Here is a recent paper Metformin: From diabetes to cancer to prolongation of life (Oct 2024 U of Milan). I noticed quite a few recent researches out there expanding its claim on many protective effects:
Diabetes Prevention: Metformin reduces diabetes risk by 31% over 3 years in at-risk populations, with sustained benefits observed over decades.
Mechanisms of Action:
Primarily acts on the gut, affecting glucose absorption and incretin hormone release.
Influences gut-liver axis to decrease hepatic glucose production.
Extended Applications:
Cancer: Potential anti-cancer properties linked to mitochondrial activity.
Cardiovascular Benefits: Suggested cardioprotective effects in men.
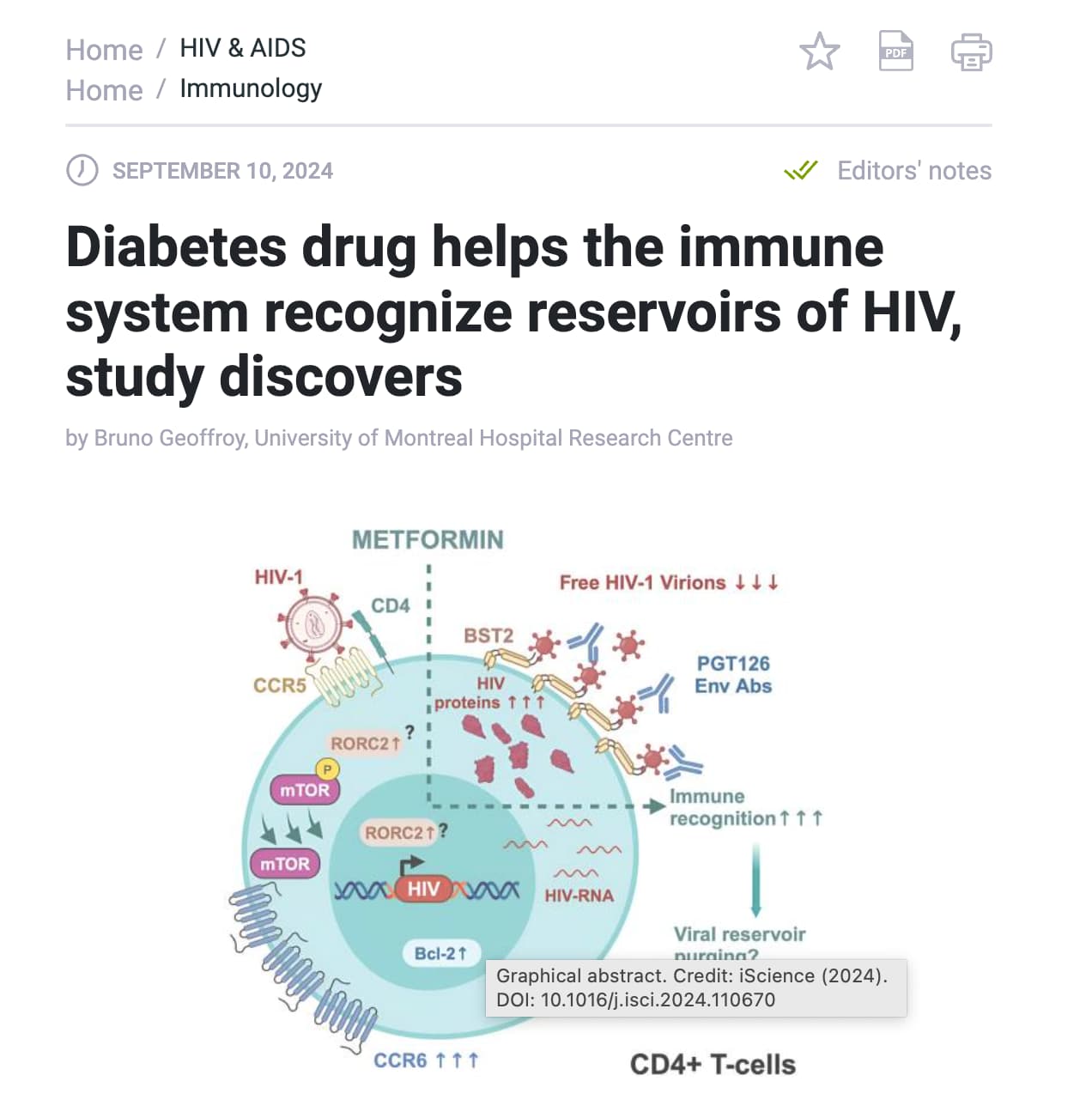
HIV: Research indicates metformin could help deplete viral reservoirs in HIV patients on antiretroviral therapy.
