Got it. @adssx - have either of you looked into Chris Masterjohn’s paid content on the topic, heard that it might be good
Saw this teaser
Got it. @adssx - have either of you looked into Chris Masterjohn’s paid content on the topic, heard that it might be good
Saw this teaser
Did you/anyone else ever look into TMG to lower Hcy?
4 grams of TMG consistedly lower Hcy levels across various studies. Even lower doses than that might work. Personally I am supplementing with 2g every day until more studies come out showing a benefit for brain aging.
Thanks AlexKChen! Appreciate it.
Can possibly raise LDL when more than 4g a day are used.
I haven’t looked at it. I don’t know what kind of good content can be behind a paywall on this topic. I mean: what more than the academic papers already published? Looking at these, I haven’t found evidence of benefits for Hcy-lowering therapies (besides some association studies, but by that reasoning, we would keep ApoB not too low…), so I don’t want to spend too much time on it. But I want to increase my low B12 (and check my B6…).

Thanks. More interesting that the association (that we already knew) is the potentially causal link:
Moreover, Index revealed a normalization of accelerated epigenetic aging in these individuals following treatment with tHcy-lowering B-vitamins. Our results indicate that elevated tHcy is a risk factor for accelerated epigenetic aging, and this can be ameliorated with B-vitamins.
We believe that high tHcy is causally associated with rapid aging because normalizing tHcy levels with B-vitamins decelerates biological aging over the 2-year duration of the trial. We suggest that accelerated aging may help drive the broad spectrum of maladies in people with hyperhomocysteinemia, including cardiovascular and neurodegenerative diseases, as well as cognitive decline (Smith & Refsum, 2021). These findings may have broad implications: an estimated 13.6% of men and 8.7% of women aged 60 years and above in the United States have tHcy level >13 μmol/L (Pfeiffer et al., 2008), putting them at risk for accelerated biological aging and severe health consequences. In countries that have not introduced folic acid fortification, these values are likely to be higher. tHcy can effectively be lowered with B-vitamins, which represents a safe and cost-effective approach to potentially reduce all-cause mortality risk, as well as many other adverse outcomes (Smith & Refsum, 2021) in the broader population.
