Gerontological research has traditionally treated sleep deterioration as a passive consequence of growing old. However, emerging macro-epidemiological and mechanistic data flip this script, revealing that age-related sleep fragmentation and circadian dampening act as primary, aggressive accelerants of biological aging. As the human brain ages, the master circadian pacemaker—the suprachiasmatic nucleus (SCN)—undergoes structural and functional decay. This neurological decline dampens the amplitude of core body temperature rhythms and blunts nighttime melatonin peaks, forcing a progressive phase-advance that drives older adults toward early evening sleepiness and fragmented, low-efficiency nocturnal sleep.
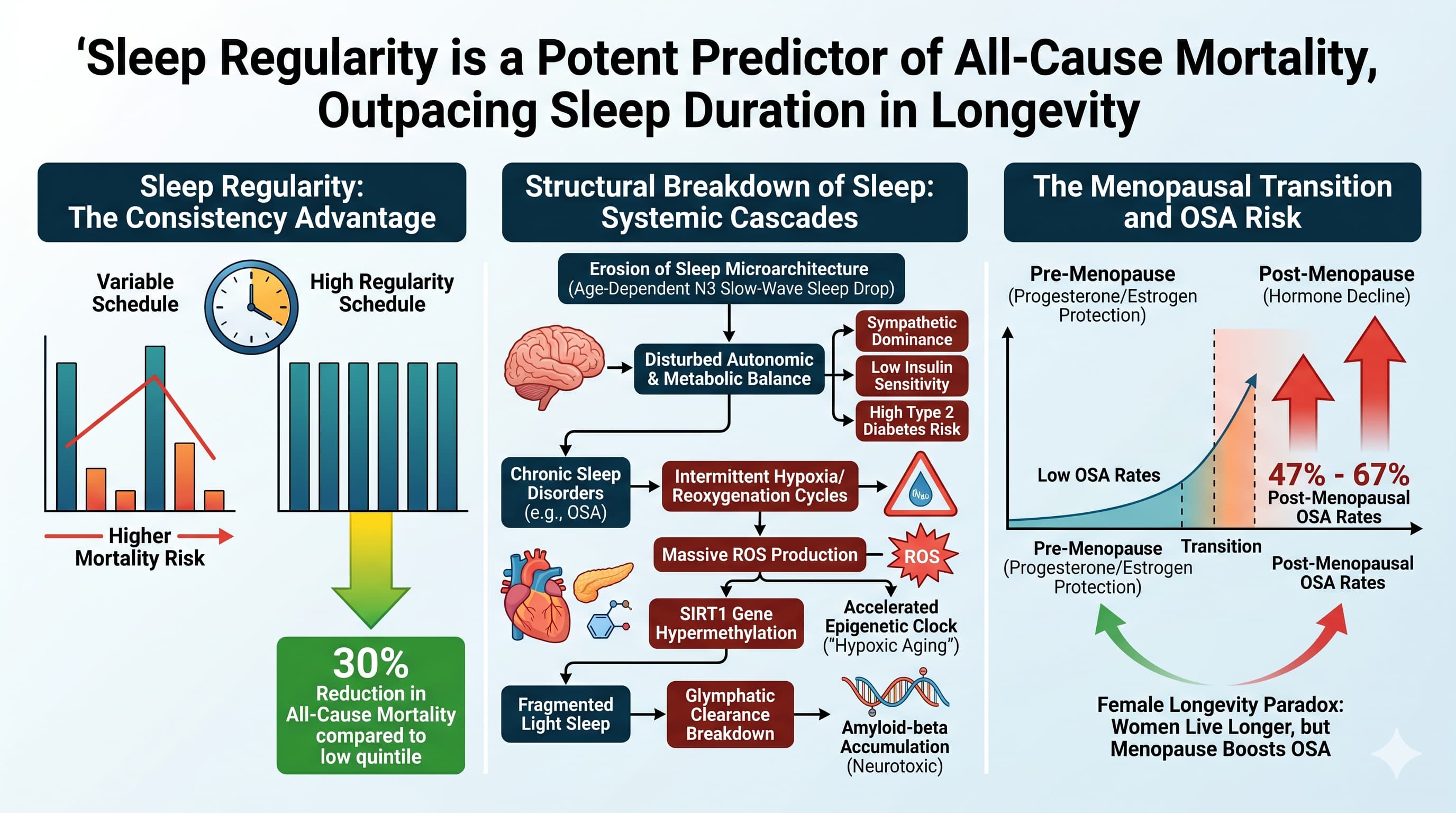
The truly paradigm-shifting insight from recent large-scale cohort analyses is that sleep regularity—maintaining a highly consistent day-to-day sleep-wake schedule—is a significantly more potent predictor of all-cause mortality than total sleep duration. Individuals tracking in the highest quintile of sleep regularity exhibit a clean 30% reduction in all-cause mortality compared to those with highly variable routines. Conversely, structural erosion of sleep microarchitecture delivers severe systemic blows. The sharp, age-dependent drop in slow-wave sleep (N3) directly disrupts autonomic and metabolic balance, inducing a shift toward sympathetic dominance, reducing insulin sensitivity, and elevating the risk of type 2 diabetes.
