Lustgarten has lower hcy with higher BCAAs…
1 Like
Thanks. I can’t see that online yet though, here is his collection on homocysteine posts: Homocysteine | Michael Lustgarten
Do you have any link or color on his protocol?
One issue is that BCAAs seem to be not optimal to raise from a longevity perspective? Or did he impact homocysteine by lowering BCAAs?
Btw - homocysteine might be bad for longevity also via mTORC1 activation…
Parkinson’s disease and vitamins: a focus on vitamin B12 2024

More rapid motor progression has also been associated to Vit B12 deficiency and HHcy as highlighted in the study conducted by M. C. Bakeberg et al. encompassing 205 PwPD. The authors demonstrated that male PwPD presenting with HHcy had significantly lower levels of Vit B12 and more rapid motor progression. In fact, they noted an increase of 0.77 points on the UPDRS part III for each additional 1 μmol/L of serum Hcy (Table 1) (Bakeberg et al. 2019).
“Regarding non-motor symptoms in PD, Vit B12 has been individually linked to cognition and is used as a therapy for Vit B12 related cognitive impairment (McCarter et al. 2020b). Yet, Vit B12 deficiency and HHcy are both catalysts for a singular non-motor PD phenotype characterized with cognitive dysfunction. Higher baseline Vit B12 has been associated with lower risk of developing dementia among PwPD (Müller et al. 2013). In this latter study, a cut-off value of Vit B12 has been established (> 587 ng/L) to reduce the risk of developing dementia with reasonable sensitivity and specificity at 5 and 10 years from PD diagnosis. Thus, we recommend to regularly assess cognitive function among PwPD, test Vit B12 serum levels along with Hcy and MMA levels.”
““Since the list of contraindications of Vit B12 is really restrained to Leber optic neuropathy as it may aggravate it and to advanced renal failure since the injections may include aluminum in its components, we may suggest to consider systematically supplementing PD patients with B12 in the absence of contraindications or potential adverse effects””
Compelling evidence has been provided pinpointing that Vit B12 effectively hinders the formation of αSN fibrils and reduces neuronal cytotoxicity. Such conclusion was mainly established based on animal models of PD and in-vitro experiments. Furthermore, the question whether Vit B12 should be considered as symptomatic treatment in PD or as a disease modifying therapy remains triggering and unresolved. Thus, it is essential to approach such hypothesis with caution and aim to demonstrate it in case–control studies including PwPD.
As for clinical correlates, Vit B12 deficiency and HHcy do predict more rapid motor progression and cognitive dysfunction among PwPD and thus modulate PD clinical phenotypic variability. We highlighted that PN is an underestimated problem among PwPD, especially among those receiving LCIG infusion. It remains crucial to regularly warrant a close monitoring of Vit B12, Hcy and MMA as well as the nutritional status of PwPD in general. We provided a guideline detailing the key aspects of managing LCIG-treated PwPD. In this context, the subcutaneous LDopa infusion pump could offer an intermediate approach between the two conventional administration routes of LDopa, potentially mitigating some side effects.
Finally, while Vit B12 supplementation has practical implications in neurological diseases and seems to yield benefits in PD, the dearth for comprehensive understanding surrounding its CNS bioavailability and mechanisms of action presents an obstacle to elucidate among PD patients. As we move forward, it becomes increasingly evident that further interventional studies are essential to provide evidence-based valuable insights and recommendations regarding the monitoring of Vit B12 deficiency and its biomarkers and to establish accurate guidelines for Vit B12 supplementation in PD.
For the 587 ng/L B12 cutoff, see: Higher vitamin B12 level at Parkinson’s disease diagnosis is associated with lower risk of future dementia 2020
Vitamin B12 cutoff of <587 ng/L was 87% sensitive and 70% specific (AUC 0.79, 95% CI 0.60-0.98) distinguishing patients with dementia. PD patients with vitamin B12 levels <587 ng/L were 5.4 times more likely to develop dementia, with 50% having dementia within 5 years of PD diagnosis compared with 11% in those with a vitamin B12 level of ≥587 ng/L (p < 0.05).
4 Likes
Thorne Methylcobalamin 1 mg then? Is it 1 mg a day?
