Thanks a lot for sharing your protocol @Tomnook.
Yes, my conclusion so far is that the best strategy to achieve the desired target is: Telmisartan 20 mg => T 40 mg => T 40 mg + Amlodipine 2.5 mg => T 40 mg + A 5 mg => T 40 mg + A 5 mg + Hydrochlorothiazide (HCTZ) 12.5 mg
It might be better to start with the low-dose combination, but it’s not available. One manufacturer is actually developing something similar (with the thiazide-like indapamide instead of HCTZ, not sure it’s better though): Rationale for a New Low-Dose Triple Single Pill Combination for the Treatment of Hypertension 2024
In both trials, these ‘hypertension polypills’ were superior to usual care, achieving >80% BP control without increasing withdrawal due to side effects. However, there are no such products available for prescribers. To address this unmet need, George Medicines developed GMRx2 with telmisartan/amlodipine/indapamide in three strengths (mg): 10/1.25/0.625, 20/2.5/1.25; 40/5/2.5.
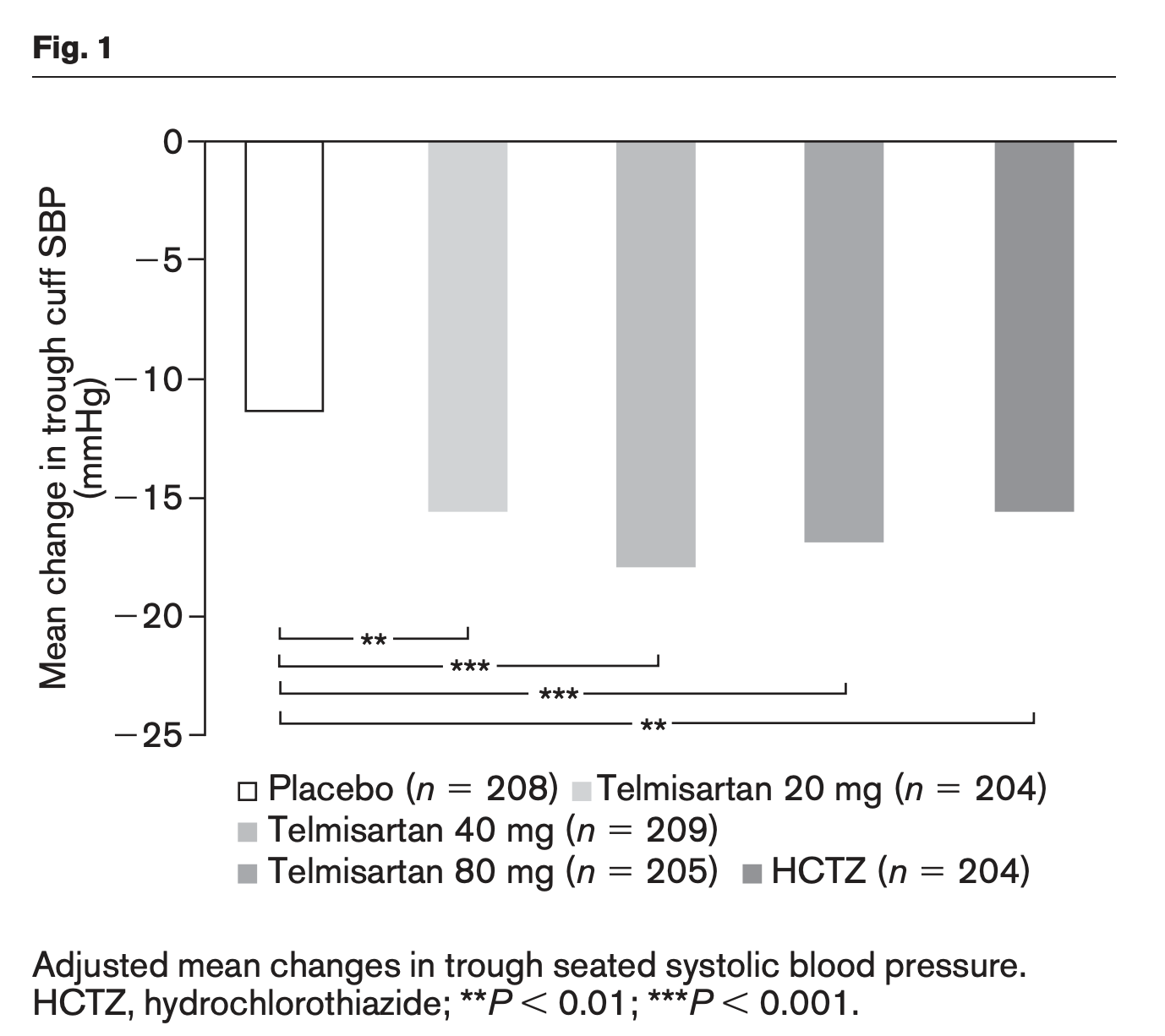
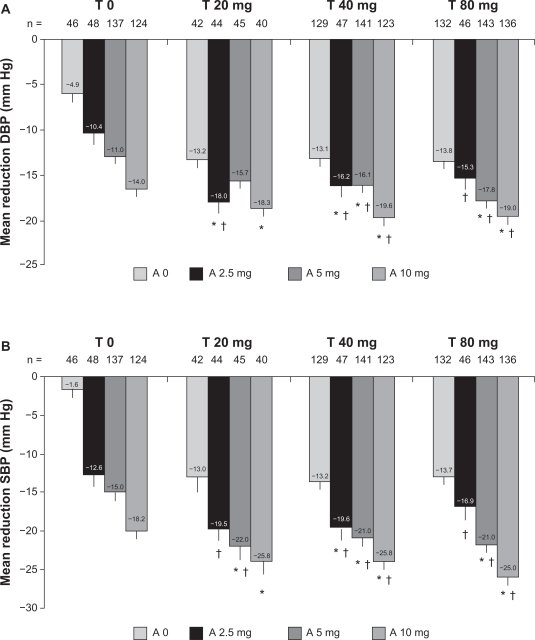
The systolic BP (SBP)-lowering efficacy of GMRx2 strengths 1, 2 and 3 (Table 2) from a baseline SBP of 150 mmHg are expected to be approximately 13 mmHg, 18 mmHg and 25 mmHg, respectively. This represents a much greater and clinically important BP reduction in comparison to standard-dose monotherapy, which reduces SBP compared with placebo by only 8–9 mmHg on average, with each doubling of dose conferring only a 1–2 mmHg incremental SBP reduction
They completed the trials. I can’t wait to see the results.
[Update: actually, indapamide might be better than HCTZ as it has a longer half-life and might cause less insulin resistance. Telmisartan is the longest-acting ARB and amlodipine is the longest-acting CCB and long-acting drugs are preferred to reduce BPV per this source. So Telmisartan/Amlodipine/Indapamide might be the best combo out there.]
