I believe the quote comes from The Company.
1 Like
So, if I’m reading this graphic properly, it’s saying all of the benefits come from 2 mg/day and below? Would it be equivalent to a 12-14 mg weekly dose?
It definitely implies an inverted U-shaped curve for immunity.
2 Likes
How do we know that? Let me know if I have this backward: it would be an inverted U curve… if so that goes against a lot of the mechanistic understanding of mTOR and logic overall?
Yes, that’s how i interpret it, with the exception of endocrine system benefits. Where you could argue a slightly higher dose (3-4mg/day).
But I suspect the underlying studies aren’t compelling.
It would be useful to have a sude effect score for each of the studies too.
2 Likes
Yes exactly that. But the curve for immunity benefits (the blue circles) does appear to be ushaped. I assume its just an artefact.
1 Like
Inverted of what we normally mean by U shape. So it’s the “opposite”. There is not one single, intermediate best point. Rather there are two regions of of it getting better and better with either the lowest doses and better with the highest doses.
Its upside down because generally south on the graph is the good (lowest all cause mortality, etc), but here the good is north on the graph not down.
3 Likes
I see, yes. This is upside down compared to the usual hazard ratio graph.
This chart, showing better outcomes with either low or high dosing is odd and doesn’t make a lot of sense to me.
1 Like
Interesting info. The chart on body part by rapa dose seemed to show Rapa benefit at lower doses but the overall conclusion is negative. It’s no wonder the scientists are so slow to jump on board.
Clearly there are rapa benefits for some people. Perhaps the learning here is that rapa isn’t for everyone. If you don’t seem to get a benefit that is greater than the side effects, don’t push.
5 Likes
My assumption would be that there isn’t a u shaped immunity response curve to rapa, and that this is just an artefact of the limitations of these studies.
My assumption wouldn’t be…
Because mTOR knock-outs are embryonic lethal, we generated a viable hypomorphic mouse by neo -insertion that partially disrupts mTOR transcription and creates a potential physiologic model of mTORC1/TORC2 inhibition. Homozygous knock-in mice exhibited reductions in body, organ, and cell size. Although reductions in most organ sizes were proportional to decreased body weight, spleens were disproportionately smaller. Decreases in the total number of T cells, particularly memory cells, and reduced responses to chemokines suggested alterations in T-cell homing/homeostasis. T-cell receptor-stimulated T cells proliferated less, produced lower cytokine levels, and expressed FoxP3. Decreased neutrophil numbers were also observed in the spleen, despite normal development and migration in the bone marrow. However, B-cell effects were most pronounced, with a partial block in B-cell development in the bone marrow, altered splenic populations, and decreases in proliferation, antibody production, and migration to chemokines. Moreover, increased AKTSer473 phosphorylation was observed in activated B cells, reminiscent of cancers treated with rapamycin, and was reduced by a DNA-pk inhibitor. Thus, mTOR is required for the maturation and differentiation of multiple immune cell lineages.
Constitutive reductions in mTOR alter cell size, immune cell development, and antibody production
With the caveat that I haven’t read the paper yet and there may be something else I’m still missing:
That’s what you would expect, but the graph as drawn and as (naively?) interpreted shows a true U-shaped curve: benefits at doses up to 1.5 mg/day, neutral at2.9 mg/day, deleterious at 3 or 4.5 mg/day, neutral again at 4.75 or 6 mg/day, and beneficial again at 6 or 10 mg/day.
One thing to remember is that the Mannick papers included daily low-dose and weekly 5 or 20 mg everolimus. Since this graph plots everything in dose/24 hours, 5 mg/week would be .7 mg/24 h, and 20 mg/week would be 2.86 mg/week. That’s consistent with some of the data points attributed to Mannick in the graph, but not the 3 mg/week data point.
Again, I’ve not properly read the paper yet.
Its interesting that this is coming out the same time as the Review Paper by Andrea Maier and her group at the National University of Singapore. I would trust Andrea’s research over that of a journalist (Josh Conway, who seems to have no formal science training that I can see) at lifespan io. I love what Lifespan.io does, but they definitely aren’t experts in the area of rapamycin. It would take a fair amount of work to evaluate and compare the two summaries, and I don’t have time for that right now - but if someone else does, have at it…
I will note that a PubMed search for “rapamycin” returns about 53,900 published papers—including 3,295 clinical trials and 1,991 randomized control trials. Lifespan.IO looked at 19 papers to do their writeup. I wouldn’t be too confident that their summary is representative given the their review of only two dozen papers.
The NUS review at the top of this thread is much, much more in-depth and was produced because they are doing a rapamycin clinical trial soon and needed to summarize the state of the research for their IRB (institutional review board).
Lifespan IO says " Rapamycin and its analogs do not have many large effects on people.". But its still very early in terms of the research of rapamycin use in healthy people, so I wouldn’t put much value in any of the studies done so far (except the Mannick / ResTOR Bio studies, as they were well-funded, large phase 2 and 3 studies - but the phase 3 study had issues because the FDA changed the endpoints between the phase 2 and phase 3 studies).
