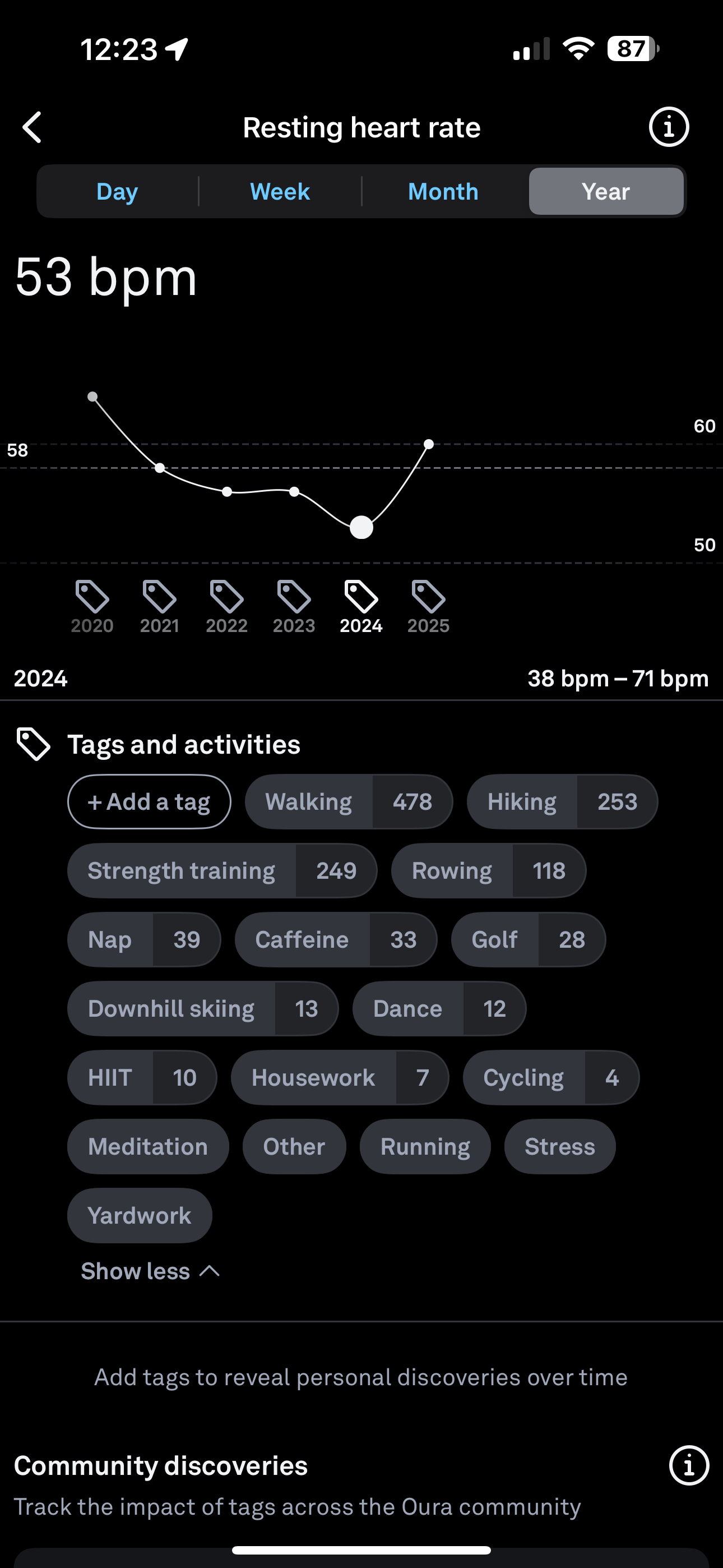
Thanks for the charts…your data is interesting in the very limited range of your 2025 HR….presume you have a good sleep protocol and are consistent.
In contrast,Oura has my range 41-64 (47 average)
My HR varies based on cardio activity over long term. For example, during 2020 COVID I biked frequently (annual HR 46) but from 2021-23 didn’t train much (annual HR 51 each year). Last year began running and HR returned to mid 40’s (45 annual) and tapered this year (47).
Late snacks/alcohol/stress = high overnight HR IMO
Altitude seems to have a big impact on my RHR/HRV. I spent all of January skiing and a couple weeks in March and also spent some time in Mexico City, all of which had an immediate effect on my RHR/HRV. Combine that with an increase to 7.5mg of Tirzepatide and that likely explains a significant portion of the average increase for 2025. We’ll see if some consistent training will bring it back down over the year now that I’m done skiing for the season.
Michael Lustgarten has a video or two on this topic and how it changes across age and how it is associated with mortality - you might want to look at that (they tend to just quite short and sweet)
Thanks for that, Davin8r. Tofogliflozin indeed sounds interesting. It is apparently even more selective of SGLT-2 compared to SGLT-1 than empagliflozin. It’s nice wrt. the nocturia, but ultimately what’s really of interest is how it compares to other SGLT2i in various settings, whether glucose control, CV benefits etc. I have not done a deep dive on tofogliflozin, but I did note this paper:
Tofogliflozin long-term effects on atherosclerosis progression and major clinical parameters in patients with type 2 diabetes mellitus lacking a history of cardiovascular disease: a 2-year extension study of the UTOPIA trial
This review identified several key mechanisms by which SGLT2 inhibitors may benefit the heart directly, including reductions in oxidative stress, inflammation, and myocardial fibrosis. Emerging evidence suggests that these drugs modulate key pathways such as sodium-hydrogen exchange (NHE) inhibition, improvement of mitochondrial function, and promotion of ketone body utilization in cardiomyocytes.