Simultaneously, chronic sleep disorders introduce devastating pathophysiological cascades. Obstructive sleep apnea (OSA) triggers repetitive cycles of intermittent hypoxia and reoxygenation, generating massive waves of reactive oxygen species that hypermethylate the SIRT1 gene, effectively accelerating the epigenetic clock. This “hypoxic aging” is compounded by a profound breakdown in glymphatic clearance during fragmented light sleep, allowing neurotoxic aggregates like amyloid-beta to accumulate. Crucially, the data exposes a stark female longevity paradox: while women live longer, the menopausal transition strips away the upper-airway protective benefits of progesterone and estrogen, causing post-menopausal OSA rates to skyrocket to between 47% and 67%. Ultimately, sleep can no longer be viewed as a luxury; it is a highly malleable, structural column of healthspan execution.
Actionable Insights
-
Enforce Strict Sleep-Wake Timing: Prioritize the Sleep Regularity Index by going to bed and waking up at identical times every single day. This behavioral anchor stabilizes circadian phase alignment and lowers all-cause mortality risk by 30%, completely independent of total sleep duration.
-
Aggressively Cool the Sleep Environment: Keep bedroom ambient temperatures strictly at or below 22 degrees Celsius (71.6 degrees Fahrenheit). Total sleep time remains stable up to this threshold but drops precipitously above it, causing an absolute loss of 60 minutes of sleep as ambient temperatures climb to 30 degrees Celsius.
-
Widen the Evening Fasting Window: Complete your final meal at least 6 hours before your calculated sleep midpoint. Every hour delayed significantly inflates the odds of short sleep by 30%, sleep latency by 14%, and chronic insomnia by 11%.
-
Eliminate Artificial Light and Noise at Night: Achieve absolute black-out conditions and mitigate ambient sound pollution. Nighttime light exposure directly suppresses melatonin amplitude, while even minor localized ambient noise increases the odds of severe sleep disturbance up to nearly three-fold.
-
Screen for Obstructive Sleep Apnea and Deploy CBT-I: Bypass high-risk sedatives and Z-drugs, which relax airway muscles and compound fall risks. Treat chronic insomnia via Cognitive Behavioral Therapy for Insomnia (CBT-I) to safely boost slow-wave power, and aggressively manage any underlying hypoxic burden with Continuous Positive Airway Pressure (CPAP) therapy.
Source:
-
Paywalled Paper: Sleep health in the older adults: Architecture, circadian changes, and
common sleep disorders
-
Affiliated Institutions: University Sleep Disorders Center, Department of Medicine, College of Medicine, King Saud University, Riyadh, Saudi Arabia; Government Hospitals, Manama, Bahrain; Department of Psychiatry, College of Medicine and Health Sciences, Arabian Gulf University, Manama, Bahrain; etc.
-
Journal Name: Ageing Research Reviews.
-
Impact Evaluation: The impact score of this journal is 13.1, evaluated against a typical high-end range of 0–60+ for top general science, therefore this is a High impact journal.
1 Like
Thanks for the read and the Actionable Insights. While I try to follow most of those, my struggle is needing to urinate usually at least 2X a night (sometimes more). I can usually fall asleep right after going, but my sleep is still being disrupted. Not sure what long-term effect this may be having on healthspan.
1 Like
I remember seeing this article in The NY Times:
Is Waking Up to Pee Normal?
Experts weigh in on what the urge means, and what you can do to curb it.
What can I do to reduce nocturia?
While the effects of aging aren’t reversible, there are simple lifestyle changes you can make.
Improving your sleep hygiene, for example, can help limit the number of times you wake up at night. One key step is staying clear of tea, coffee and alcohol in the evenings, since they not only disrupt sleep but also cause your body to produce more urine, Dr. Huang said.
More generally, be mindful of what you eat and drink before bed. A good rule of thumb is to avoid water and other fluids two to four hours before bed, although it’s fine to take a few sips with medication or if you’re thirsty.
Some fruits and vegetables, like asparagus, celery, watermelon and grapes, have high water content and are also known to make people urinate more. And decreasing your daily sodium intake can also help, since salt causes fluid retention.
