I had high homocysteine levels both from genetics (mthfr) and health issues (taking high dose PPIs for GERD). Now my tests come out at around 7. For me, taking b12 and methyl folate helped some, and taking choline seemed to help a bit. The thing that apparently helped the most was NAC. I’ve been taking it for a couple years now and my HST levels dropped by around 4. I was taking 1.2gms a day but now with the data of glynac, I’ve bumped it up to 2.4gms a day
3 Likes
> what are the 1st, 10th, 25th, 50th, 75th, 90th, and 99th percentile homocysteine concentration of people?
The percentiles for homocysteine concentration in people would vary based on factors like age, diet, and health. Some general estimates include:
1st percentile: Around 5 μmol/L or less. Very low homocysteine, likely indicating adequate B vitamin status and metabolism.
10th percentile: Around 7 μmol/L. Still on the lower end of the normal range; low risk of deficiency or issues.
25th percentile: Around 8-9 μmol/L. Within the normal, healthy range but may indicate some increased risk of B vitamin deficiency or impaired metabolism in some cases.
50th percentile (median): Around 10-12 μmol/L. The median for a generally healthy population likely with adequate but not excessive B vitamin and metabolism status.
75th percentile: Around 13-15 μmol/L. On the higher end of normal; some risk of deficiency/impaired metabolism for certain individuals. Supplements/diet changes could help.
90th percentile: Around 16-18 μmol/L. Some risk of hyperhomocysteinemia which can increase heart disease risk; warrants diet/lifestyle evaluation and potentially B vitamin treatment for some.
99th percentile: Around 19 μmol/L or above. Very high homocysteine which may indicate a genetic issue or B12/folate deficiency; requires medical evaluation and treatment to lower risk.These are general estimates. The precise percentiles would depend on a variety of individual and population factors. Both high and low homocysteine can indicate issues in some cases. Elevated homocysteine is a risk factor for heart disease, but levels should be evaluated in context. A doctor can assess homocysteine along with symptoms and other health factors to determine appropriate treatment or further testing. Diet/lifestyle changes and B vitamin supplements may help address high homocysteine, but medical advice is necessary for individual cases.
> what are the 1st, 10th, 25th, 50th, 75th, 90th, and 99th percentile homocysteine concentration of 25-year olds?
The percentiles for homocysteine concentration in 25-year-olds would likely be generally lower than for older populations, but the exact values would depend on factors like diet and health in 25-year-olds. Some estimates could be:
1st percentile: Around 4 μmol/L or less. Very low homocysteine in healthy young people with adequate nutrition.
10th percentile: Around 6 μmol/L. Still low, indicating good B vitamin and metabolism status for age.
25th percentile: Around 7-8 μmol/L. Within the healthy range but some risk of deficiency/impaired metabolism in less healthy individuals.
50th percentile (median): Around 8-10 μmol/L. The median for 25-year-olds would likely be on the lower end of normal, reflecting good health and nutrition at this age.
75th percentile: Around 10-12 μmol/L. Higher than median but still normal for age; some may have deficiencies or impaired metabolism, warranting diet/lifestyle evaluation.
90th percentile: Around 13-15 μmol/L. Elevated for age and warrants homocysteine-lowering changes; some risk of hyperhomocysteinemia and related health issues in less healthy individuals.
99th percentile: Around 16 μmol/L or above. Very high for age and requires medical evaluation; may indicate genetic issues or severe deficiency that necessitates treatment to reduce risks.However, these are rough estimates. The precise homocysteine percentiles for 25-year-olds would depend on the attributes and diets/lifestyles of people of this age. In general, homocysteine levels would likely be lower than in older populations. But both high and low homocysteine can indicate issues at any age, so values should be evaluated based on symptoms and other health factors. Medical advice is necessary for individual cases of very high or very low homocysteine.
> what are the 1st, 10th, 25th, 50th, 75th, 90th, and 99th percentile homocysteine concentration of 18-year olds?
The percentiles for homocysteine concentration in 18-year-olds would likely be lower than for older populations, reflecting good health and nutrition at this age. Some estimates could be:
1st percentile: Around 3 μmol/L or less. Very low homocysteine in healthy young people with adequate nutrition.
10th percentile: Around 5 μmol/L. Still low, indicating good B vitamin and metabolism status for age.
25th percentile: Around 6-7 μmol/L. Within the healthy range but some risk of deficiency/impaired metabolism in less healthy individuals.
50th percentile (median): Around 7-8 μmol/L. The median for 18-year-olds would likely be low, reflecting good health and diet at this age.
