Focus on Aging Research The speaker emphasizes that aging research is more effective than focusing on individual diseases like cancer or Alzheimer’s for extending healthy lifespan. He highlights that curing cancer completely would only increase a woman’s life by about 2.6 years, whereas anti-aging interventions in mice have shown significantly greater increases.
New Concepts in Aging Research
Aging can be slowed: Contrary to popular belief, aging can be slowed in mammals through diet, single-gene mutations, and drugs.
Lifespan and Healthspan are linked: Interventions that extend lifespan also extend healthspan by slowing the loss of health, dispelling the idea of a trade-off.
Molecular clues: Studies have provided new molecular insights, pointing to factors like IGF-1, uncoupling proteins in mitochondria, and changes in glucose metabolism as targets for anti-aging drugs.
Focus on aging rate: Instead of asking what causes aging, the more important question is what slows the rate of aging, as the causes of aging are highly heterogeneous across different body parts.
Interventions Testing Program (ITP)
Methodology: The ITP uses genetically heterogeneous mice, allowing for suggestions from the scientific community, and testing drugs at three different labs. They use a large number of mice to detect small changes in lifespan.
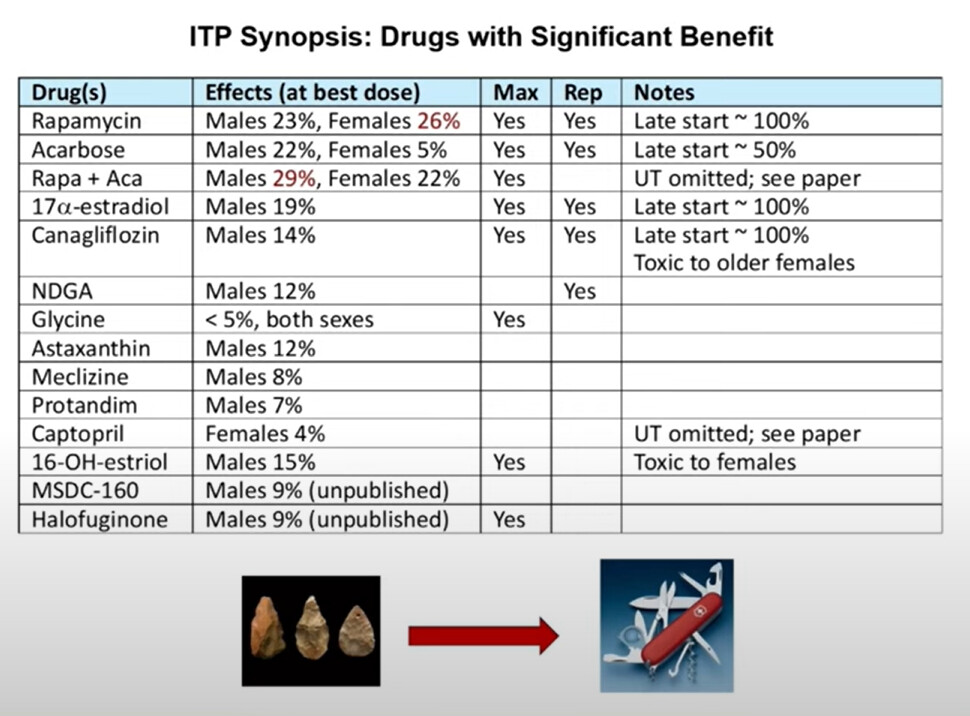
Results: While 85% of suggested drugs do not work, 12 drugs have shown positive effects. Rapamycin is the most famous, increasing male lifespan by 23% and female lifespan by 26% at the highest doses.
Middle-Aged Intervention: A significant finding is that rapamycin and several other drugs are effective even when started in middle-aged mice, rather than only in youth.
Broad Impact: Rapamycin slows the aging process itself, not just specific diseases, delaying various age-dependent tissue changes and cancers.
Other successful drugs: Acarbose, canagliflozin, 17-alpha estradiol, and others have also shown positive effects. Metformin, while a “terrific diabetic drug,” did not extend mouse lifespan in ITP studies.
Over-the-counter options: Meclizine and astaxanthin are available without prescription and have shown benefits in mice, though human efficacy is unknown.
Sex-specificity: Many drugs exhibit sex-specific effects in mice, working in males, females, or both.
Aging Rate Indicators (ARIs)
Concept: ARIs are like a “speedometer for how rapidly you are aging,” distinct from biomarkers of aging which are like an odometer. They detect changes in the rate of aging quickly after an anti-aging intervention.
Shared mechanisms: The goal is to identify common pathways and changes induced in young adults by various slow-aging interventions (genes, diets, drugs).
Examples of ARIs:
GPLD1 protein: Elevated in slow-aging mice and those treated with anti-aging drugs and caloric restriction. This protein is translated via cap-independent translation, not changes in mRNA levels.
