This class of drugs seems to be flying under the radar, despite quite a bit of evidence pointing towards longevity benefits. I’ve seen a handful of people on this site report taking them, but I wanted to make a thread and invite anyone else using them to report their dosing protocols and subjective experiences (whether good or bad), and hopefully spur some further discussion.
I guess to start, here’s a good review on why ARBs may be pro-longevity drugs. In particular, they appear to protect the heart, kidneys, and blood vessels, although concerns may arise about their effects on blood levels of sodium and potassium.
The ITP is currently testing the ARB telmisartan, although in combination with atorvastatin. I find this a little odd considering they’ve tested neither drug in isolation, but at least a positive result would provide further support for telmisartan.
A related class of drugs, the ACE inhibitors, have already seen two examples (captopril and enalapril) tested in the ITP. Enalapril was without effect, while captopril was effective in females but the result was inconclusive in males. This inconclusive result was due to low survival of control mice at one of the three test sites. Excluding that site from the analysis, captopril increased 90th percentile female lifespan by ~7%.
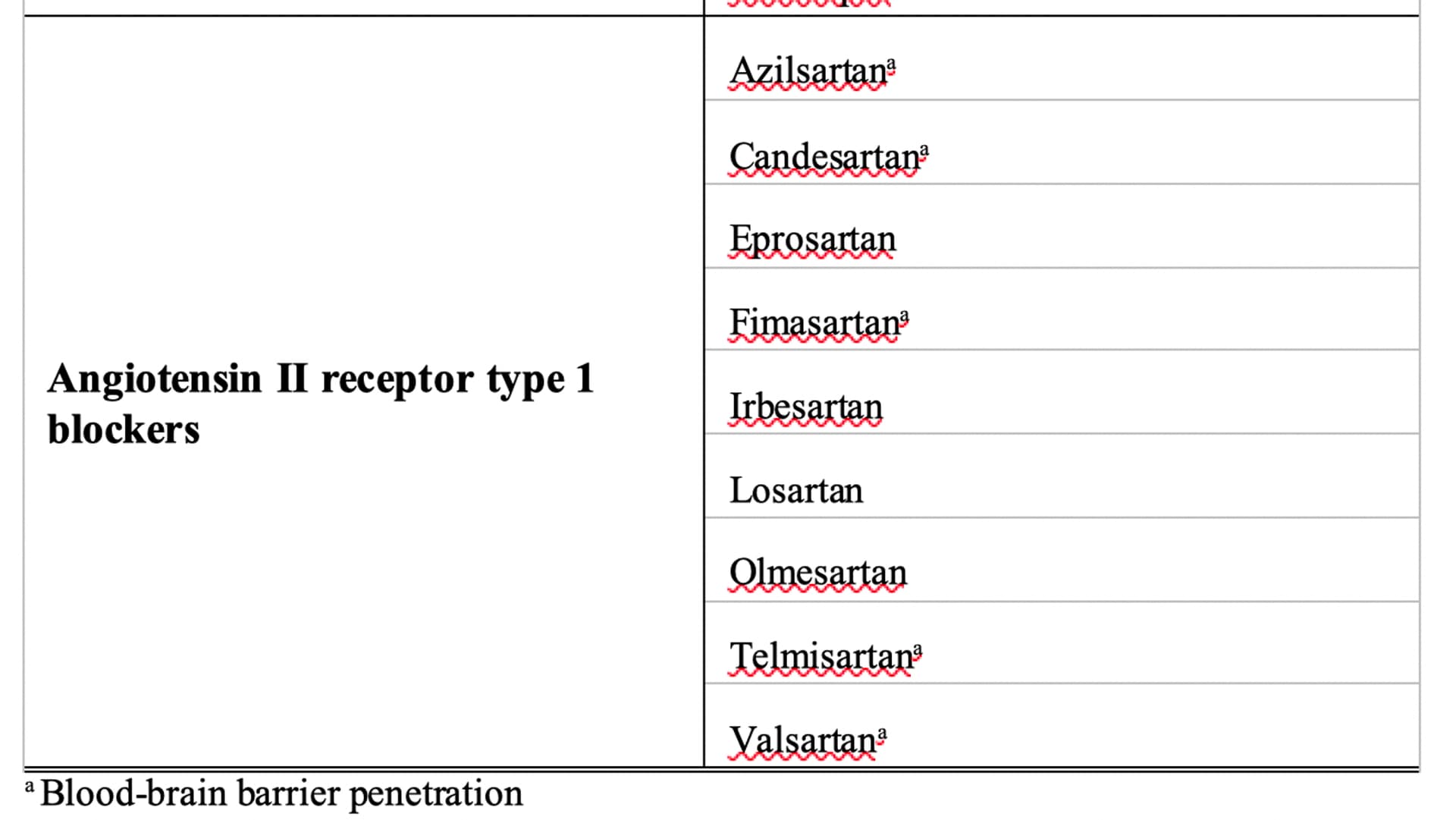
As far as the pharmacology of angiotensin II receptors goes, you need to know that there is both angiotensin II receptor type 1 (AT1) and angiotensin II receptor type 2 (AT2). Additionally, mice have two isoforms (AT1A and AT1B) of angiotensin II receptor type 1 while humans have only one, but it’s their AT1A which is considered equivalent to our single copy of AT1 (yes, the nomenclature is very confusing).
AT1 tends to exert anti-longevity effects while AT2 tends to oppose those effects. For this reason, ARBs may foster greater longevity than ACE inhibitors. This is because ARBs are quite selective for AT1, whereas ACE inhibitors will inhibit both AT1 and AT2.
One study found that knocking out AT1A in mice increased average lifespan by 26% while protecting against cardiac hypertrophy, cardiac fibrosis, and deterioration of aorta histology. Additionally it reduced oxidative stress in heart, kidney, and aorta, and prevented mitochondrial loss in kidney.
Whereas the ITP studies only found conclusive evidence for lifespan extension via renin-angiotensin system inhibition in females, this study provides evidence that males may also benefit. OTOH, the glaring issues with this study are the small number of mice in each group, as well as the short lifespan of controls (~755 days average lifespan).
One further study supports that AT1 is anti-longevity, and it showed this by knocking out ATRAP, which negatively regulates AT1. The median lifespan of mice lacking ATRAP was 18.4% shorter than controls, and they displayed a deterioration of kidney function despite lacking obvious changes in blood pressure or cardiovascular phenotype.
I’m considering trying telmisartan from India, and it would be nice to hear anyone else’s experience with it, or any concerns that others may have. I guess it would be smart to monitor sodium and potassium levels while on it, although I imagine healthy people would have fewer issues in this regard compared to people taking it for clinical manifestations.
One last thing, for those who believe that DNA damage (oxidative or otherwise) is a fundamental driver of aging, it’s interesting to consider that AT1 is expressed on nuclear membranes and stimulates intranuclear ROS production. As mice are generally less su
Two polymorphisms in AGTR1 promoter, rs422858 and rs275653, in complete linkage disequilibrium, were significantly associated with the ability to attain extreme old age. We then replicated the study of rs275653 in a large independent cohort of Japanese origin (598 centenarians and semi-supercentenarians, 422 younger controls) and indeed confirmed its association with exceptional old age. In combined analyses, rs275653 was associated to extreme longevity either at recessive model (P = 0.007, odds ratio (OR) 3.57) or at genotype level (P = 0.015). Significance was maintained after correcting for confounding factors. Fluorescence activated cell sorting analysis revealed that subjects homozygous for the minor allele of rs275653 had less AT1R-positive peripheral blood polymorphonuclear cells. Moreover, rs275653 was associated to lower blood pressure in centenarians.