I just noticed that "Food slightly reduces the bioavailability of telmisartan, with a reduction in the area under the plasma concentration-time curve (AUC) of about 6% with the 40 mg tablet and about 20% after a 160 mg dose" (per FDA). 6% is not a massive difference, but I was taking telmisartan 40 mg just before my meals; from now I’ll try to take it two hours after dinner to maximize absorption.
4 Likes
Telmisartan (TMN), an angiotensin receptor blocker (ARB) drug, is being considered as an alternative therapy for Alzheimer’s disease (ALZ). However, when taken orally, its low water solubility leads to a low bioavailability and brain concentration. To overcome this problem, TMN was formulated as nanocrystals (NC), then incorporated into dissolving microneedles (DMN) to enhance drug delivery to the brain via the trigeminal route on the face.
3 Likes
So We can do it internasally for the brain ?
This is just a research paper. I don’t know whether intranasal telmisartan is safe or not.
1 Like
Just published: Homocysteine: a futile comeback or a promising tool for the risk assessment of hypertensive patients? 2024
Nevertheless, some questions remain unsolved and require further research in our view:
- What is the contribution of Hcy in the global cardiovascular risk (fraction of attributable risk of Hcy), and is it worth to add this variable in the pre-existing CVR calculators?
- How to manage the factors influencing Hcy levels in the long term?
- Are the findings replicable in other CV diseases and other populations?
Further research seems warranted to close the current debates and precise the place of Hcy in the CVR assessment.
The above article is a comment on: Homocysteine, hyperhomocysteinemia, and H-type hypertension 2024
Generally, a plasma Hcy level higher than 10 or 15 μmol/L has been defined as hyperhomocysteinemia (HHcy). An individual with essential hypertension complicated with HHcy is considered to have H-type hypertension (HTH). Currently, HHcy is considered a novel independent risk factor for various cardiovascular diseases.
Another paper suggests that ARBs (e.g. telmisartan) are the best antihypertensive drug for people with HHcy: Homocysteine predicts vascular target organ damage in hypertension and may serve as guidance for first-line antihypertensive therapy 2021
From a clinical perspective, Hcy levels could therefore not only represent a useful marker of arterial HMOD but also potentially serve to guide the choice of the most appropriate first-line RAAS blocking antihypertensive regimen, that is, ACEi or ARB, the latter being the preferred choice in the context of elevated Hcy levels above 10 µmol/L. Clearly, future studies are needed to investigate whether indeed these theoretical considerations hold true in prospective longitudinal studies and whether Hcy levels may influence the potency of antihypertensive therapy with ACEi vs ARBs in regard to lowering BP and preventing HMOD.
7 Likes
I was excited about the homocysteine theory, so I bought the article. It’s garbage. (No comment on the fact that it comes from the 3rd poorest Chinese province…) It concludes that “Moreover, the curative effect may be improved if traditional Chinese medicine can be administered at the same time.” based on “Compound prescriptions such as Huanglian Wendan Decoction or Erchen Decoction, Shenxiong Glucose, Compound Danshen Dropping Pills, Breviscapine and Banxia Baizhu Tianma Decoction, Tianma Gouteng Decoction, and Qiju Dihuang Pill have certain effects on controlling BP and lowering Hcy levels.” The paper also says that “cholesterol decreasing or lipid-lowering drugs” increase Hcy levels but somehow “atorvastatin calcium tablets” decrease it. Of course, they don’t cite sources, nor do they explain the contradiction.
Worse: they mostly cite literature confirming their thesis and they don’t mention that most Mendelian randomization studies and meta-reviews of clinical trials did not find a significant causal effect of homocysteine-lowering interventions for BP:
- Effect of vitamin B2, vitamin C, vitamin D, vitamin E and folic acid in adults with essential hypertension: a systematic review and network meta-analysis 2024: “Among the five vitamins, only vitamin E was significantly more effective at reducing SBP (mean difference: −14.14 mm Hg, 95% credible intervals: −27.62 to –0.88) than placebo. In addition, no evidence was found that any of the five vitamins influenced DBP, 24 hours SBP, 24 hours DBP, or HR.”
- Phenome-wide association study of genetically predicted B vitamins and homocysteine biomarkers with multiple health and disease outcomes: analysis of the UK Biobank 2023: they didn’t find a causal link between high Hcy and hypertension
- 1 mmHg of reduction… wow…
 Folic acid supplementation and blood pressure: a GRADE-assessed systematic review and dose-response meta-analysis of 41,633 participants 2021: “The pooled results of 22 studies, including 41,633 participants, showed that folic acid supplementation significantly decreased systolic BP (SBP) (WMD: −1.10 mmHg; 95% CI: −1.93 to −0.28; p = 0.008).
Folic acid supplementation and blood pressure: a GRADE-assessed systematic review and dose-response meta-analysis of 41,633 participants 2021: “The pooled results of 22 studies, including 41,633 participants, showed that folic acid supplementation significantly decreased systolic BP (SBP) (WMD: −1.10 mmHg; 95% CI: −1.93 to −0.28; p = 0.008). - Blood Pressure Variability in CKD: Treatable or Hypertension’s Homocysteine? 2019: “The once promising ability to reduce elevated serum homocysteine levels did not prove, for example, to lessen the risk of cardiovascular outcomes aside from stroke.”