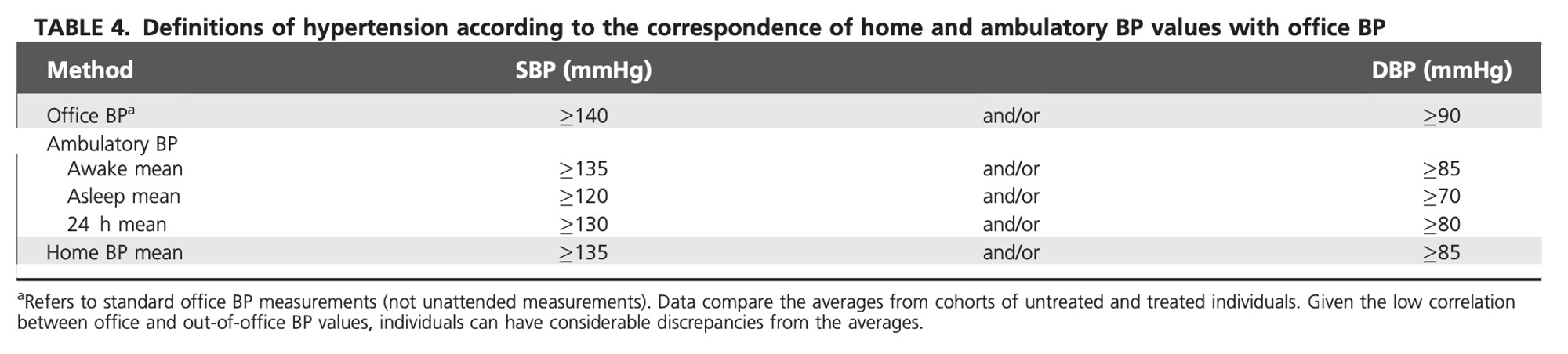
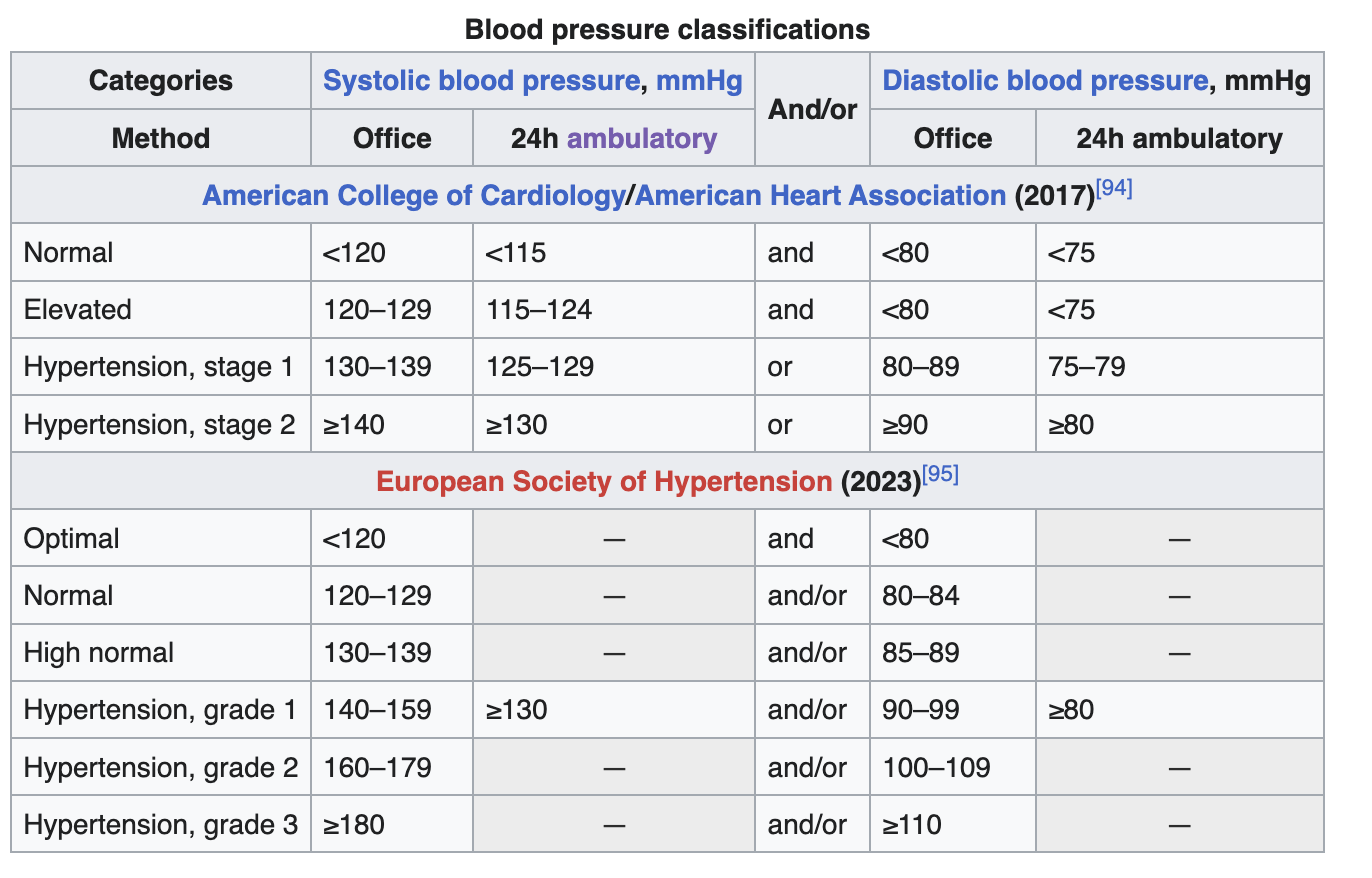
I agree that 115/75 mm Hg should be the ideal BP (if not lower). Unfortunately, the 2023 European guidelines still give 130/80 as the 24h ABPM threshold for hypertension while the American guidelines have been lowered to 125/80 since 2017:
I did a 24-hour ABPM in 2015 in France (130/69) and in 2022 in the UK (132/73), and in both cases the cardiologists concluded that I was “normotensive”. (To their defense, “Isolated systolic hypertension of the young” [ISHY] is apparently common and not associated with an increased risk for non-smoking and physically active tall men.) I tried to argue a bit (it seemed stupid to me to have an arbitrary threshold set in stone versus seeing things as a continuum) but I didn’t know much back then (and I had other things to focus on…).