First of all… note that you don’t want the regular “Clostridium Buyricum” product. See below:
Gemini Comparison of versions of Clostridium butyricum
The distinction between Clostridium butyricum MIYAIRI 588 (CBM 588) and “regular” or wild-type Clostridium butyricum is critical. While they share the same species name, they are vastly different in terms of safety and biological activity.
The short answer: CBM 588 is a specific, non-toxic therapeutic strain. “Regular” Clostridium butyricum includes wild strains that can be pathogenic and fatal.
Here is the breakdown of the scientific and clinical differences.
1. Safety: The Neurotoxin Risk (Critical)
The most significant difference is safety.
- Regular Clostridium butyricum : Some wild strains of C. butyricum carry the gene for type E botulinum neurotoxin . These strains have been identified as causative agents in cases of infant botulism (a potentially fatal paralytic illness) and necrotizing enterocolitis (NEC) in premature infants. You cannot assume a generic C. butyricum is safe.
- CBM 588: This specific strain has been genomically sequenced and proven to lack the genes for botulinum neurotoxins (types A, B, E, and F) and other virulence factors. It is one of the few strains authorized for human use by regulatory bodies (like the EU’s EFSA and Japan’s Ministry of Health) specifically because it is confirmed non-toxigenic.
2. Mechanism of Action: Unique Pathways
While all Clostridium butyricum strains ferment fiber to produce butyrate (a beneficial short-chain fatty acid), CBM 588 possesses specific immunomodulatory traits that are not guaranteed in generic strains.
| Feature | CBM 588 (Therapeutic Strain) | Regular C. butyricum (Wild Type) |
|---|---|---|
| Protectin D1 Induction | Proven. CBM 588 specifically triggers the gut to produce Protectin D1, a rare molecule that actively “resolves” inflammation and speeds up tissue repair. | Unknown/Unverified. This complex signaling pathway has not been established as a general trait of the species. |
| IL-10 Upregulation | Proven. It potently stimulates regulatory T-cells (Tregs) to release Interleukin-10 (anti-inflammatory) in the colon. | Variable. Some wild strains may actually provoke inflammation or aggravate conditions like NEC (necrotizing enterocolitis) rather than soothe them. |
| Spore Resistance | Optimized. CBM 588 spores are highly resistant to gastric acid and heat, ensuring they reach the lower colon alive. | Variable. Wild strains vary wildly in their ability to survive the stomach’s acidity. |
Export to Sheets
3. Clinical Utility and Evidence
- CBM 588: Almost all modern clinical trials regarding C. butyricum benefits (including the cancer immunotherapy trials mentioned previously) use the CBM 588 strain specifically.
- Regular C. butyricum: There is virtually no clinical evidence supporting the use of “generic” C. butyricum. If a supplement label says Clostridium butyricum without specifying the strain (e.g., “MIYAIRI” or “CBM 588”), you are rolling the dice on its efficacy and safety profile.
Summary
To treat “regular” Clostridium butyricum as equivalent to CBM 588 is scientifically inaccurate.
- CBM 588 is a pharmaceutical-grade, non-toxic probiotic with specific anti-inflammatory properties.
- Regular C. butyricum is a broad category of bacteria found in soil and stool that includes potential pathogens capable of producing neurotoxins.
Recommendation
When sourcing this for longevity or gut health, you must verify the strain. Look specifically for “MIYAIRI 588,” “CBM 588,” or “Miyarisan.” Do not use products that simply list the species name without a strain identifier.
Measuring Results of your protocol:
Therefore, the most accurate way to measure success is to ignore the “Input” (butyrate levels) and measure the “Outcome” (Gut Barrier Integrity and Systemic Inflammation).
Here is the tiered approach to measurement, ranked by ease and accuracy.
1. The “Easiest” Method (Systemic & Subjective)
This combination costs <$50 and tells you if the gut protocol is translating to whole-body health.