- Is there a causal role for homocysteine concentration in blood pressure? A Mendelian randomization study 2016: “Overall, the present findings do not corroborate the hypothesis that homocysteine has a causal role in blood pressure, especially in SBP.”
- Here as well, tiny effect: High-dose folic acid supplementation effects on endothelial function and blood pressure in hypertensive patients: a meta-analysis of randomized controlled clinical trials 2009: “The pooled estimate of effect of folic acid supplementation on systolic and diastolic blood pressure was −2.03 mm Hg (95% confidence interval [CI], −3.63 to −0.43; P = .04) and 0.01 mm Hg (95% CI, −1.12 to 1.13; not significant), respectively.”
Even this paper does not conclude this but: “As such, the debate as to the causal link between hyperhomocysteinemia and hypertension continues.”
So does it mean the Hcy hypothesis for hypertension should go to the trash? Probably, until we have more data.
4 Likes
I think the combination of telmisartan with an SGLT2 Inhibitor is no-brainer for anyone that wants maximum benefits from this wonderful molecules
5 Likes
Yes the ARB/ACEI + SGLT2i combination seems safe and effective, here are papers published this year:
- ASSOCIATION BETWEEN USE OF SGLT2 INHIBITORS COMBINED WITH RENIN-ANGIOTENSIN ANTAGONISTS AND OUTCOMES FOR HEART FAILURE
- Assessment of effects of combination of SGLT2 inhibitors and renin–angiotensin–aldosterone system blockers on the renal functions of patients of diabetic kidney disease (SGRASS-DKD study)
- Combining renin-angiotensin system blockade and sodium-glucose cotransporter-2 inhibition in experimental diabetes results in synergistic beneficial effects
- Combination Therapy of RAS Inhibition and SGLT2 Inhibitors Decreases Levels of Endotrophin in Persons with Type 2 Diabetes
5 Likes
Catching up on old posts. I do like that it lowers resting heart rate, so it might be better for peple who need to reduce that, but otherwise you make a convincing case that it’s not as good as the others mentioned.
1 Like
BP = SV x HR x SVR
SV = Stroke volume
HR = Heart rate
SVR = Systemic vascular resistance
Beta blockers primarily act on BP via a reduced heart rate. Other anti hypertensive work on other parts of the equation. Amlodipine might increase a bit the HR so there might be a place for a beta blocker in addition to telmisartan, amlodipine and indapamide SR as an ultra low dose quadruple combination. Indeed, this paper published a few days ago makes the case for such combinations and notes the potential synergies between beta blockers and CCBs and ACEIs/ARBs: β-blockers are not all the same: pharmacologic similarities and differences, potential combinations and clinical implications 2024
However, the authors argue that bisoprolol is the best beta blocker based on clinical trials and pharmacokinetics. It seems that nebivolol hasn’t been studied enough to recommend it and suffers from great variability between individuals.
It turns out that in the two QUARTET trials they used bisoprolol (+ ARB + amlodipine + indapamide): Rilmenidine vs Telmisartan or other BP meds for Longevity - #63 by adssx
2 Likes
Is the response to antihypertensive drugs heterogeneous? Rationale for personalized approach 2024
The Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) 2019, which estimated the proportion of mortality, years of life lost, and years of life lived with disability attributable to 87 behavioural, environmental, occupational, and metabolic risk factors, highlighted how the predominant share of deaths in the world is attributable to systolic BP values ≥ 110–115 mmHg with an estimate of 10.8 million avoidable deaths every year and 235 million years of life lost or lived with disability every year.
Furthermore, the combination of drugs that act on different mechanisms involved in the rise in BP values reduces the variability of the BP response to treatment and allows for a faster BP response to be obtained than that which can be obtained with increasing doses of a single drug and it is safe and well tolerated with a modest risk of hypotensive episodes, even when prescribed to patients with grade 1 hypertension.
The finding of a substantial heterogeneity in the individual response to the different treatments used in the PHYSYC study suggests the possibility of obtaining additional advantages with a personalization of the treatment, but in the current state of knowledge, this eventuality still appears rather theoretical, especially due to the difficulties in making personalized choices. Following the approach used in the PHYSIC study, one could hypothesize testing the patient’s individual response to a series of short periods of treatment before defining long-term therapy with one or more drugs, but this approach appears quite laborious.
Theoretically, it would be simpler to identify phenotypic characteristics that can predict a satisfactory response to a drug or a combination of drugs. Indeed, beyond the long-known modest sensitivity of black hypertensive patients to treatment with ACE-I, the limited availability to date of phenotypic indicators of response to a drug makes this approach difficult to pursue.
The progressive digitalization of healthcare systems is making enormous quantities of data available for machine learning systems which will allow the derivation of management algorithms for truly personalized antihypertensive therapy in the near future.
In the meantime, I guess the best approach is trial and error and/or a low-dose combination of the best-in-class agents (so telmisartan, amlodipine, indapamide SR, and bisoprolol?).