If your ankles and legs are swollen, you could also wear compression stockings to prevent fluid from building up, Dr. Markland said; keeping them elevated can also help.
For people with overactive bladders, she suggests pelvic floor exercises to strengthen this muscle, helping control unwanted bladder contractions.
A doctor might be able to treat any underlying medical condition or review any prescription drugs you’re taking. There are even medications that can help regulate bladder and kidney function, Dr. Huang said, although they don’t work for all patients, and some can cause serious side effects.
Often, it takes a combination of small changes to discover what works for you. “Nocturia doesn’t lend itself to a single magic bullet,” Dr. Huang said.
Full article: https://archive.ph/TRUJP#selection-863.0-929.151
1 Like
The Wake-Up Call: Sleep Fragmentation, Not Just Duration, Drives Cognitive Aging
A premier study has exposed a critical flaw in how we evaluate sleep and its relationship to brain decay. For decades, the public health narrative has focused almost exclusively on sleep duration—the classic “eight hours a night” paradigm. However, new data reveals that sleep fragmentation, specifically an objective metric known as Wake After Sleep Onset (WASO), serves as a far more sinister predictor of multi-domain cognitive decline in older adults.
The research utilized baseline data from the Investigating Gains in Neurocognition in an Intervention Trial of Exercise (IGNITE) study, tracking 589 cognitively unimpaired individuals aged 65 to 80. By cross-referencing subjective data from the Pittsburgh Sleep Quality Index (PSQI) with objective data from 24-hour wrist actigraphy trackers, the investigators mapped sleep characteristics against five distinct core cognitive domains: episodic memory, processing speed, working memory, executive function, and visuospatial performance.
The findings challenge standard assumptions. High objective sleep fragmentation (elevated WASO) was robustly associated with worse performance across all five cognitive domains, showing the strongest negative correlations with working memory and visuospatial processing. Conversely, short subjective sleep duration (perceiving that one slept less than 6 hours) independently predicted poor performance across the exact same domains.
Crucially, when both metrics were factored into the same statistical models, they both remained independently associated with cognitive impairment. This implies that actigraphy and self-reports are tracking entirely different neurobiological phenomena. Actigraphy catches the physical tossing and turning of sleep fragmentation , while subjective logs capture long periods of still wakefulness—such as lying frozen in bed with insomnia—that motion sensors mistake for deep sleep.
Furthermore, the study uncovered a striking age-dependent inflection point. For individuals under 70, subjective sleep metrics carried the most weight in predicting memory decline. But for those aged 70 to 80, subjective complaints lost their predictive reliability; instead, objective sleep fragmentation and frequent night awakenings became the dominant indicators of structural cognitive degradation.
Actionable Insights
-
Track and Minimize WASO: Do not just optimize for total time in bed; prioritize sleep continuity by monitoring Wake After Sleep Onset (WASO) via consumer wearables or clinical actigraphy. Accumulating high WASO is an independent risk factor for accelerated cognitive decline across all major domains, regardless of total sleep duration.
-
Maintain Subjective Duration Above 6 Hours: If your self-reported sleep duration falls below 6 hours, take aggressive corrective action. Short subjective sleep is a powerful proxy for long periods of still wakefulness and perceived poor sleep quality, which independently correlate with impaired episodic memory, processing speed, and executive function.
-
Pivot to Objective Metrics Past Age 70: Recognize that subjective sleep perception degrades with advancing age. If you or a patient are over 70, do not rely on the self-reported feeling of a “good night’s sleep”; deploy objective tracking devices to verify that underlying sleep fragmentation is not masking silent cognitive erosion.
-
Optimize for Glymphatic Clearance: Sleep fragmentation disrupts standard progression through deep slow-wave sleep cycles. Prioritize behavioral and environmental interventions (e.g., thermal regulation, alcohol elimination, and dark environments) designed to safeguard deep sleep continuity, maximizing the brain’s glymphatic clearance of neurotoxic beta-amyloid aggregates.
Source:
-
Open Access Paper: Self‑report and actigraphy measures of sleep and domain‑specific cognitive performance in older adults
-
Institutions: AdventHealth Research Institute (Neuroscience Orlando), University of Pittsburgh, Northeastern University, University of Illinois at Urbana-Champaign, University of Kansas (USA); Murdoch University (Australia).
-
Country: United States and Australia.
-
Journal Name: GeroScience.
-
Impact Evaluation: The impact score of this journal is 5.6 (Journal Impact Factor), evaluated against a typical high-end range of 0–60+ for top general science, therefore this is a High impact journal within the specialized fields of gerontology, aging biology, and longevity medicine.