-
Test: hs-CRP (High-Sensitivity C-Reactive Protein)
- Why: Butyrate’s primary mechanism is sealing the gut lining to stop “Metabolic Endotoxemia” (LPS leaking into blood). If the protocol works, less LPS leaks, and your systemic inflammation (hs-CRP) will drop.
- Target: You want to see hs-CRP drop below 1.0 mg/L (ideally <0.5 mg/L).
- Timeline: Test at Day 0 and Day 45.
-
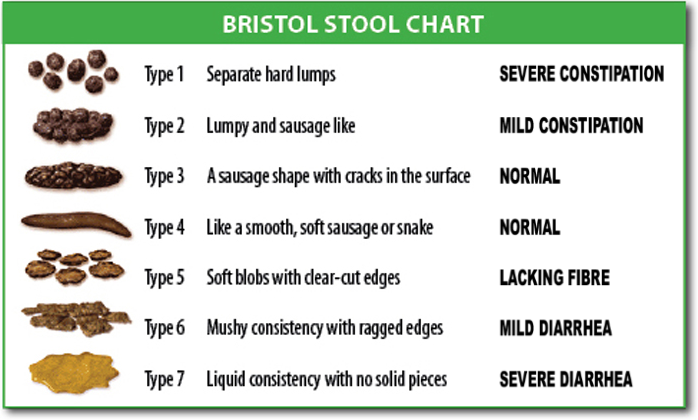
Tracker: The Bristol Stool Chart
- Why: Clostridium butyricum and green banana flour normalize water absorption.
- Target: You are aiming for Type 3 or Type 4 (smooth sausage). If you see Type 1 (constipation) or Type 6 (mushy), the fiber dose is incorrect.
2. The “Most Accurate” Method (The Barrier Panel)
If you want scientific proof that your gut lining is healing, you need specific fecal biomarkers. You will likely need to order a functional stool test (like GI-MAP, Genova, or Thorne).
-
Biomarker A: Fecal Calprotectin
- What it is: A marker of neutrophil activation in the gut mucosa.
- The Signal: Elevated levels (>50 µg/g) indicate active “fire” in the gut wall.
- Success: Butyrate is a potent anti-inflammatory. If this protocol works, Calprotectin should plummet.
-
Biomarker B: Fecal Zonulin
- What it is: The protein that regulates the “Tight Junctions” between your gut cells.
- The Signal: High Zonulin = Leaky Gut.
- Success: Green banana flour (resistant starch) specifically strengthens these junctions. A drop in Zonulin is the definitive proof that the barrier is sealed.
3. The “Engraftment” Check (Microbiome Sequencing)
If you specifically want to know if the Clostridium butyricum probiotic actually “moved in” (engrafted) rather than just passing through:
- Test: 16S rRNA or Shotgun Metagenomic Sequencing (e.g., Thorne Gut Health, Tiny Health, Ombre).
- The Metric: Look for the specific abundance of Clostridium clusters (specifically Cluster IV and XIVa) or the species C. butyricum.
- Reality Check: Probiotics are often transient. Don’t be disappointed if the specific strain doesn’t permanently colonize. As long as Biomarkers A & B (above) improve, the protocol is a success.
Summary Protocol for Measurement
| Method | Biomarker | Target Result | Cost | Accuracy |
|---|---|---|---|---|
| Blood (Easy) | hs-CRP | < 0.5 mg/L | $ | High (Systemic) |
| Stool (Deep) | Calprotectin | < 10 µg/g | $$ | Very High (Local Inflammation) |
| Stool (Deep) | Zonulin | Low Range | $$ | Very High (Permeability) |
| Observation | Bristol Chart | Type 4 | Free | Medium (Function) |
Export to Sheets
Actionable Recommendation: Start with the hs-CRP blood test. It is cheap and widely available. If your hs-CRP drops significantly over 6 weeks while on this stack, you can be 90% confident the gut barrier is healing without paying for expensive stool panels.