Brain health indicators: BDNF and doublecortin levels increase in the brain of slow-aging and drug-treated mice.
Fat biology: Increased uncoupling protein 1 (UCP1) and conversion of white fat to brown/beige fat in most slow-aging mice (with rapamycin being an exception).
Inflammation: Reduced pro-inflammatory macrophages (M1) and increased anti-inflammatory macrophages (M2) in the fat of slow-aging mice.
FNDC5/Irisin: Elevated in the muscle tissue of slow-aging mice, linking muscle to fat changes.
Implications: ARIs are detectable in various tissues, influenced by diverse genetic mutations and anti-aging interventions. They are not cell-autonomous and often involve communication between different cell types, making them difficult to discover in tissue culture models.
Future Directions
Identify upstream mechanisms producing these shared cellular and molecular changes.
Understand how these changes delay age-associated diseases.
Determine how quickly drugs can switch these indicators (e.g., within months) to accelerate drug screening.
Investigate if ARIs can be influenced in people and if they are under genetic control.
Call to Action: The ITP invites scientists to suggest new drugs for testing and offers access to their drugs and tissues for research collaborations.
Vision of Aging: The ultimate goal is to produce a “new kind of old person” – healthy and active at advanced ages, exemplified by a hypothetical 114-year-old with the vitality of a typical 70-year-old today.
Q&A Highlights:
Human Data: The speaker discusses the need for large-scale, placebo-controlled clinical trials for human data, but also points to potential insights from existing human exposure databases (e.g., people taking SGLT2 inhibitors like canagliflozin for pre-diabetes).
Common Pathway: The presenter believes that the similar benefits across different interventions (rapamycin, caloric restriction, etc.) suggest a common upstream pathway that influences various tissues.
Statistical Analysis: Acknowledges alternative statistical approaches (like Jim Nelson’s work) that offer more nuanced insights into lifespan curves, showing that some drugs might affect mortality risk at specific ages even if not overall median/maximum lifespan. He encourages researchers to use the publicly available ITP data for their own statistical analyses.
It looks like we have 2 new potential anti-aging drugs here - MSDC-160 and Halofuginone. Is either practical for humans to take? Any notable side effects? Halofuginone is an anti-parasitic used for animals (this reminds me of Ivermectin).
It seems that this year’s crop of ITP results is a disappointment. Nothing notable that moves the needle.
Given the paucity of new LE drug candidates, if the ITP had more funding I’d love to see if they could do more with the drugs that already did show effects. One way to do that would be to have a separate program that took all the drugs that showed effects and focused on running trials with various combinations of these drugs - they’ve already done some like rapa + acarbose, but if this was a separate program then the main ITP could focus on testing new drugs, while the combo-ITP would keep working so there’s always something cooking and we don’t have the feeling of stagnation. Alas, it looks like there won’t be extra money anytime soon.
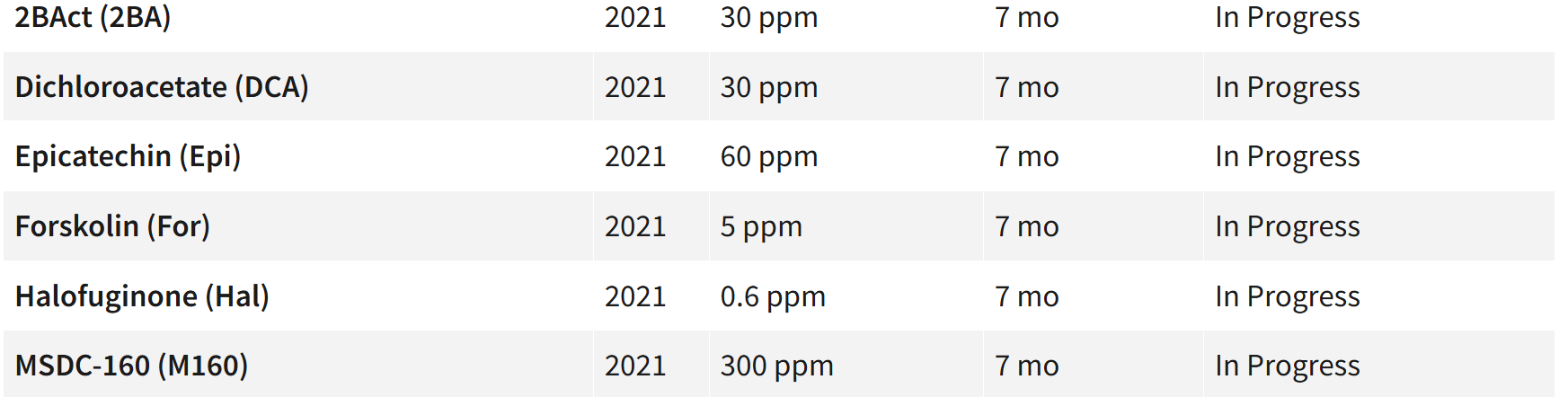
Does this mean the other substances tested by the ITP that started the same year (2021): 2BAct, Dichloroacetate, epicatechin, and Forskolin all failed? You’d think they’d be mentioned if they had any success at all.