(link)
I’m actually waiting for my Hcy results after 6 weeks of methyl-B12 2 mg/day… Should have the results today or on Monday…
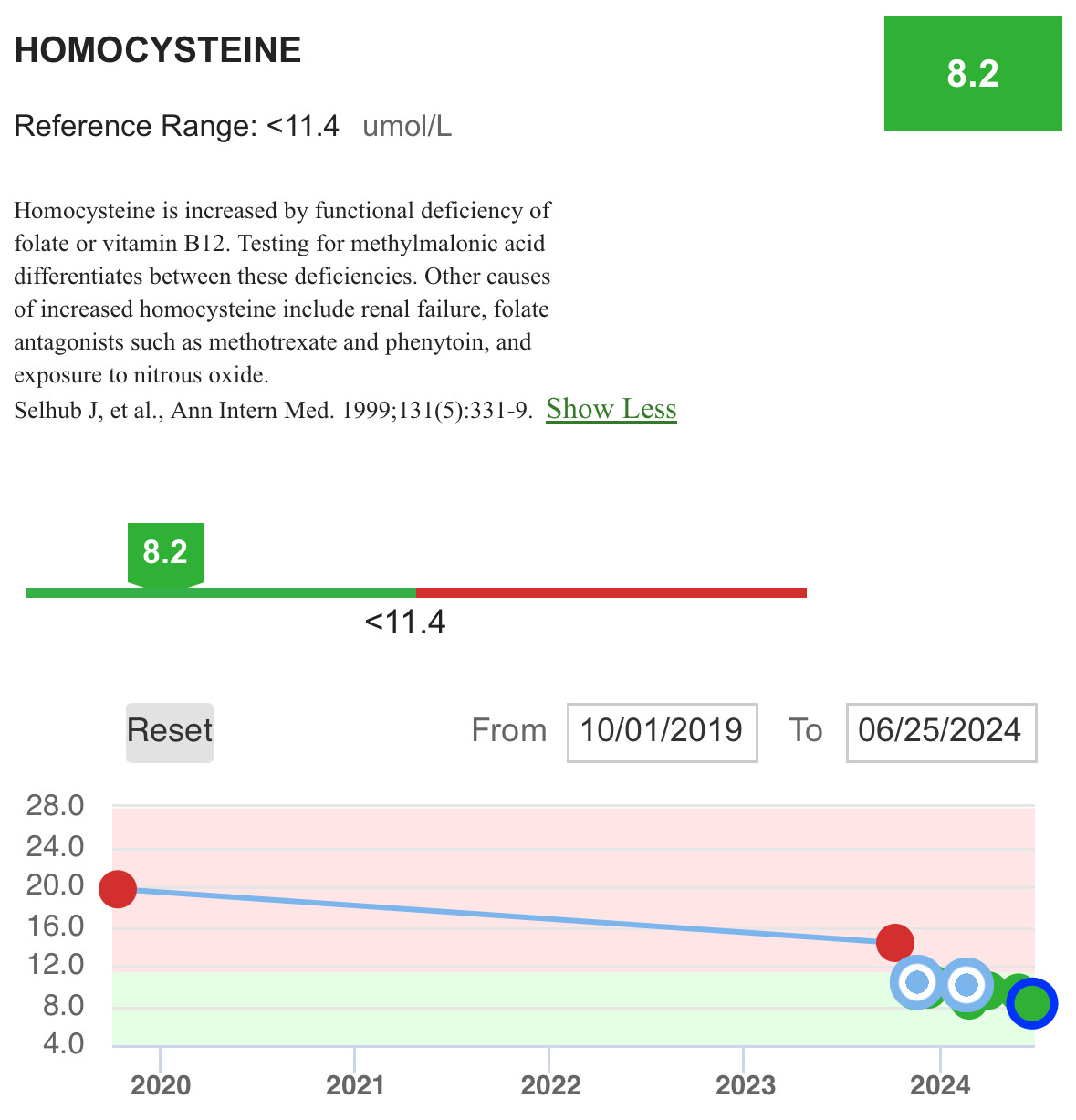
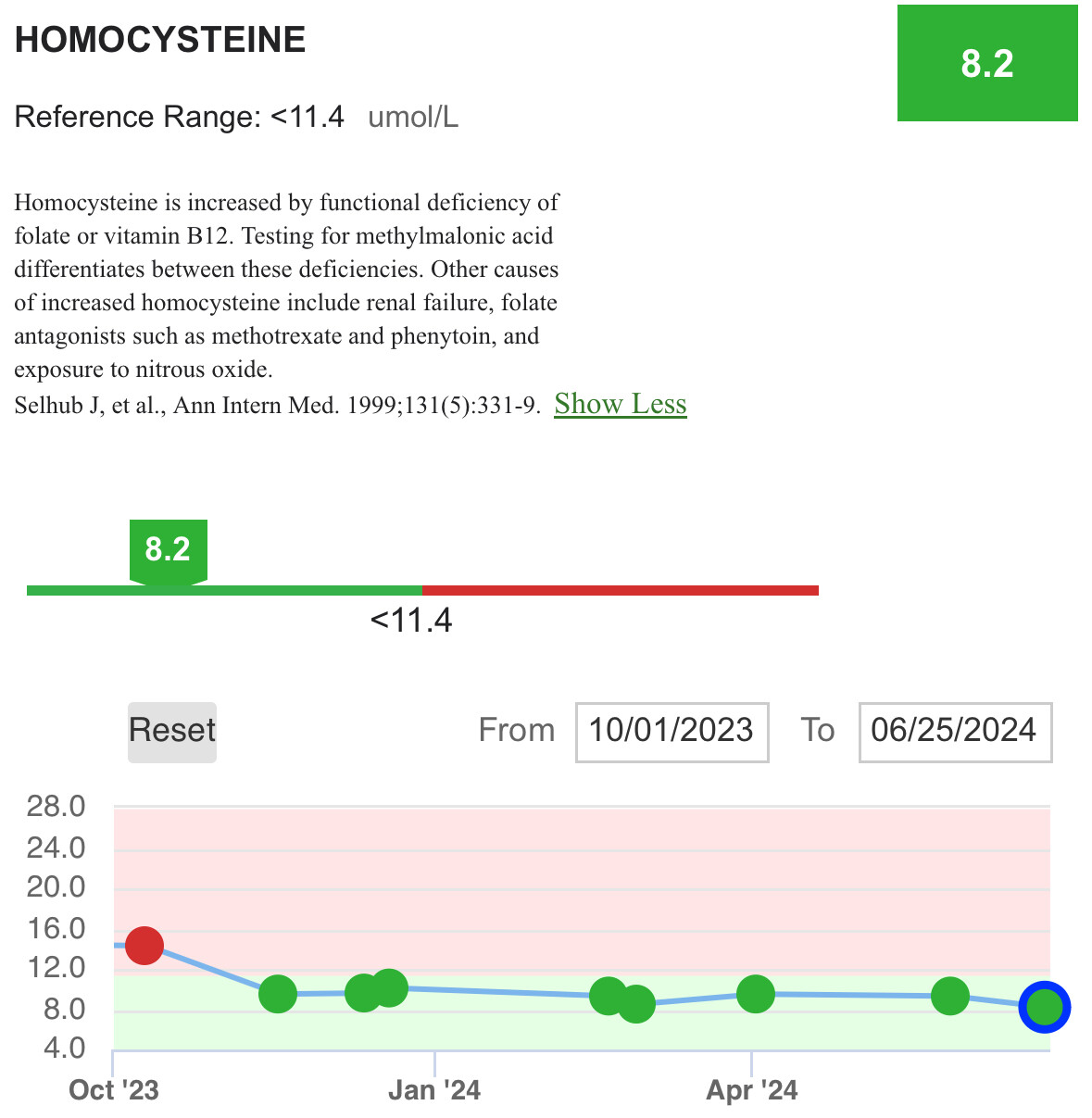
My Hcy results:
But at the same time, my B12:
My lab tells me that 1,123 ng/L is way too high and that the upper limit is 771 ng/L… So I guess I’ll go back to 1,000 µg/day supplementation…
@adssx Perhaps you can add some of the B6 and B9 per eg Peter Attia’s protocol to belp keep Hcy down without going too high on B12.
My results after this protocol are below.
(The last data points also included taking creatine daily and not just on strength training days).
(I have not yet done, but think I saw that adding a bit of B2 can help also).
Two interesting articles on homocysteine:
Yes, I think I’ll go back to methyl-B12 1,000 µg/day sublingual and add a simple B complex (such as this one) that includes B2, B6 and B9. Which B6 and B9 are you taking?
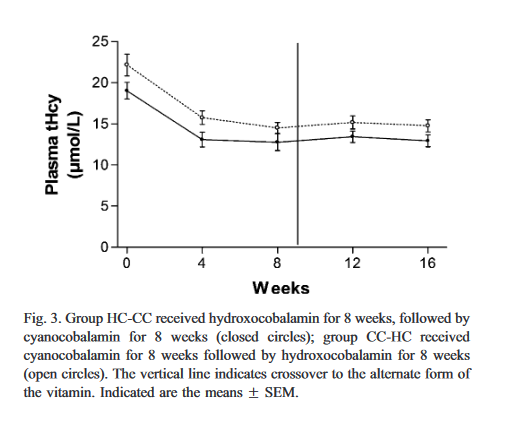
Cyanocobalamin is as effective as hydroxocobalamin in lowering homocysteine levels in a randomized, crossover trial.