75th percentile: Around 8-9 μmol/L. Higher than median but still normal for age; some may have deficiencies or impaired metabolism, warranting diet/lifestyle evaluation.
90th percentile: Around 10-12 μmol/L. Elevated for age and warrants homocysteine-lowering changes; some risk of issues in less healthy individuals.
99th percentile: Around 13 μmol/L or above. Very high for age and requires medical evaluation; may indicate genetic issues or severe deficiency that necessitates treatment.However, these are rough estimates. The precise homocysteine percentiles for 18-year-olds would depend on the attributes and diets/lifestyles of people of this age. In general, homocysteine levels would likely be lower than in older populations. But both high and low homocysteine can indicate issues at any age, so values should be evaluated based on symptoms and other health factors. Medical advice is necessary for individual cases of very high or very low homocysteine.
2 Likes
Homocysteine-lowering interventions seem useless for hypertension: Rilmenidine vs Telmisartan or other BP meds for Longevity - #84 by adssx
But are they useful for anything at all? It’s not convincing:
- Association Between Plasma Homocysteine Level and Mortality: A Mendelian Randomization Study 2023: “In contrast to the results of conventional multivariate analysis, the association between plasma homocysteine and all-cause and cardiovascular mortality was not statistically significant in MR analysis.”
- Is High Plasma Homocysteine a Direct Cause of Cardiovascular Disease and Mortality? 2023: “Despite abundant observational epidemiologic evidence, it is unclear whether hyperhomocysteinemia is a mechanistic risk factor with a direct causal effect for CVD or only risk indicator without any direct effects. […] Furthermore, several recent MR studies have failed to provide a causal link between hyperhomocysteinemia and various CVDs including coronary heart disease, acute myocardial infarction, systolic and diastolic blood pressure, atrial fibrillation, congestive heart failure or cardiomyopathy. Based on current evidence, high plasma homocysteine level is unlikely to act as a mechanistic risk factor with a direct causal effect for CVD.”
- Plasma homocysteine concentrations and depression: A twin study 2021: “The findings argue against a causal role for homocysteine in the development of depression.”
- The effect of homocysteine-lowering therapy on the formation of carotid atherosclerosis: A follow-up study in the rural areas of northwest China 2023: “In this program, people with baseline hyperhomocysteinemia were given 800 μg folic acid and 500 μg vitamin B12 daily to reduce their serum levels of Hcy, and they were followed for three years. […] In participants with hyperhomocysteinemia, we observed that 3-year treatment with vitamin B12 and folic acid did not prevent CIMT increasing, carotid plaque formation, and carotid stenosis”
- Causal effects of circulating vitamin levels on the risk of heart failure: a Mendelian randomization study 2023: “Evidence from our study does not support the causal effects of circulating vitamin levels on HF. Therefore, there may be no direct beneficial effects of vitamin intake on the prevention of primary HF.”
- Plasma homocysteine levels and risk of congestive heart failure or cardiomyopathy: A Mendelian randomization study 2023: “Genetically predicted homocysteine level was not associated with congestive heart failure or cardiomyopathy risk. It is unlikely that homocysteine-lowering therapy decreases the incidence or improves the outcomes of congestive heart failure and cardiomyopathy.”
- No causal effects of plasma homocysteine levels on the risk of coronary heart disease or acute myocardial infarction: A Mendelian randomization study 2019: “The findings from this Mendelian randomization study indicate no causal relationship between plasma homocysteine levels and coronary heart disease or acute myocardial infarction. Conflicting findings from observational studies might have resulted from residual confounding or reverse causation.”
- A Mendelian Randomization Study of Plasma Homocysteine Levels and Cerebrovascular and Neurodegenerative Diseases 2021 “Meanwhile, there was no evidence of association between plasma Hcy level and other types of IS, transient ischemic attack (TIA), or neurodegenerative disease.”
- Effect of Vitamin B Supplementation on Cognitive Function in the Elderly: A Systematic Review and Meta-Analysis 2019: “Raised total plasma homocysteine is associated with an increased risk of cognitive impairment and dementia, although available evidence from randomized controlled trials shows no obvious cognitive benefit of lowering homocysteine using B vitamins.”
- Long-Term Intake of Folate, Vitamin B6, and Vitamin B12 and the Incidence of Parkinson’s Disease in a Sample of U.S. Women and Men 2023: “Our results do not support the hypothesis that a higher intake of folate or vitamin B6 would reduce PD risk in this population. Our results provide moderate support for a possible protective effect of vitamin B12 on the development of PD.”