Thanks for sharing. I greatly respect Rich Miller and the unbiased work he does. Really, the ITP deserves 5x more funding. They need to test drug combinations - especially where they likely have different mechanisms. Imagine Astaxanthin and Acarbose together.
The ageing rate indication stuff is brilliant, and I can see that being more useful than the “clocks” for tracking various interventions.
I did start taking Astaxanthin, based entirely on the ITP result. I felt there’s very little harm, and there’s some decent evidence out there that it’s useful.
I am very curious about the Meclizine result, and I can’t imagine what the mechanism would be.
The acarbose and canagliflozin results really tell us that blood glucose control is super important. I can only imagine that GLP1RAs will do well in the ITP once they test them.
Holy mackerel — they’re still using the wrong terminology. They do correctly list the first estrogen derivative that Brian Johnson experimented with — 17α-estradiol. That’s basically just estradiol with the 17-position hydroxy flipped from the β- to the α-orientation, a small stereochemical tweak that alters metabolism and leads to estriol-like downstream products.
But for the new compound, they slip back into the wrong name. What they call “16-OH estriol” is nothing more than my dear friend estriol (E3) herself. If you wanted to be precise, you could say estriol is a “modified estradiol” — in other words, estradiol with an additional hydroxy group at the 16 position. That makes it formally 16-α-hydroxy-estradiol, which is a syntactically correct chemical name but also a source of endless confusion with plain old but still beautiful E3.
To back this up, here’s the official correction they had to issue last time:
“There are five places in the paper where a drug is mistakenly referred to as ‘16-hydroxyestriol.’ The correct name of this drug is ‘16-hydroxyestradiol.’”
It would be messy and likely not feasible but every time I read ITP-related articles, I envision a metanalysis that aggregates the ITP findings and determines how much variance they account for in human healthspan mid-points. It is an open empirical question but I think the findings would not support the kind of conversations that I see so many of in which the term ‘mice’ is tacitly replaced with human interests. ITP is a worthwhile venture and I admire the methodological discipline of the program but its value lies primarily in establishing early directions for human investigations.
Maybe I’m missing something but why were they testing these instead of more commercially available supplements/drugs that more people are actually using?
If I just go by these there’s very few if any interventions worth a woman’s consideration. @RapAdmin posted another article in a different thread about the sex asymmetry effect of most of these (the benefits skewing heavily male, aside from Rapa and one or two more, barely worth mentioning due to small effect size). I’d love to see replication of, say canagliflozin or Astaxanthin, in different mammal species to see if the sex asymmetry is only specific to mice. Something tells me it might not be.
Rich Miller has talked about this on podcasts before.
Basically, people need to submit a proposal, which needs to include at least some plausible evidence, a potential mechanism etc. Like, this molecule has extended life of C.elegans, binds this protein also found in mice etc.
Then there are funding limitations. They can only take a certain number of molecules per year.
Then there are practical limitations. The molecule needs to be orally available, and needs to be integrated with the mouse food pellets. They can’t do injectable, since they have hundreds of mice (it’s why GLP1RAs haven’t been tested yet). They’ve had serious issues in the past with things having no solubility and no absorption. The first Rapamycin trial almost got cancelled because it has terrible bioavailability and they had to find a way to encapsulate it, and make sure it’s actually getting into the mouse blood stream, which took ages.
Plus, I think there is a bit of personal opinion from the three ITP managers, perhaps based on their interested. Rich Miller said they wanted to test resveratrol because there was so much hype about it. Same with Fisetin (which completely failed, and didn’t even show activity).
That’s disappointing about epicatechin, because there are results like this:
…
I wonder how much results like ITP’s just boil down to them having more money and resources (enabling them to use more mice and longer-lived varieties), as opposed to having more talent. The point being that perhaps a lot of people could run good studies if they had 10x the funding and weren’t under as much pressure to publish results quickly.
