Hey, does anyone know if there are products in these classes of medications that have been shown to extend life in various animal studies(quality testing like ITP etc)?
I’ve seen lithium and l-deprenyl on some of the lists/threads posted on this forum that seem to improve longevity. But that seems to be all I could see.
Seen some good posts about various MAOI’s(parnate) besides l-deprenyl.
Anyone have a list on what has been tested for longevity in regards to things like:
Specific reuptake inhibitors or modulators(serotonin/dopamine/noradrenaline/histamine/monoamines etc), tricyclic or tetracyclic antidepressants, antipsychoics, antidementia, antiparkinsons, anxiolytics, adhd/add, nootropics, or any other neurotransmitters or neuropeptides etc.??
Long-term studies have shown significantly lower mortality rates in patients with continuous clozapine (CLZ) treatment than other antipsychotics. We aimed to evaluate epigenetic age and DNA methylome differences between CLZ-treated patients and those without psychopharmacological treatment. The DNA methylome was analyzed using the Infinium MethylationEPIC BeadChip in 31 CLZ-treated patients with psychotic disorders and 56 patients with psychiatric disorders naive to psychopharmacological treatment. Delta age (Δage) was calculated as the difference between predicted epigenetic age and chronological age. CLZ-treated patients were stratified by sex, age, and years of treatment. Differential methylation sites between both groups were determined using linear regression models. The Δage in CLZ-treated patients was on average lower compared with drug-naive patients for the three clocks analyzed; however, after data-stratification, this difference remained only in male patients. Additional differences were observed in Hannum and Horvath clocks when comparing chronological age and years of CLZ treatment. We identified 44,716 differentially methylated sites, of which 87.7% were hypomethylated in CLZ-treated patients, and enriched in the longevity pathway genes. Moreover, by protein–protein interaction, AMPK and insulin signaling pathways were found enriched. CLZ could promote a lower Δage in individuals with long-term treatment and modify the DNA methylome of the longevity-regulating pathways genes.
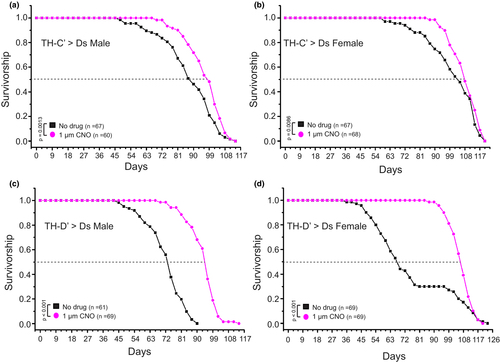
Figure 2. Moderately activating the ectopically expressed DREADD system in the TH-C’ or TH-D’ DANs extends lifespan in flies. Survivorship curves of male and female adult flies expressing the DREADD Gαs receptor and raised on food containing DMSO only (No Drug) or 1uM Clozapine N-oxide (CNO). (a, b) moderately activating the DREADD-Ds receptor in the TH-C’ neurons leads to an extension of lifespan in flies. The median lifespan increased from ~87 days to ~98 days (~12.6% increase) in the male flies and from ~95 days to ~108 days (~12.6% increase) in the female flies. (c, d) moderate activation of the DREADD-Ds receptor expressed in the TH-D’ neurons leads to a significant extension of lifespan in flies. The median lifespan increased from ~73 days to ~95 days (~30% increase) in the male flies and from ~67 days to ~107 days (~50% increase) in the female flies?