On the other hand, homocysteine-lowering interventions might lower the risk of stroke:
- Phenome-wide association study of genetically predicted B vitamins and homocysteine biomarkers with multiple health and disease outcomes: analysis of the UK Biobank 2023
- Homocysteine, B vitamins, and cardiovascular disease: a Mendelian randomization study 2021: “This study reveals suggestive evidence that B vitamin therapy and lowering of tHcy may reduce the risk of stroke, particularly subarachnoid hemorrhage and ischemic stroke.”
- Problem in the Recent American Heart Association Guideline on Secondary Stroke Prevention: B Vitamins to Lower Homocysteine Do Prevent Stroke 2022: “When considering all the best external evidence, it is clear that B vitamins do prevent stroke, but in the early secondary stroke prevention studies, the benefit of B vitamins in participants with good renal function was apparently offset by harm from cyanocobalamin among participants with renal failure (level B-R evidence). We review the evidence that B vitamins should be used to prevent stroke, both in primary and secondary stroke prevention (class 2a recommendation). We also review issues in folate metabolism that require further study, with regard to the form of folate to be used for stroke prevention. We recommend that the guideline be revised to say that B vitamins to lower homocysteine prevent stroke and that methylcobalamin or hydroxycobalamin should be used instead of cyanocobalamin.”
- Cochrane 2017: “In this third update of the Cochrane review, there were no differences in effects of homocysteine‐lowering interventions in the form of supplements of vitamins B6, B9 or B12 given alone or in combination comparing with placebo on myocardial infarction, death from any cause or adverse events. In terms of stroke, this review found a small difference in effect favouring to homocysteine‐lowering interventions in the form of supplements of vitamins B6, B9 or B12 given alone or in combination comparing with placebo.”
That being said, although the association between homocysteine levels and CVD is non-causal, it is quite strong, and I’ll get tested to know my baseline levels and better understand my “baseline” CVD risk besides genes + Lp(a) + family history.
5 Likes
Peter Attia targets 8-9 as upper level of homocysteine for his patients, using methylated B vitamins to achieve this target.
From his show notes (#257): “Peter’s concern is mostly cardiovascular because there is good evidence that homocysteine impairs clearance of two molecules (SDMA and ADMA [symmetric and asymmetric dimethylarginine]) that impair nitric oxide synthase”
But in that podcast with Tommy Wood (#257) they also discuss the role of homocysteine levels in cognitive decline. They discuss the VITACOG study, in which cognitive decline and brain atrophy were reduced in the setting if lower homocysteine levels. Moreover, this effect was greatest in those with highest Omega 3 status.
So the key point they are making is that you need both low homocysteine AND high omega 3 for the cognitive benefits.
They cite 3 studies: VITACOG, B-proof, and OmegAD.
https://www.sciencedirect.com/science/article/pii/S0002916523277655?via%3Dihub
So I’m now trying to get my homocysteine low and omega 3 index high.
4 Likes
So if I understand correctly, homocysteine-lowering interventions alone are useless unless combined with omega 3 supplementation (or in people with already high omega 3)?
3 Likes
“Our results do not support a causal association between elevated homocysteine and risk, severity, and progression of AD.” (Genetic influence of plasma homocysteine on Alzheimer’s disease 2018)
So for sure homocysteine-lowering alone is useless. TBC if really useful if combined with omega 3 ![]()
3 Likes
That was certainly the gist of Peter Attia’s discussion with Tommy Wood around preventing cognitive decline. Decreasing homocysteine is effective only in setting of high omega3 status.