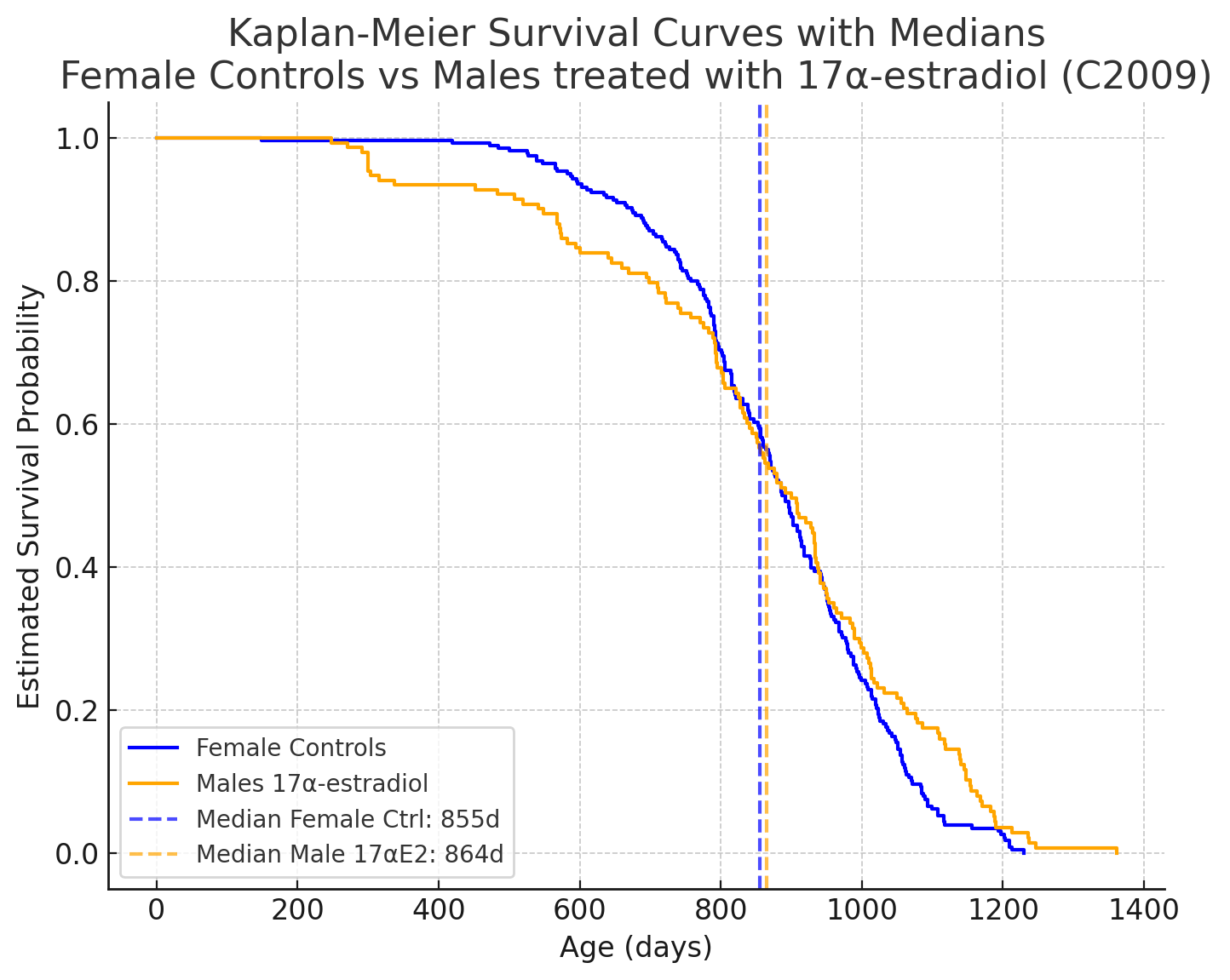
I conducted a comparison in ChatGPT of the best intervention in males against the female control group. There is no significant difference, which suggests that interventions that increase lifespan in males may only provide a compensatory effect rather than actually delaying aging. In contrast, interventions that act in both sexes do appear to have a genuine effect on longevity.
Is it me or do these percentages keep changing? I thought Captopril only extended lifespan slightly in males but this chart says females. I also thought glycine had a 6% benefit, not less than 5%.
Does anyone know what exactly is meant by canagliflozin being toxic to older females by chance? Specifically how older is defined and in what way it is toxic? Extra credit: would this apply to all flozins?
I think they are two different research questions.
That epicatechin study used B6 mice, and had 33 mice per group.
B6 mice are very commonly used, but they are very weird overall and not really representative of a “mouse”. Plus they are essentially genetically identical to each other. SO people will say that the n = 33 is more like n = 1 sample with 33 replicates. And, they’re all from one supplier, housed in one lab etc.
The ITP has a minimum of 150 mice per group, and usually has ~300 mice in the control groups. And, the mice are split between 3 institutions in 3 states. So if a molecule extends lifespan in all 3 sites, that’s very strong evidence. (Funnily enough, Rich Miller has reported that even the control groups sometimes show differences in survival between sites, and they have no idea why). They also use mice that are much more genetically heterogeneous, so the n = 300 really is n = 300.
So basically, the ITP is more powerful in every way - not just because of funding, but because of the design and all the time they’ve invested into getting the model working, standardising protocols etc.