Looks like there’s no general discussion on this, so I’m starting this one. But if I missed an existing topic, please merge this post there.
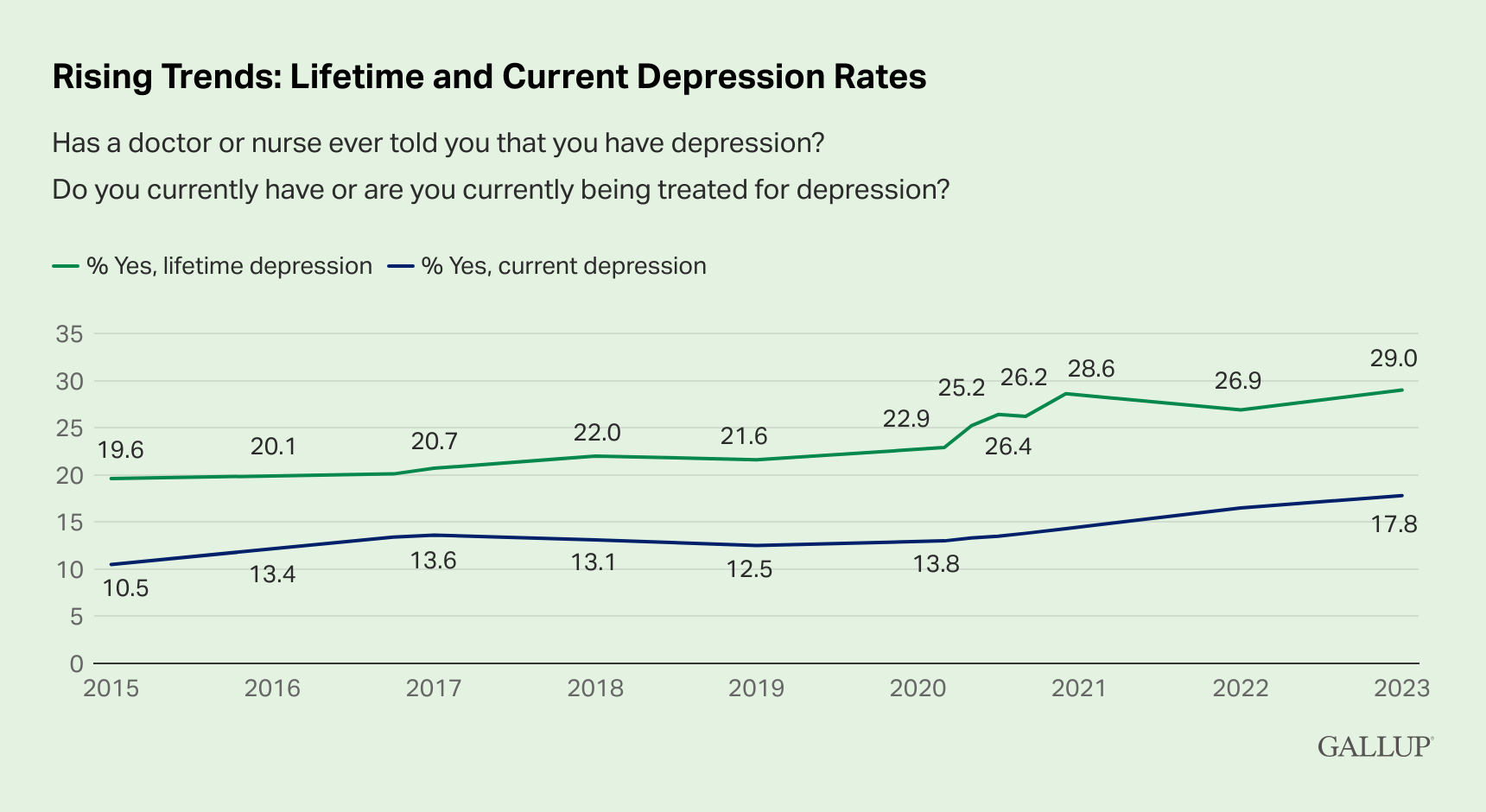
Depression seems to accelerate biological aging (see: Depression’s Unexpected Role in Accelerating Biological Aging ). In the US, 17.8% of adults are currently treated for depression:
Depression is also a risk factor or even a prodromal symptom of many neurodegenerative diseases (NDDs) such as Alzheimer’s and Parkinson’s. It can start years or decades before the actual NDD diagnosis. As we improve prevention, early diagnosis, and treatment of cardiovascular diseases and cancer, NDDs are becoming the first cause of death in high-income countries.