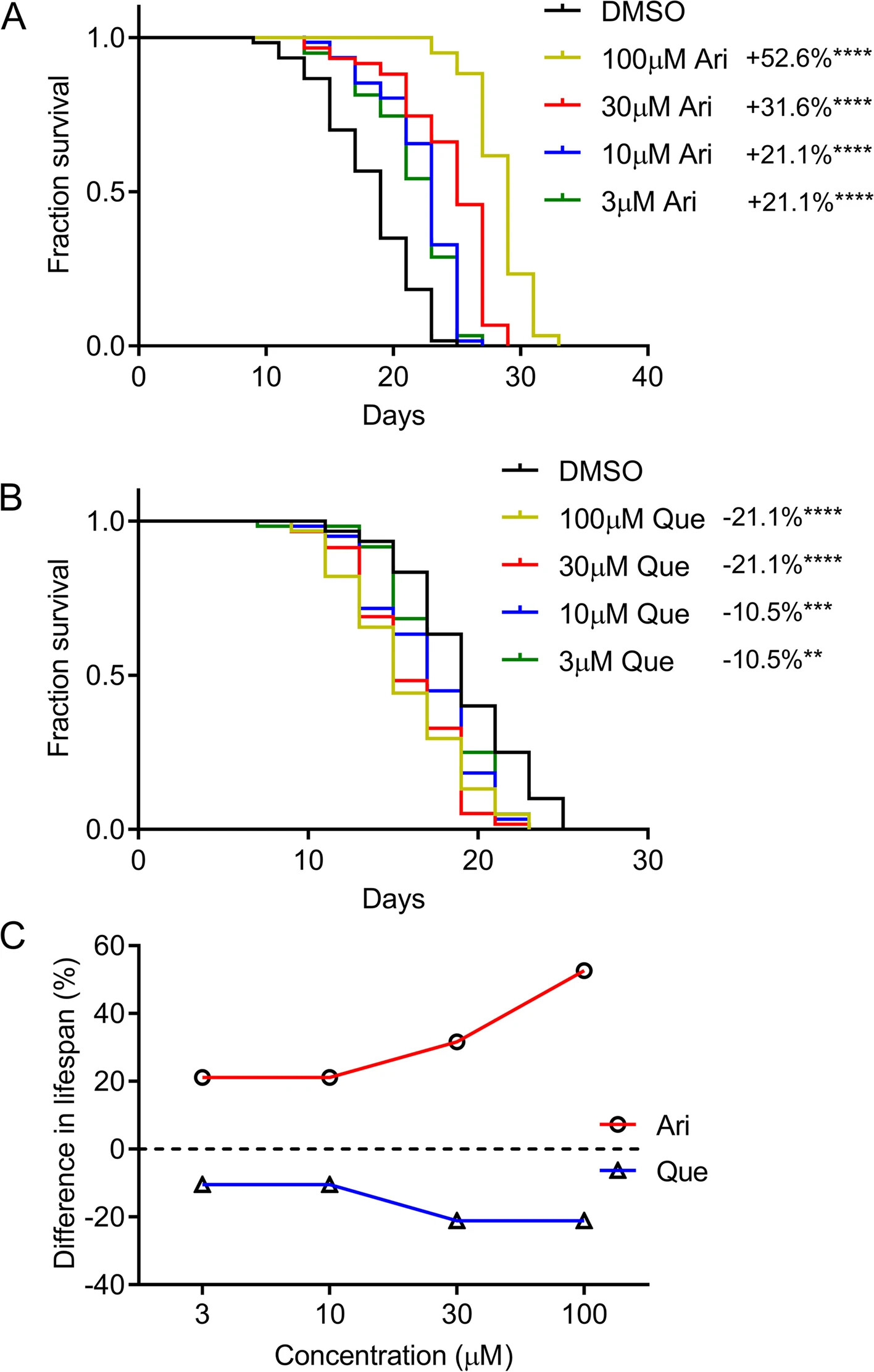
To further confirm the role of D2R in extending lifespan in C. elegans, a pharmacological approach employing aripiprazole, a D2R agonist, and quetiapine, a D2R antagonist, were used to determine the effect on worm lifespan [21, 22]. Wild-type N2 worms were treated with aripiprazole and quetiapine at concentrations ranging from 3 to 100 μM. Robust lifespan extensions were observed in aripiprazole-treated worms. Aripiprazole at 3 μM concentration significantly extended the median lifespan of N2 worms by 21.1% (P < 0.0001). Worms exposed to 100 μM of aripiprazole reached a maximum lifespan extension of up to 52.6% (P < 0.0001) (Fig. 2A). In contrast, quetiapine treatment dose-dependently shortened worm lifespan (Fig. 2B). Dose-response curves are shown in Fig. 2C. These findings further support a key role of D2R in regulating worm lifespan.