I do roughly Peter Attia’s protocol and measure B6, B9, B12 and Hcy. (And in most recent also measuring B2).
As near vegan I also supplement with creatine.
Requirements for these alternative forms have not been fully elucidated and common recommendations are for 1,000 µg/day.
For methylcobalamin recommendation is 1,000 ug/day or 1 mg/day.
I wonder if elderly needs higher doses as I think B12 absorption goes down with age.
@Neo do you take it from Thorne? 1 mg a day?
In the comments:
Before recommending methyl or adenosyl, I would want a study that compares MMA levels before and after supplementing at a range of dosages to determine what amounts consistently reduce MMA levels in most people. I’m guessing dozens of people for each dosage would be required to reach statistical meaningfulness.
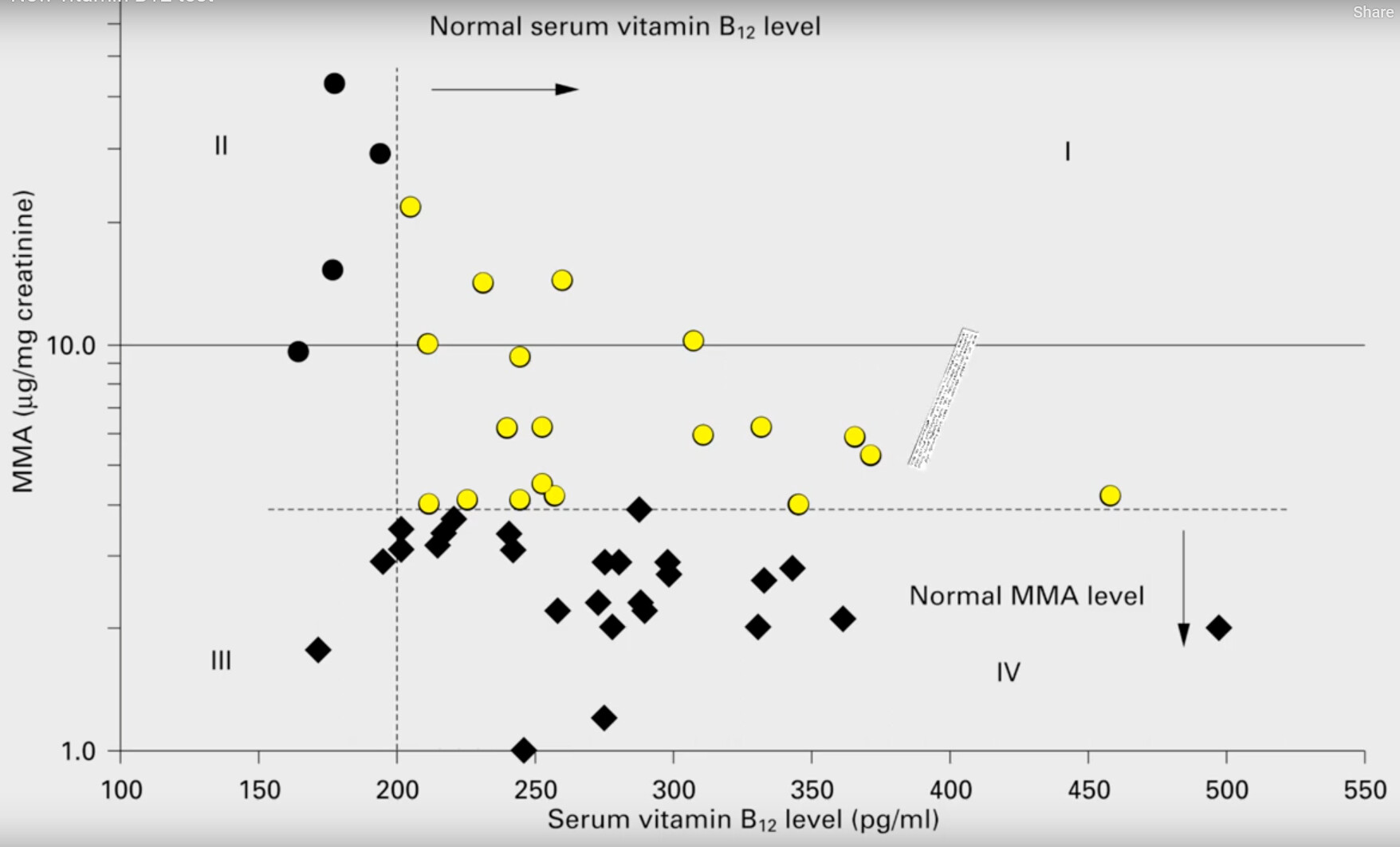
Serum B12 not so accurate:


Lots of people have normal serum B12 levels but deficient in B12 (elevated MMA levels), shown in yellow.