Unfortunately, it looks like there’s no excellent treatment to date. Indeed, antidepressants seem, at best, a bit better than placebo (see: Antidepressant - Wikipedia). They’re also associated with significant withdrawal symptoms (see Antidepressant discontinuation syndrome - Wikipedia) that make me weary of just trying them. And some longitudinal studies also point to long-term risks:
- Antidepressant use and risk of adverse outcomes: population-based cohort study 2022
- Association between Antidepressants and Dementia Risk in Older Adults with Depression: A Systematic Review and Meta-Analysis 2023
(Although others show no risk, but no benefit either: Antidepressant use in relation to long-term dementia risk and imaging markers of neurodegeneration: a population-based study of potential adverse effects 2022)
As I have a family history of MDD and a personal history of low-mood episodes, I’d love to find ways to reduce my long-term risk of depression and associated complications (especially neurological damage), besides diet, sleep, exercise, meditation/stress management, and socializing, that are, of course, essential but, at least for me, not enough.
My reasoning is to look at “longevity interventions” (such as successful compounds in the ITP) and then, among them, look at those with antidepressive (and anti-anxiolytic) properties. I assume that they’re safe(r) for long-term use (on other markers of health than mental health) and that if they improve my mood they can be a reasonable long-term option. So far, I’ve found that:
- SGLT2 inhibitors seem associated with lower risks of depression: “patients with diabetes using SGLT2 had even lower odds of depression compared to individuals without diabete” (Diabetes, antidiabetic medications and risk of depression – A population-based cohort and nested case-control study 2022). There are two ongoing clinical trials of dapagliflozin and empagliflozin for depression. (And anecdotally, after one month of dapagliflozin 5 mg, that I’m taking for reactive hypoglycemia, my mood seems better…)
- Rapamycin + ketamine may be more effective than ketamine alone for major depressive disorder (MDD). And Kaeberlein’s survey points to many users feeling happier: an interesting but weak signal.
- GLP1 agonists and creatine seem promising and there are ongoing clinical trials.
- Low-dose selegiline may be worth exploring as well.
Besides the above, I could not find anything. Either there are just a few weak papers on rodent models (but are animal models of depression good?) or small phase 1 or 2 trials on humans without strong conclusions. In any case, we rarely know the long-term effects of taking these drugs or supplements on general health (whereas we know that, for instance, long-term use of SGLT2 inhibitors is safe and even beneficial for some conditions such as CVD).
And then there’s ecstasy/MDMA (which will soon be FDA-approved for PTSD), psilocybin (approved in Australia and some Canadian provinces for depression) and other psychedelics. They’re interesting because they seem effective after just a couple of sessions, without withdrawal symptoms, compared to long-term use for traditional antidepressants, with a significant risk of discontinuation syndrome. But there are methodological weaknesses in psychedelic trials (the most important being the absence of a real blinded placebo: patients know for sure that they had the drug) and their safety profile is not yet fully known. They also seem to work as part of a “psychedelic-assisted therapy”. So I would not try them alone but I would prefer to do it under the guidance of an experienced therapist. And unfortunately, they’re not yet approved where I live (the UK, although ketamine is approved here). I could travel to places where it is approved (or just tolerated, like Portugal) but I would prefer something local.
What do you think? What do folks here use or have tried? What’s the state of the research on this topic? Are there other promising interventions?