Pharmacological activation or inhibition of D2R exerts opposite effects on the lifespan of C. elegans . A Survival curves of wild-type (N2) worms cultured at 20 °C on NGM plates containing different concentrations of aripiprazole (Ari). DMSO treatment was used as a control. B Survival curves of N2 worms treated with the indicated concentrations of quetiapine (Que) or DMSO at 20 °C. (aripiprazole and quetiapine treatment were compared with the DMSO treatment: **indicated P < 0.01. ***, P < 0.001. ****, P < 0.0001, log-rank test). C Dose-response curve of aripiprazole (Ari) and quetiapine (Que) treatment. (see Additional file [2](for supporting data). Experiments were performed in three independent biological replicates
No recent high-quality studies confirm that L-deprenyl (selegiline) is useful. It’s probably better to avoid it.
So lithium is probably the best guess.
Then some “longevity” drugs seem to have mild antidepressant properties as a side effect (rapa? GLP-1RA? SGLT2i? telmisartan?) but it’s mostly based on some anecdotal evidence or association studies and it probably varies a lot from one person to another.
There’s something weird going on with BPD drugs, for sure. Lithium and olanzapine might both exert longevity effects through GSK3 inhibition, which may also be the mechanism of action (I don’t understand what causes BPD or how the drugs work; maybe no one does). Li alone did not extend mouse lifespan in the best study to date. Valproate has significant chatter about it, but doesn’t have a proper longevity study in mammals AFAIK.
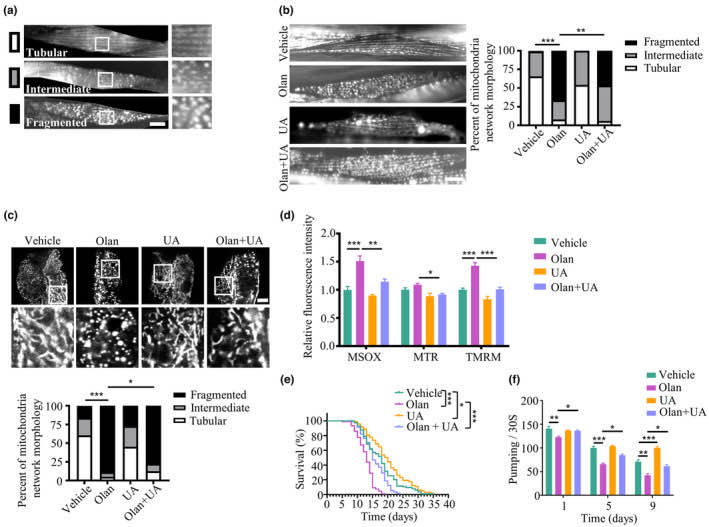
The lifespan of schizophrenia patients is significantly shorter than the general population. Olanzapine is one of the most commonly used antipsychotic drugs (APDs) for treating patients with psychosis, including schizophrenia and bipolar disorder. Despite their effectiveness in treating positive and negative symptoms, prolonged exposure to APDs may lead to accelerated aging and cognitive decline, among other side effects. Here we report that dysfunctional mitophagy is a fundamental mechanism underlying accelerated aging induced by olanzapine, using in vitro and in vivo (Caenorhabditis elegans) models. We showed that the aberrant mitophagy caused by olanzapine was via blocking mitophagosome–lysosome fusion. Furthermore, olanzapine can induce mitochondrial damage and hyperfragmentation of the mitochondrial network. The mitophagosome–lysosome fusion in olanzapine‐induced aging models can be restored by a mitophagy inducer, urolithin A, which alleviates defective mitophagy, mitochondrial damage, and fragmentation of the mitochondrial network. Moreover, the mitophagy inducer ameliorated behavioral changes induced by olanzapine, including shortened lifespan, and impaired health span, learning, and memory. These data indicate that olanzapine impairs mitophagy, leading to the shortened lifespan, impaired health span, and cognitive deficits. Furthermore, this study suggests the potential application of mitophagy inducers as therapeutic strategies to reverse APD‐induced adverse effects associated with accelerated aging.