1 Like
What is proven so far is the opposite: omega 3 supplementation is only effective at high dose AND in the context of low homocysteine:
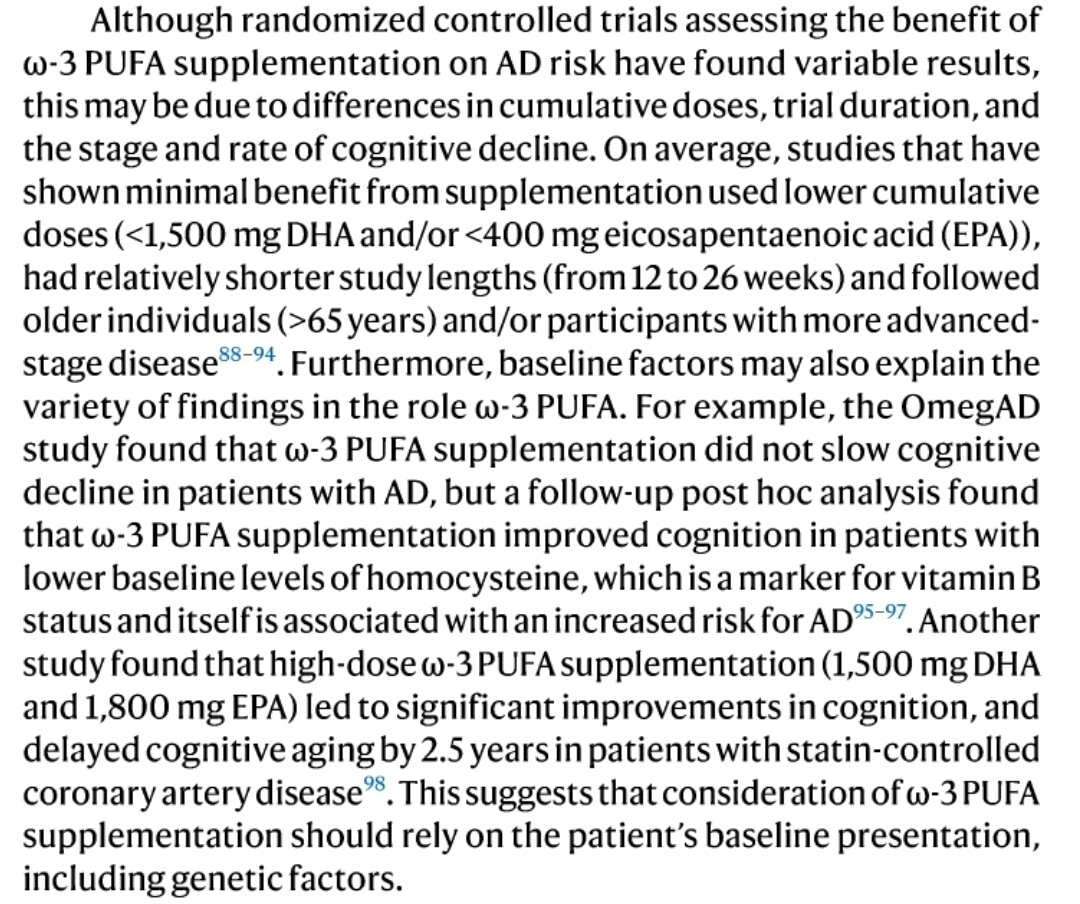
What is unknown (but a reasonable assumption) is whether homocysteine-lowering interventions (via methyl-B9 and methyl-B12 supplementation) combined with high-dose omega 3 supplementation is effective. We could answer this question by looking at multi vitamin trials: was supplementation effective in people with high homocysteine at baseline?
3 Likes
Interesting, thanks. On the whole, seems like reasonable approach to keep homocysteine low and omega-3 high.
My most recent Omega index was 6% (trying to get above 8) and homocysteine was 8.8 (trying to stay below 9.
1 Like
@adssx et al, people may want measure those two above and see if decreasing homocysteine also decreases them
They seems like good datapoints to have in themselves
1 Like
Thanks. Are these easy to test? (I couldn’t find it after a quick Google search) Is there any evidence that lowering them improves outcomes (ACM, AD, other NDDs, etc.)? Homocysteine-lowering interventions failed and MR studies dont look great, so even if my homocysteine is high (I’ll do my test next week) I’m not sure I’ll start supplementing in B9 & B12. I’m now trying to only take drugs and supplements if highly safe and effective (with measurable outcomes). For instance, drugs to lower BP & BPV (with ARB + D-CCB + thiazide-like) and to improve insulin sensitivity (with SGLT2i, acarbose and maybe GLP-1RA) meet these criteria for me.
2 Likes
At least in the US very easy, Quest and Labcorp both offer them and one can order it oneself without a doctor via services like ULTA labs for about 40 dollars for a package with both of them after their almost universal 20% off discount.
See ADMA/SDMA | Ulta Lab Tests and/or Quest Diagnostics: Test Directory and ADMA/SDMA | LABCORP OKLAHOMA, INC. | Test Directory
My framework is similar, but I’d frame it more as “effectiveness-to-safety” ratio. If the safety of a intervention is very high (like adding some non crazy amounts of B6, B9 and B12 and/or some creatine) then it’s ok for me that there is less certainty about the effectiveness in cases where the effectiveness could be very, very valuable (neurological and cardiovascular health in this case).