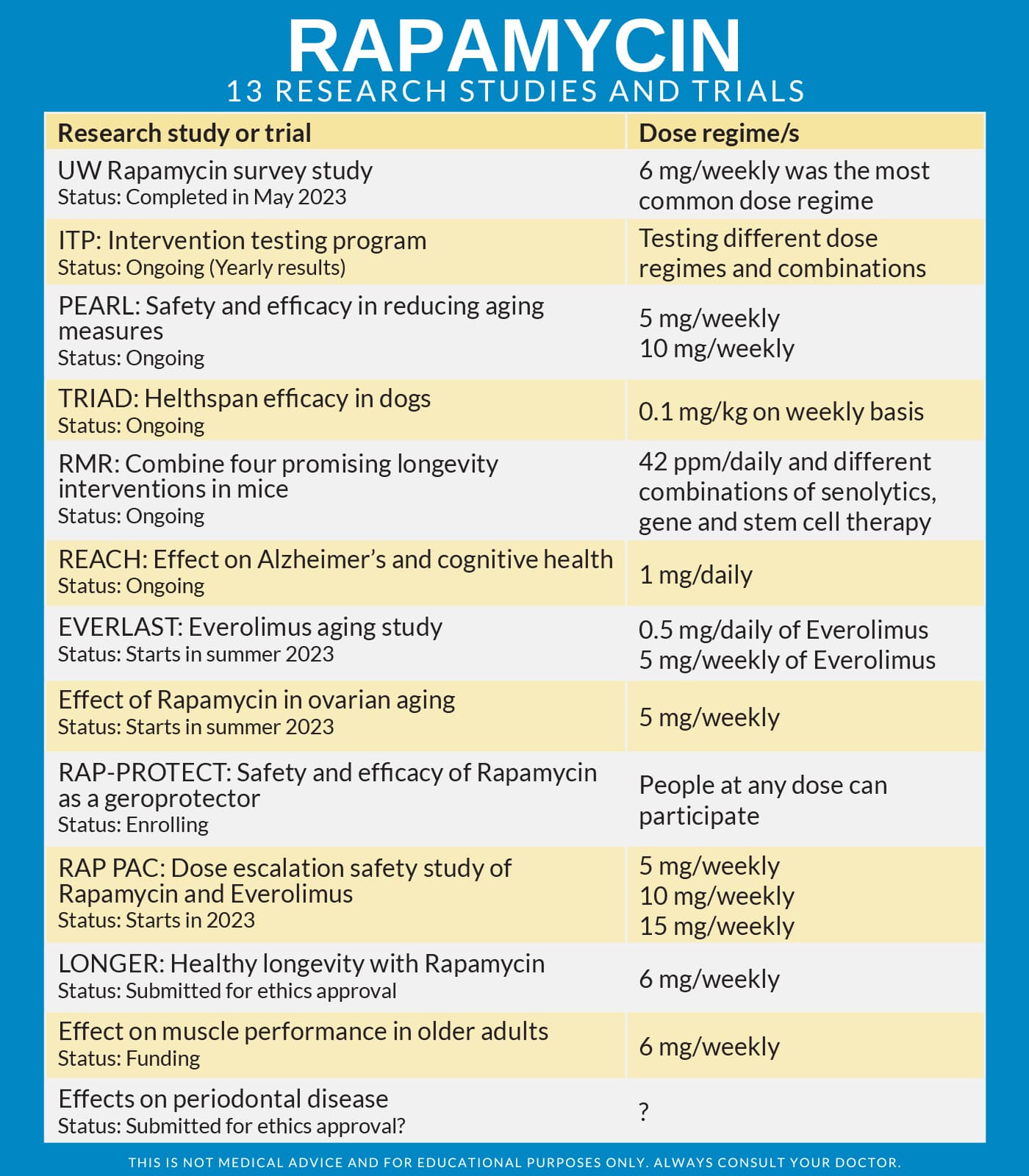
There are many studies ongoing right now, so we’ll be learning a lot more over the coming 5 years:
7 Likes
Thank you for that overview and the table of studies. Much appreciated.
https://www.thelancet.com/journals/lanhl/article/PIIS2666-7568(23)00258-1/fulltext#%20 February, 2024 Singapore
Feel free to jump in to correct any of those following statements:
The key findings from the 19 included studies on the effects of rapamycin and its derivatives on aging-related health outcomes are as follows:
- Rapamycin and its derivatives improved physiological parameters associated with aging in the immune, cardiovascular, and integumentary systems in both healthy individuals and those with aging-related diseases.
- No significant effects on the endocrine, muscular, or neurological systems were observed in the studies.
- The effects of rapamycin or its derivatives on the respiratory, digestive, renal, and reproductive systems were not assessed in the reviewed studies.
- In individuals with ageing-related diseases, there were increased numbers of infections and elevations in total cholesterol, LDL cholesterol, and triglycerides reported 1.
- Studies did not find a clear relationship between the dose of rapamycin or its derivatives and their efficacy in ameliorating aging-related outcomes 9.
- While rapamycin and its derivatives have shown benefits in animal models such as enhancing learning and memory and reducing neurodegeneration, these effects were not consistently observed in the human studies included in the review 8.
5 Likes
I see that 0.5 to 1 mg per day gives the most positive results. I don’t see any recommendation to take this dose (multiplied by 7 days) once a week. Looks like a small daily dose taken consistently every day has the most benefits.
3 Likes
Having read the whole review, I have to say I’m pretty disappointed. There are substantially more human data in age-wise “healthy” people and people with age-related diseases other than cancer or for immune suppression than I was aware of, and a discouragingly large amount of it is either null or gives signals of harm (such as some of the visual system indications).
One interesting thing is that while there are a lot of moving parts, the effects on the immune system and on rheumatoid arthritis (an autoimmune disorder) seem to be fairly consistently encouraging for everolimus but not for rapamycin itself.
Is anyone daily dosing their Rapamycin? I have to say, it’s a little more practical for me to simply take 1mg per day with the rest of my pills than take a bolus dose every once or two weeks.
A researcher at the Buck Institute, Pankaj Kapahi, takes rapamycin daily (but with regular breaks/ mini vacations). He’s the only one I know. I think he discusses it in Krister’s podcast here: New Rapamycin podcast with Pankaj Kapahi
4 Likes
I dose it daily, 0.5mg, like Pankaj Kapahi, then have a short break, but I take it for my kidney transplant.
3 Likes