1 Like
Even with 1,000 µg/day (sublingual methylcobalamin), my serum B12 is still below 500 ng/L. I’m considering doubling to 2,000 µg/day.
1 Like
How would you monitor if dosage is too high at 2000 ug/day? Would it be via serum B12 only and is nothing else needed?
Yes, B12 only (together with other regular blood tests, especially B9 and iron as “A complex interaction occurs between folic acid, vitamin B12, and iron. A deficiency of folic acid or vitamin B12 may mask the deficiency of iron; so when taken as dietary supplements, the three need to be in balance.”).
1 Like
I’ve been using the brands Peter Attia uses:
For B12 (and folate) I’ve used

Or

And

At 2 of those per day I felt good (and did move my Hcy down), but slightly high on B12, so went down to 1 per day and will see how Hcy looks (don’t have the latest yet), do wonder if my B12 now is not quite optimal and could be raised just slightly (@adssx @A_User any thoughts?)
Have also been using this based on Peter (3 times a week first, but might have overshot so no 2 times a week)
1 Like
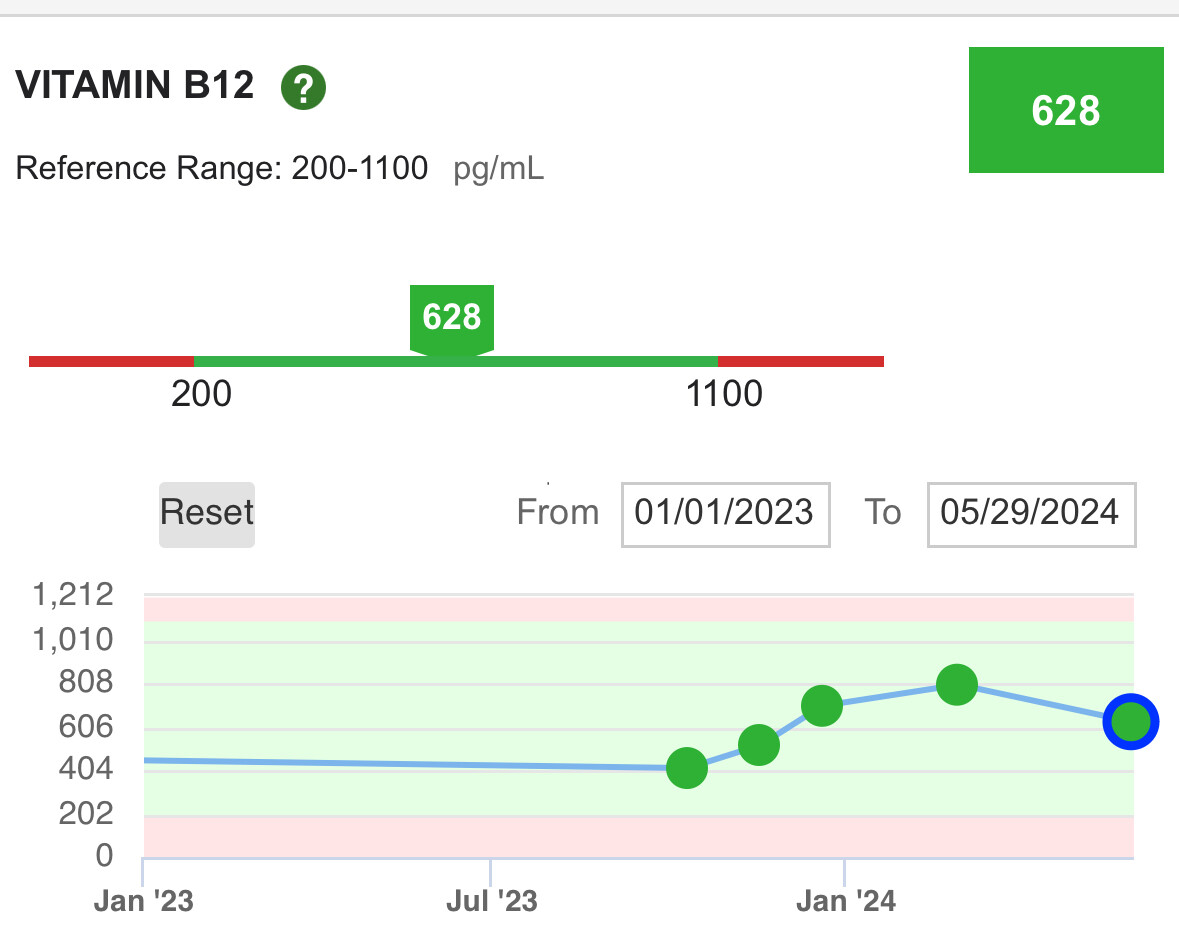
I don’t know, I would be happy with this level ![]()
1 Like
If you want to know for sure, you should test homocysteine and MMA levels.