Think in contexts where there are no patents like for vitamins like B6, 9 and 12 we are naturally not going to have as much clinical trial data, so that has to be weighed too.
The rationale and mechanistic understanding is also something that matters in my framework. Perhaps listen to the DRIVE episodes where it’s discussed to help build out some intuitions / questions re what to look into further.
2 Likes
This was my framework as well before. I changed my mind as I’m looking for treatments to continue until the end of my life. Unfortunately as you noted data on vitamins isn’t as good as data on patented drugs (although you can patent some formulations, see for instance Deplin and medical foods). This means that we have less data on their safety and effectiveness. It’s sad because I’m sure some supplements are as safe and effective as some drugs. But I apply the same criteria to evaluate supplements, drugs and devices. I see no reason to lower the bar for some compounds because of the lack of a legal framework to support R&D around these therapies. That being said, despite the lack of patentability for vitamins (and for repurposed generics like rapamycin!) there are hundred of animal studies and trials (often under powered…) studying them.
Mendelian randomization studies are also extremely cheap and they’re super valuable for stuff like vitamin levels. Homocysteine lowering is useless according to MR. Do we have MR for SDMA and ADMA activity and longevity?
I don’t believe in mechanistic understanding alone. Because we know so little. Mechanistic assumptions have to be backed by at least animal studies and/or clinical trials and/or emulated trials (leveraging longitudinal data) and/or Mendelian randomization.
7 Likes
Creatine might help if so because I think it is one of the most studied supplements in the world with other possible benefits as well like for muscle strength and cognition.
2 Likes
But where do we draw the line? Should we only make decisions about what foods to eat and what foods to not eat, how much food to eat, how to optimize sleep, what exercise to do and not and methods for managing stress and mental wellbeing based on only on clinical trials? Clearly most of us think it is better to make decisions on those types of things even when there is no data.
And re medications, everything a person combines two or more medications that have not been tested together he or she is no-longer in the world of clinical trials because the very large risks of interactions and polypharmacy. So if you are combining more than two drugs that have not been tested in clinical trials you are somehow using other frameworks for your decision making (whether explicitly or (less good) implicit) - I think that is the case right?
It’s probably better to make decisions for the next 6-12 months at a time and then keep updating the decisions along the way as more and better info comes out. So the decision for me in this context on whether a bit of B-vitamins and some creatine knocks down my homocysteine in a bit way, is whether it is worth doing that for the next 6-12 months and not for the rest of my life, so go another 6-12 months and then both see where my individual measured b-vitamin levels come out and my homocysteine (and SDMA and ADMA come out) and how I feel. And also keep looking at what we learn datawise and then combine that info and update my decisions for the next 6-12 month period or so.
2 Likes
To each their own way! We have a lot of data on diet and sleep. I don’t want to review everything every 6 months. I already do a lot of monitoring (every morning I check Google Scholar actually ![]() ). Anyway in the specific case of homocysteine-lowering: clinical trials and MR studies point to its uselessness so I see no reason to do it. Still, it’s a risk factor, so it’s good to know it. (And raised homocysteine might be a symptom of something else, I’d like to act on that, if only I could find it!)
). Anyway in the specific case of homocysteine-lowering: clinical trials and MR studies point to its uselessness so I see no reason to do it. Still, it’s a risk factor, so it’s good to know it. (And raised homocysteine might be a symptom of something else, I’d like to act on that, if only I could find it!)
2 Likes
Still, there’s no harm in supplementing with the b vitamins and tmg.
- How do we know that long-term? Under which dose? Which form of these vitamins? I remember reading somewhere that B12 as cobalamin could be bad for renal function for instance (not 100% sure, I could make this up). [EDIT: it’s actually cyanocobalamin that is harmful in people with low eGFR: B vitamin therapy for homocysteine: renal function and vitamin B12 determine cardiovascular outcomes - PubMed It just shows that the safety profile of these vitamins is not that simple.]
- I think that some vitamins like this could be useful. But not for their homocysteine-lowering properties (as homocysteine-lowering is useless): they also act on other pathways. B12 as methylcobalamin seems especially interesting.
Of course. Just trying to share some issues that I saw in the logic. No need to discuss further.
Look at the Mendelian randomization studies. Genetically high homocysteine is different than homocysteine from other causes, and directly reducing homocysteine via betaine may not have the effect as going after the more upstream factors (some which are really tough)
B vitamins don’t reduce my homocysteine, which is sad. But maybe I can try betaine and see how it goes
2 Likes