Not a lot people here taking metformin though, for longevity or healthspan. Anyone taking metformin here for that purpose? Heard a rumor some nobel prize winner is taking it for longevity at a conference. I believe is Juan Carlos Izpisua Belmonte of Altos Labs. @RapAdmin may be can poke around? He was presenting at All-In Summit 2024 The All-In Summit 2024 - September 8-10 - Los Angeles, CA
September 11, 2024
BUFFALO, N.Y. — The University at Buffalo is part of a nationwide study to see if a popular diabetes drug can prevent Alzheimer’s.
Millions of people worldwide take Metformin, especially to treat diabetes, and now the hope is that it could help prevent short-term memory loss from progressing to Alzheimer’s.
“It is a very exciting study because we are re-purposing a medication that has been used in millions of people, and it’s a pretty safe medication,” said Dr. Kinga Szigeti, Alzheimer‘s Disease and Memory Disorders Center Director.
A common diabetes medication, metformin, slows the growth of precancerous cells in the esophagus while some metabolic conditions accelerate it, suggests a new study.
Also this:
Several large-scale observational studies have suggested that diabetic patients taking metformin tend to live longer than non-diabetic control groups.
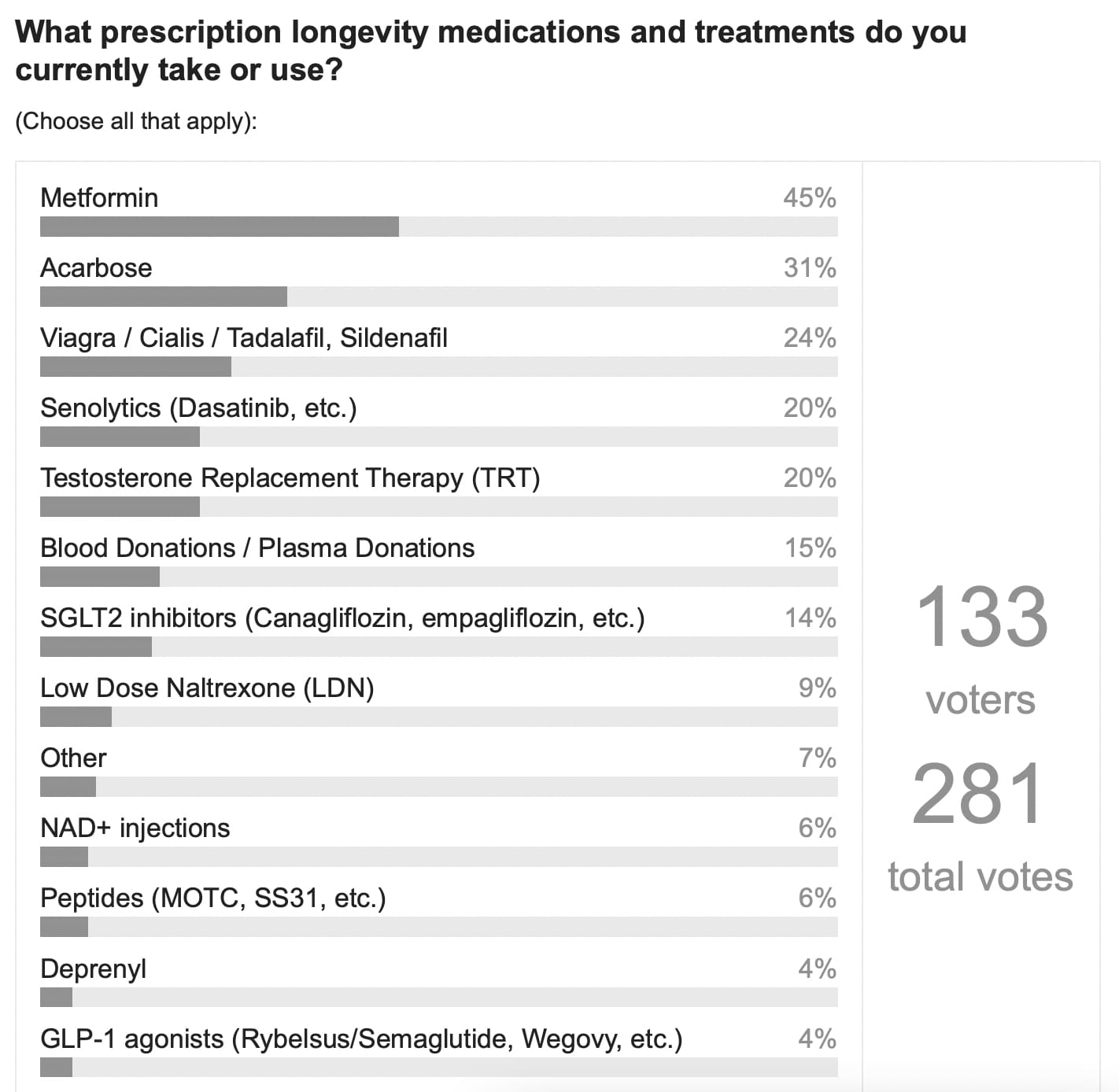
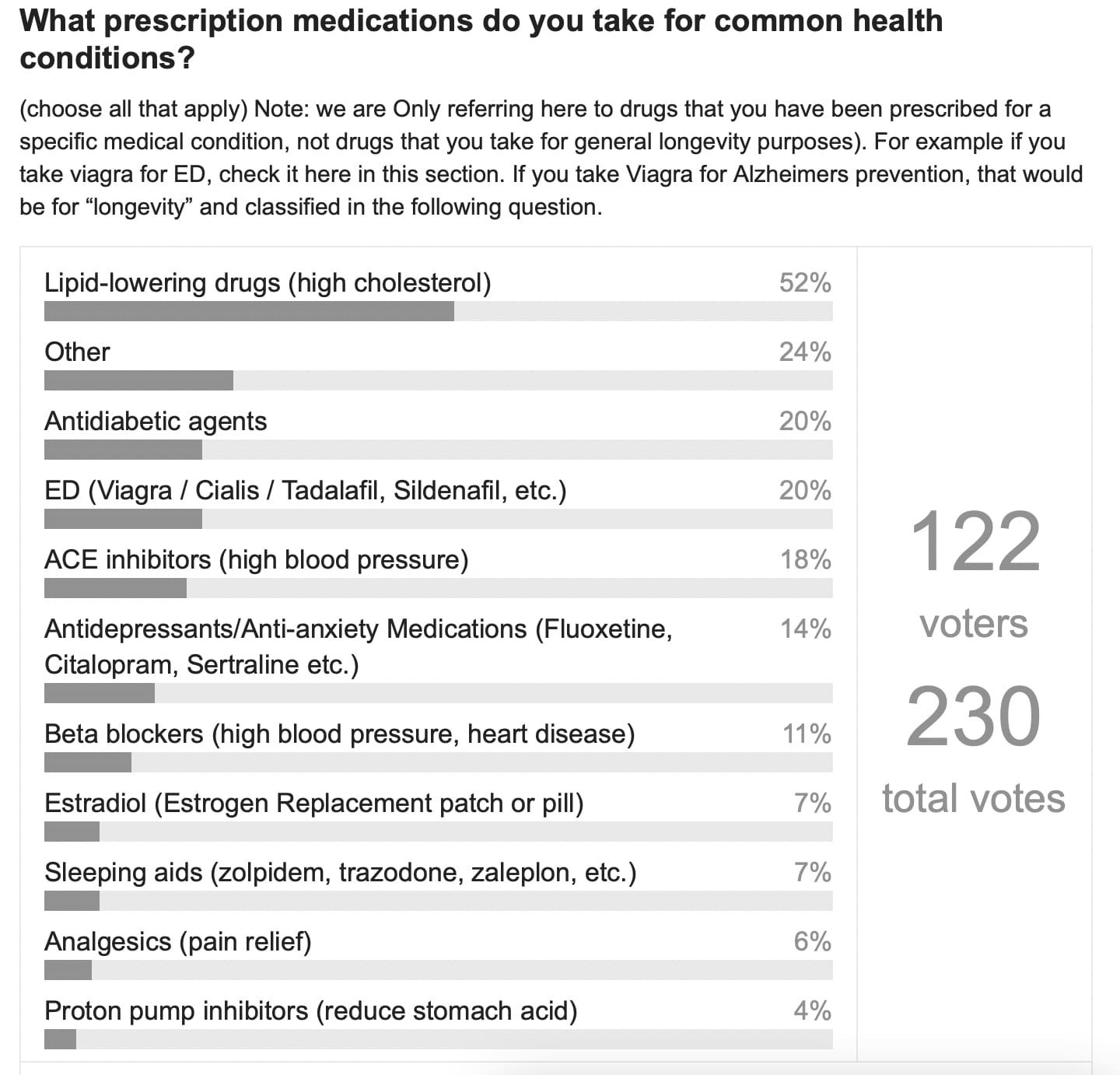
We asked about this in the poll / survey we did in 2022. I was surprised at how high the usage was. I’m not sure its changed since then… perhaps time for another poll soon?