Appreciate for the replies and information everyone! @Cohen@adssx@Lost
Cohen, so clozapine, aripiprazole (antipsychotics atypical), fluoxetine (ssri), safinamide (mao-B) has shown to be helpful for longevity.
Some of the other medicines like Olanzapine might speed up aging.
adssx, good info and link. I read your thread, and it was very good. I see what you mean now with the l-deprenyl (selegiline) in that thread.
I have not tried any of those you mentioned but would like to compare those someday (rapa, glp-1ra, sglt2I, telmisartan).
Very nice to see Ward Dean MD on this forum! He’s been talking about longevity related topics for probably over 30+ years. Here is a good audio only video with him back in 2001.
Lost, good info with the gsk3 inhibition. I have not looked into that area before. The various kinases seem very complex. As you mentioned that maybe no one understands some of these mechanisms of action mentioned at this time. Valproate does sound interesting.
AI, or some type of computer might figure this out eventually.
Thanks. This would indeed be worrisome if one intended to use olanzapine at full dosages. I in no way recommend experimenting with this drug at all – I mentioned it because it’s interesting that it has some overlap with lithium. Like with Li, if there is a pro-longevity dose one might expect it to be much smaller than the psychiatric dose.
In light of the data described in this editorial, it is probably an approximately correct conclusion that most cases of AD might be cured within six months of taking triple therapy, consisting of lithium, at a dose of 150 mg daily, fluoxetine, at a dose of 20 mg daily, and one weekly injection of dulaglutide at a dose of 1.5 mg, which, between them, address 19/21 of the causal factors in Table 1. The causal elements not addressed by the suggested combination are hypertension and inadequate levels of folate and vitamin D; regardless, if these are present in individual patients, they should be treated with appropriate antihypertensives and with folate and vitamin D.
I’m not super convinced. It’s a very bold claim. (Also: very high lithium dose, can be dangerous for kidneys?). I still think that the multiple therapy approach is interesting in general.
Quetiapine is often used off-label for insomnia at doses of 25 mg or less, while schizophrenics take 800 mg or more. I’ve been taking 12.5 mg every night for years, and it always knocks me out like a mickey finn. I know that anticholinergics like quetiapine have an increased risk for dementia, but the tradeoff for me is no insomnia, which has an even higher risk for dementia, not to mention a zombie-like quality of life.
adssx, Have you read the LifeExtension.com article titled “The Deprenyl Controversy” from August 2023? It’s a long summary with LEF giving their opinion under the title “Why We Continue To Recommend Deprenyl For Anti-Aging Purposes.” If you have any thoughts on the article please list them.
Yes I read it and I think it’s BS. I commented in other posts, but to sum it up here:
Extraordinary claims need extraordinary evidence: no one reproduced the extraordinary findings regarding selegiline. (Most recently Ora Biomedical did not find any life extension in worms.)
The Hungarian team who studied selegiline and came up with these extraordinary claims is not working on selegiline anymore. They also don’t want to submit a selegiline proposal for the ITP (I asked them).
Selegiline is already approved, we could look at medical records to see if users live longer than non users. Either no one looked at it or no one found anything.
In Parkinson’s disease selegiline is symptomatic, it’s not disease modifying. So it does not slow the disease. And probably doesn’t do anything for life extension either (we would easily see it otherwise).