Well, do you have any data showing that cyanocobalamin harming kidneys without kidney failure?
The obvious risk is vitamin b12 deficiency from using a less studied and less shelf stable form of vitamin b12.
Yes: “A trial in patients with diabetic nephropathy randomized to placebo vs. folate 2.5 mg, B6 25 mg and cyanocobalamin 1,000 μg daily showed faster decline of renal function, and a doubling of cardiovascular events, with B vitamins.” (B vitamins for NASH: Use methylcobalamin, not cyanocobalamin 2022)
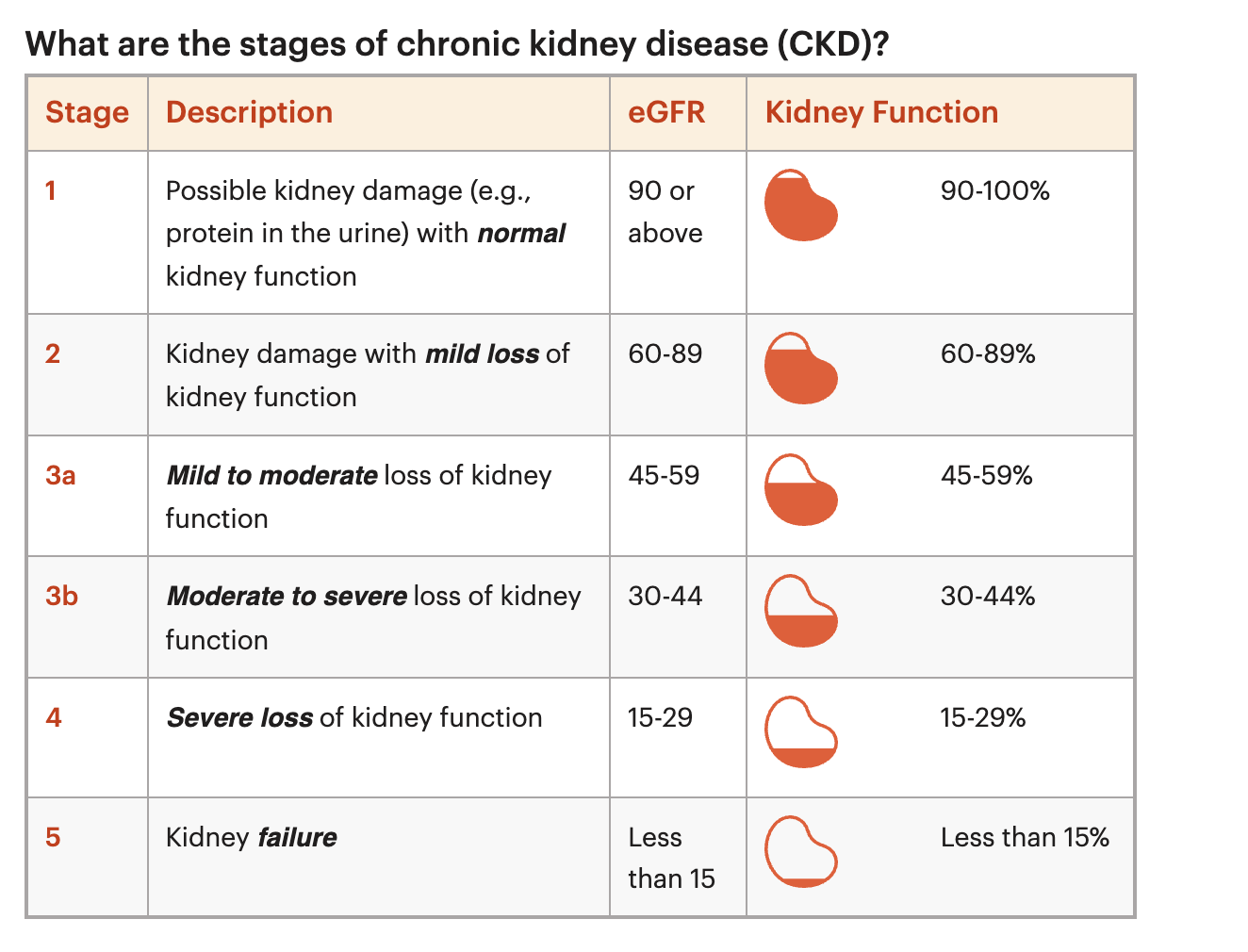
Note: “Nephropathy is the deterioration of kidney function. The final stage of nephropathy is called kidney failure, end-stage renal disease, or ESRD.” We all have some kind of loss of kidney function after the age of 30/40.
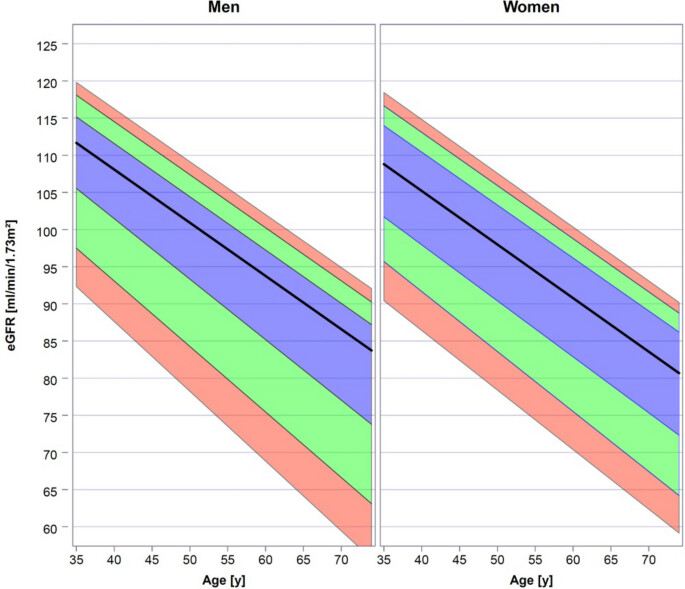
Is the above relevant if your eGFR is still above 90? Not at all if you only occasionally supplement with low doses of cyanocobalamin. However, if you plan to supplement with B12 at a “large” dose (≥ 1,000 µg) for the rest of your life, then I think so. You might still prefer to use cyanocobalamin as long as your kidney function is perfect (eGFR > 90) and then switch to methylcobalamin if you ever go below that. To each their own way.