I’m interested in this topic but, as far as I have understood, this putative effect is pretty controversial. Several (how many?) studies have suggested an improvement in lifespan, but how many others have refuted that effect? For example, in a podcast a known Italian oncologist, collaborator of the eminent professor Veronesi, cited a study led by him in northern Italy where such effect was not found.
I wonder if there is a valid review article or umbrella review on this interesting aspect.
I think the fact that metformin didn’t demonstrate benefit in the ITP trial plus Attia’s general negativity on the drug has played a role in the longevity community.
I respect Attia’s work but he frequently fails to mention that the longevity test failure was in mice. At times he treats the mouse research as if it were research on humans.
I have been taking 850 mg. with my evening meal for about 10 years mostly for longevity but also to push my A1C back from the borderline.
Assuming Juan Carlos Izpisua Belmonte of Altos Labs is taking it for longevity, why is he taking it (he is very skinny). Would you take it? If not, why not? Attia tends to be very black white so I am less to inclined to follow him blindly.
I think Attia’s biggest beef with Metformin was how it raised his lactate during exercise. I think he was using lactate as a marker of fitness, and his lactate was high at lower exertion levels (for someone of his perceived fitness level)…he guessed correctly that it was the metformin. So he quit, and he had to explain himself. BTW, I also felt the negative impact of metformin on exercise…it always felt much harder than it should when I took metformin regularly. I also quit taking it except around my rapa dosing.
The anti-aging impact of metformin (randomly assigned, with controls) in male monkeys after 40 months of treatment, a pan-omic clock assessment
—~6 year regression of brain aging, with prevention of atrophy and enhanced cognitive ability
—minimal effect on blood sugar
—evidence for multi-organ decelerated aging
I remember Attia cited another drawback of metformin, which would affect deleteriously muscle hypertrophy. Barzilai doesn’t deny that but says that strength remained the same in tested human subjects.
A lot of hubbub as it seems to me.
Not really getting all of that. Skinny has nothing to do with anything. Black and white is appropriate when deciding whether to take a drug.
I don’t take it because I see no reason to take a mitochondrial poison until there is proof that it helps. Not saying it doesn’t help, just that I don’t see enough evidence.
And the result in the ITP was actually that the metformin treated mice lived about 7% longer than the control group. 7% isn’t nothing. The difference wasn’t statistically significant, but that doesn’t mean it isn’t real, since the ITP is only statistically powered to detect larger differences.
It’s interesting that galantamine, basically a colinergic agent, has such a peculiar sinergy in C. elegans. Let’s wait for more evolved animal models.
I don’t know if metformin may cause muscle loss or just prevent proper hypertrophy with exercise. The latter would sure be detrimental in the case of people with sarcopenia wanting to gain muscle mass back…
Interesting new turns in the metformin discussion. I have no way to be certain (and I am not motivated enough to execute an N=1 Multiple Baseline w/Reversals design) but in my late 70’s, my muscle growth response was as expected when I increased weight training efforts on biceps, triceps, shoulder, and the ankle and calf muscles. Growth in these areas seems as fast as it was with comparable efforts decades ago. I can’t say the same for the quadricep and hamstring groups. I would think the answer might lie in type differences but the calf muscles are generally the same composition as the quads. Dunno.
My take on the human evidence for longevity is mixed, ranging from ~neutral to significantly positive. Moreover, when you look into the distributional statistics of the studies failing to find significance, you see more than a few positive outcomes. Doesn’t this suggest that the decision-rules should account for individual differences? At the least, it seems reasonable to postulate genetic differences as well as individual differences in starting body mass, visceral fat, etc. Placebo effects are a stretch in some of these designs,