I’d like to try survoexant but the copay here is $500 and my favorite suppliers in India don’t have it. I could try low-dose doxepin, which may be safer than quetiapine.
I doubt quetiapine in doses of 25 mg or less would have any significant negative effect.
Anticholinergic negative side effects are dose-dependent. 25 mg of quetiapine is a small dose compared to the doses normally prescribed, 150-300 daily to 800 mg daily.
The benefit you are reaping from getting a good night’s sleep probably offsets any possible increase in dementia because poor sleep is associated with increased dementia as well as a host of other negative health benefits.
Perhaps you could consider taking a choline supplement such as CDP choline in the morning to perhaps offset the anticholinergic effect of the quetiapine.
Choline supplements can increase the availability of acetylcholine, potentially counteracting the acetylcholine-blocking effects of anticholinergic drugs.
Some people in the nootropic community take microdoses of aripiprazole, usually less than 0.2mg daily.
Aripiprazole, a novel atypical antipsychotic drug, can significantly increase dopamine (DA) levels in the prefrontal cortex of rats, but only at low doses below 1mg/kg. The aim of the present work was to test the effect of aripiprazole (0, 0.1, 0.3, 3 and 30 mg/kg, i.p.) on extracellular levels of monoamines in the prefrontal cortex of freely moving C57BL/6J mice. Concurrent horizontal locomotor activity was also assessed. Aripiprazole produced a significant increase in dialysate DA levels after the administration of a low dose of 0.3mg/kg. Lower (0.1 mg/kg) or higher (3 and 30 mg/kg) doses failed to affect extracellular levels of DA. In addition, none of the doses tested in the present study produced significant changes in extracellular levels of noradrenaline (NA) and serotonin (5-HT). For the sake of comparison, clozapine (0, 3 and 10 mg/kg, s.c.) was also tested under similar conditions. Clozapine produced a dose-dependent increase in both dialysate DA and NA levels without affecting extracellular 5-HT. Locomotor activity was significantly decreased by both clozapine and aripiprazole. These data further support the hypothesis that selective activation of dopaminergic neurotransmission in the prefrontal cortex may contribute to the therapeutic efficacy of aripiprazole.
Rationale: Working memory impairments in schizophrenia have been attributed to dysfunction of the dorsolateral prefrontal cortex (DLPFC) which in turn may be due to low DLPFC dopamine innervation. Conventional antipsychotic drugs block DLPFC D2 receptors, and this may lead to further dysfunction and working memory impairments. Aripiprazole is a D2 receptor partial agonist hypothesised to enhance PFC dopamine functioning, possibly improving working memory.
Objectives: We probed the implications of the partial D2 receptor agonist actions of aripiprazole within the DLPFC during working memory. Investigations were carried out in healthy volunteers to eliminate confounds of illness or medication status. Aripiprazole’s prefrontal actions were compared with the D2/5-HT2A blocker risperidone to separate aripiprazole’s unique prefrontal D2 agonist actions from its serotinergic and striatal D2 actions that it shares with risperidone.
Method: A double-blind, placebo-controlled, parallel design was implemented. Participants received a single dose of either 5 mg aripiprazole, 1 mg risperidone or placebo before performing the n-back task whilst undergoing fMRI scanning.
Results: Compared with placebo, the aripiprazole group demonstrated enhanced DLPFC activation associated with a trend for improved discriminability (d’) and speeded reaction times. In contrast to aripiprazole’s neural effects, the risperidone group demonstrated a trend for reduced DLPFC recruitment. Unexpectedly, the risperidone group demonstrated similar effects to aripiprazole on d’ and additionally had reduced errors of commission compared with placebo.
Conclusion: Aripiprazole has unique DLPFC actions attributed to its prefrontal D2 agonist action. Risperidone’s serotinergic action that results in prefrontal dopamine release may have protected against any impairing effects of its prefrontal D2 blockade.