SGLT2 inhibitors appear to confer direct cardioprotective effects. These include anti-inflammatory, anti-fibrotic, and energy efficiency improvements in the myocardium. The findings highlight new potential therapeutic mechanisms and provide a foundation for further research into the non-diabetic use of SGLT2 inhibitors in heart failure and other cardiac conditions. Understanding these direct effects could lead to optimized treatment strategies for patients with and without diabetes.
GLT2is significantly reduced dementia risk and mortality compared to metformin in T2D patients. These findings suggest SGLT2is may offer superior neuroprotective benefits, underscoring their potential as a first-line therapy for T2D. Further randomized trials are needed to confirm these results.
Nice find. It’s association, but still, the numbers are impressive. Are SGLT2i very good or is metformin very mediocre?
“Results
- Among 74,975 matched patients in each cohort, SGLT2i use was associated with a lower incidence of overall dementia: 2.7% vs. 6.9%: adjusted hazard ratio (aHR) 0.80 [95% CI 0.76;0.84]. Reductions were observed in vascular dementia (0.8% vs. 2.0%; aHR 0.87), Alzheimer’s dementia (1.1% vs. 3.2%; aHR, 0.76), and all-cause mortality (6.8% vs. 15.4%; aHR, 0.92). Benefits were pronounced in older adults, particularly those aged ≥80 years.”
“Benefits were pronounced in older adults, particularly those aged ≥80 years.”
Well, you expect that since dementia (and ACM) increase with age, if there are benefits, they would be more pronounced in older adults.
What would be of interest is how long does one have to be on SGLT2i to start seeing benefits and are these a steady amount per year, or are the benefits cumulative with time beyond that steady level.
Obviously, we are talking about high risk individuals with significant morbidities. How does this map out for people on these agents who don’t have these morbidities, that’s the question for those who take them for longevity/healthspan purposes.
They make a point that of course these are associations, but the RCTs are inconsistent. One wonders about the numbers of people in these RCTs, if adequately powered.
“[…] this association remains unconfirmed due to inconsistent findings across studies, particularly randomized trials.”
Impact of sodium-glucose cotransporter-2 inhibitors on aging biomarkers and plasma ceramide levels in type 2 diabetes: beyond glycemic control
Results: SGLT2i-treated patients showed significantly lower CerC16:0, CerC22:0, and CerC24:1 levels (p < 0.01) and decreased 5MC and H2AX (p < 0.05) compared to non-SGLT2i patients. IGF-1 was significantly elevated in the SGLT2i group (p < 0.01), suggesting a possible protective effect on metabolic health. PCA distinguished control from diabetic groups but revealed overlap between SGLT2i and non-SGLT2i groups.
Conclusion: Beyond glucose control, SGLT2i may improve plasma Cer and aging markers in diabetic patients, supporting their broader therapeutic potential in aging and age-related diseases. Further large-scale studies are warranted to confirm these effects and underlying mechanisms.
Empagliflozin and dapagliflozin affect miRNA expressions on diabetic rat heart.
Empagliflozin and dapagliflozin may have different cardioprotective mechanisms.
Dapagliflozin shows protective effect on thoracic aortas.
SGLT2 inhibitors showed neutral cancer risk in T2DM patients but may reduce gastrointestinal cancer versus metformin, guiding tailored therapy based on patient risk profiles.
SGLT2i-treated patients showed significantly lower CerC16:0, CerC22:0, and CerC24:1 levels (p < 0.01) and decreased 5MC and H2AX (p < 0.05) compared to non-SGLT2i patients. IGF-1 was significantly elevated in the SGLT2i group (p < 0.01), suggesting a possible protective effect on metabolic health. PCA distinguished control from diabetic groups but revealed overlap between SGLT2i and non-SGLT2i groups.
Beyond glucose control, SGLT2i may improve plasma Cer and aging markers in diabetic patients, supporting their broader therapeutic potential in aging and age-related diseases. Further large-scale studies are warranted to confirm these effects and underlying mechanisms.
Unexpectedly, mechanistic studies revealed that antagonism of AMPK aggravated oxidative stress and ferroptosis, reduced GPX4 (glutathione peroxidase 4) level, and partially abolished the anti-hypertrophic and anti-ferroptosis effects of SGLT2i in H9C2 cells. Taken together, the regulatory role between AMPK and ferroptosis was revealed for the first time in cardiac hypertrophy. SGLT2i counteracts ferroptosis by activating AMPK, providing a sustained protection against cardiac hypertrophy. This positions SGLT2i as a potential therapeutic agent for the treatment of cardiac hypertrophy. Besides, in addition to the downregulation of AMPK in hypertrophic heart tissue, its levels are also reduced in plasma, suggesting its potential to serve as a diagnostic marker for the early detection of ferroptosis and cardiac hypertrophy.
SGLT2-i and DPP4-i enhance ketone metabolism in the brain.
SGLT2-i and DPP4-i suppress neuroinflammation and promote M2 microglial polarization.
SGLT2-i and DPP4-i inhibit NLRP3 inflammasome activation through distinct pathways.
Beautiful collection of papers, thank you Antoine!
I really hope we can dig into the disparate effects of SGLTi, because we all take different ones, and many papers that find effects lump them all together which severely limits the actionability of such findings.