@A_User update, latest homocysteine just came in:
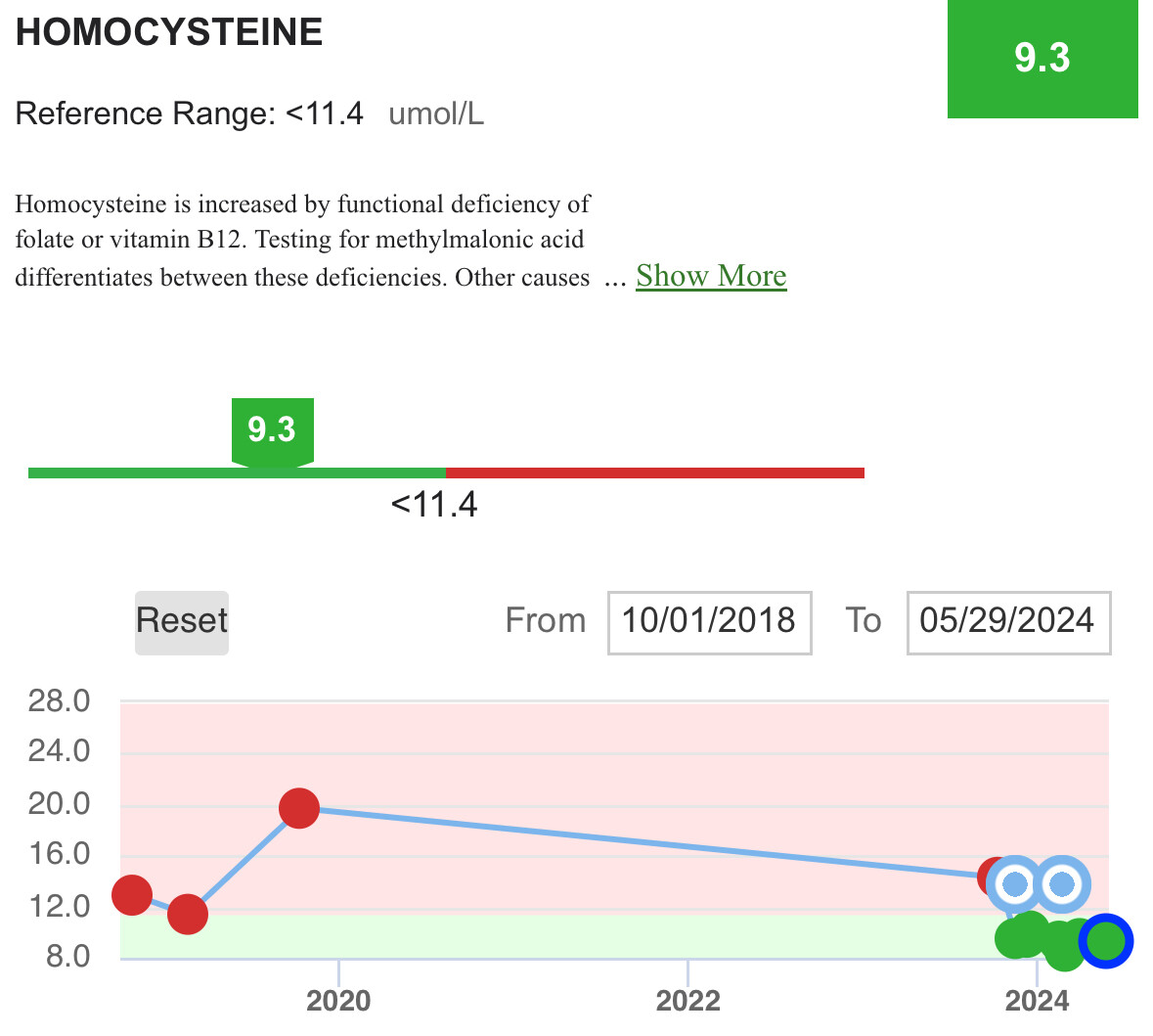
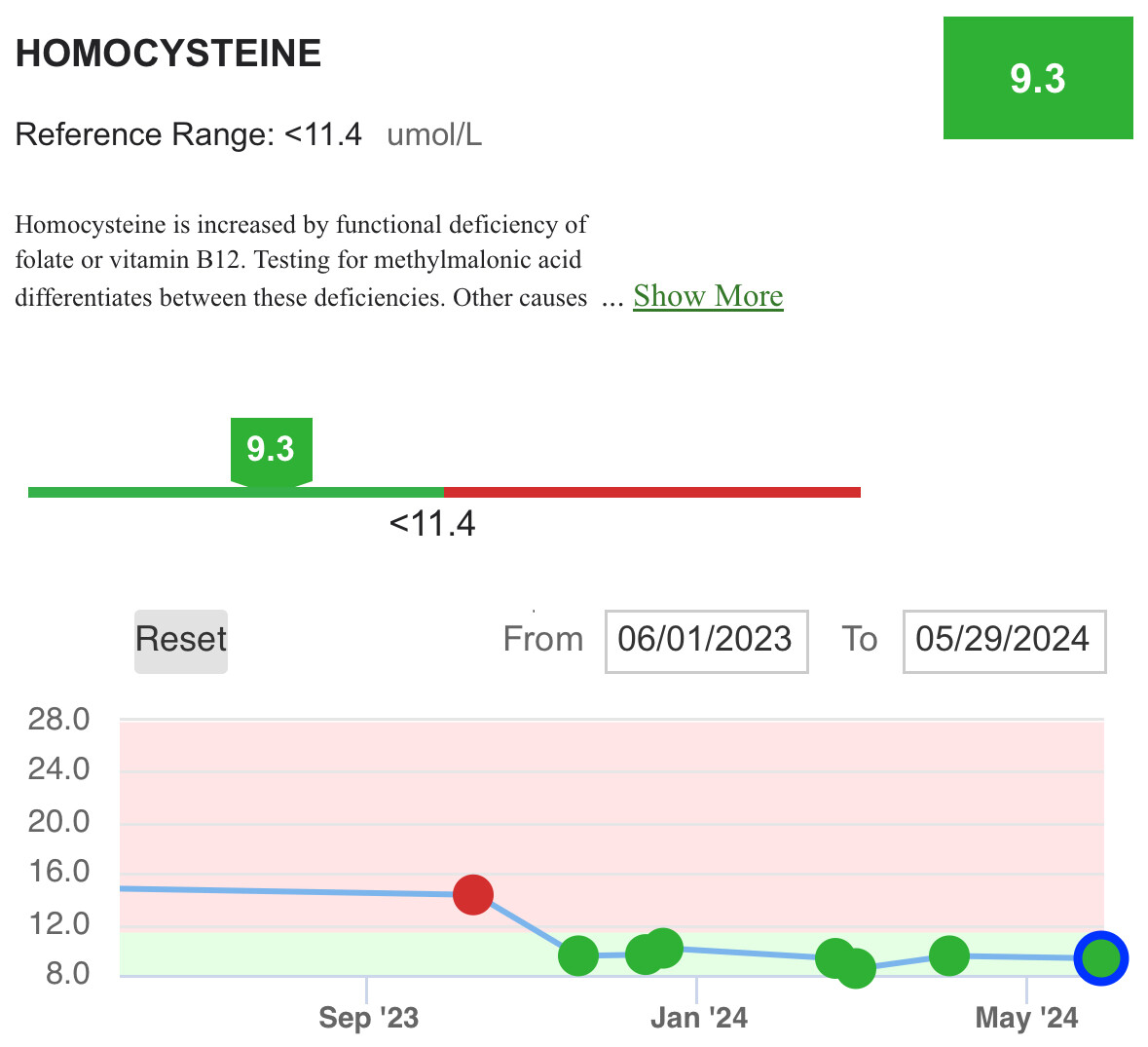
So even if I decreased the B12 (and B6 and B9) - while adding a bit more creatine - going in that last datapoint the Hcy did not really go up.
1 Like
I would test MMA too once you’ve settled for a dose you like. You took 2 mg previously of methycobalamin and it lead to a bit high levels?
Updated to the correct screenshot now, so see my latest test and time series of Hcy above now.
Yes, took 2000 MCG until about 6-7 weeks before the last test when I went down to 1000 MCG.
MMA not directly cheap in the US. I found this:
Has anyone seen a cheaper one?
@A_User what would you want to see from MMA in my case (vs the info on B12 and Hcy we have the time series on)?
There are some places it is sold for $100, but you can take a urinary MMA test which is much cheaper and the same.
You can use that test to determine whether you are getting B12 deficient or not. I would test it once after you have a dose you’re happy with then another time some time later to make sure it isn’t decreasing.
From Perplexity:
The urinary methylmalonic acid (MMA) test and the serum MMA test are both used to detect vitamin B12 deficiency, but they have some key differences:
Urinary MMA Test
- Measures the level of MMA excreted in the urine over a 24-hour period or from a random urine sample.
- Considered more sensitive than serum MMA for detecting mild or early vitamin B12 deficiency.[1][3]
- Requires collecting all urine over 24 hours or providing a random sample, which is more cumbersome than a blood draw.
- Urinary MMA levels correlate well with serum MMA levels in individuals with normal kidney function.[3]
- A fasting urinary MMA level above 1.5-2 μmol/mmol creatinine is suggestive of vitamin B12 deficiency.[3]
Serum MMA Test
- Measures the level of MMA in the blood through a simple blood draw.
- Less sensitive than urinary MMA for detecting mild B12 deficiency, but more convenient.[1][4]
- Serum MMA levels above 0.3-0.4 μmol/L are considered elevated and indicative of vitamin B12 deficiency.[1][4]
- Serum MMA can be falsely elevated in individuals with renal impairment since MMA is cleared by the kidneys.[4]
In summary, while both tests can detect vitamin B12 deficiency, the urinary MMA test is generally considered more sensitive for identifying early or mild deficiency states.[1][3] However, the serum MMA test is more convenient as it only requires a blood sample.[1][4] The choice between the two may depend on the clinical scenario and the degree of suspicion for vitamin B12 deficiency.
Citations:
[1] Methylmalonic Acid (MMA) Test: MedlinePlus Medical Test
[2] Methylmalonic Acid Test: Types, What to Expect, and More
[3] Use of fasting urinary methylmalonic acid to screen for metabolic vitamin B12 deficiency in older persons - PubMed
[4] https://www.testing.com/tests/methylmalonic-acid/
[5] https://www.cincinnatichildrens.org/-/media/Cincinnati-Childrens/Home/service/p/pathology/mass-spectrometry/MMA-urine-test-info-sheet-FINAL.pdf
1 Like
Ok, found that Market is less than 50% of Ulta Labs, at 69 dollars.
Will try and do the next time k go to LabCorp (normally use Quest).
It can take a very long time to become deficient from B12 because of B12 stores, but the consequences can be permanent and debilitating.
1 Like
Btw, are you also optimizing B6 and B9? Any thoughts on those? (Like introducing the MMA test seems very valuable to understand B12 status).
I haven’t yet, no. But I am starting a zinc supplement (Fuhrman recommends it, etc), and I’ve been low in zinc in the past. 15 mg zinc picolinate.