Provisionally accepted paper, we don’t have the full text yet: Association between types of antihypertensive medication and the risk of atrial fibrillation: A nationwide population study 2024
In monotherapy, ACEi and CCB had similar AF risks as ARB, while beta-blockers and diuretics showed higher AF risks than ARB. In combination therapy, ARBs/CCBs and ARBs/diuretics had the lowest AF risk, whereas ARBs/beta-blockers had the highest compared to ARB/CCB. Among the specific ARBs, the AF risk varied insignificantly, except for telmisartan and candesartan. In hypertensive patients receiving monotherapy, ACEi and CCB showed a similar AF risk as ARBs, while beta-blockers and diuretics were associated with a higher risk.Among those receiving combination therapy, ARBs/CCBs and ARBs/diuretics had the lowest AF risk, whereas ARBs/beta-blockers showed the highest risk. Various types of ARBs have different associations with AF risk.
2 Likes
So we’ve got nothing for now to tell us if they mean worse vs better?
I’ve been tapering off my nebivolol as I gradually increase telmisartan dose, so far BP is great (115/75) at 40mg tm, 2.5mg nb. Looks like I’m on the right track but that eventually adding in amlodipine might help further reduce future afib risk.
I tried to get dapagliflozin from India this time instead of empa (since I believe a study you posted a while ago showed decreased afib risk with dapagliflozin but not empa), but I prefer branded meds when ordering from India and was told that the manufacturer of Farxiga no longer allows sale in India😒
BTW I really appreciate the literature searches you do! I need to up my lit search skills.
3 Likes
Yes it’s a bit sad the summary doesn’t give that essential information ![]() We’ll see when we have the full text… But I’m not sure it’s a great paper tbh (given the journal + institutions).
We’ll see when we have the full text… But I’m not sure it’s a great paper tbh (given the journal + institutions).
1 Like
Besides bisoprolol, carvedilol seems interesting, although it has a shorter half-life (6h) and therefore needs to be taken twice a day (vs once daily for bisoprolol). But it has interesting additional properties:
An Updated Prioritization of Geroscience- Guided FDA-Approved Drugs Repurposed to Target Aging 2024
One study found that the beta blocker carvedilol reduced oxidative stress-induced apoptosis in cardiomyocytes (see Supplement 1).
One meta-analysis of interventional trials reported carvedilol, a non-selective beta-blocker, to decrease mortality significantly more than beta-1 selective beta blockers in patients with either heart failure or myocardial infarction.
Today, four β-blockers are recommended for the treatment of HF (bisoprolol, carvedilol, metoprolol succinate (CR/XL) and nebivolol) in the European Guidelines.
Carvedilol-induced β1AR-Gi signaling also addresses the PI3K/Akt pathway and induces NOS3 activation, thereby promoting cardiomyocyte survival.
Carvedilol induces vasodilation via antagonism at peripheral α1AR inducing arterial vasodilation while concurrently suppressing reflex tachycardia via cardiac β1AR-blockade.
Carvedilol and its metabolites have anti-oxidative properties that manifest as antioxidation (e.g. reduced lipid peroxidation) and anti-inflammation. These capabilities are attributed to the chemical structure of carvedilol and its metabolites, which have a tricyclic carbazole structure.
Carvedilol – via the PKA/PGC1α pathway – leads to improved mitochondrial function in endothelial cells, resulting in protective/beneficial effects within the context of atherosclerosis.
Additionally, carvedilol - likely via modulation of potassium channels - stabilizes glucose homeostasis and attenuates hepatic glucose production, while enhancing muscular insulin signaling. Consistent with these observations, carvedilol has shown favorable in the context of metabolic disturbances in patients.
In Association of cardiovascular disease management drugs with Lewy body dementia: a case–control study 2023, the HR of carvedilol use with LBD was 0.67 [0.65-0.69], the best-performing beta-blocker and as good as telmisartan (but it’s an association study, not an RCT).
On the other hand, in the EPITERNA preprint, carvedilol was associated with a significantly shorter lifespan and was the worst-performing beta-blocker (again, association study).
In animal and computational models, it seems neuroprotective:
- Identification of Azelastine and Carvedilol as Cholinesterase Inhibitors via Structure-Based Virtual Screening of FDA-approved Drugs 2023
- Neuroprotective repositioning and anti-tau effect of carvedilol on rotenone induced neurotoxicity in rats: Insights from an insilico& in vivo anti-Parkinson’s disease study 2022
And there are three ongoing studies of carvedilol in NDDs:
- Cardiac Changes in Early Parkinson’s Disease: A Follow up Study (NCT04218968): “Twice daily oral doses of adrenergic blocker 12.5 mg or 25mg, according to patient tolerability.” => Ends in Dec 2025
- Adrenergic Blockers for Cardiac Changes in Early Parkinson’s Disease (Protocol 53136): “target dose will be 25mg twice daily” => Ends in Aug 2024
- Data Analysis for Drug Repurposing for Effective Alzheimer’s Medicines (DREAM)- Propranolol/Carvedilol Versus Atenolol/Bisoprolol/Sotalol (NCT05794997) => Ended in Dec 2023?
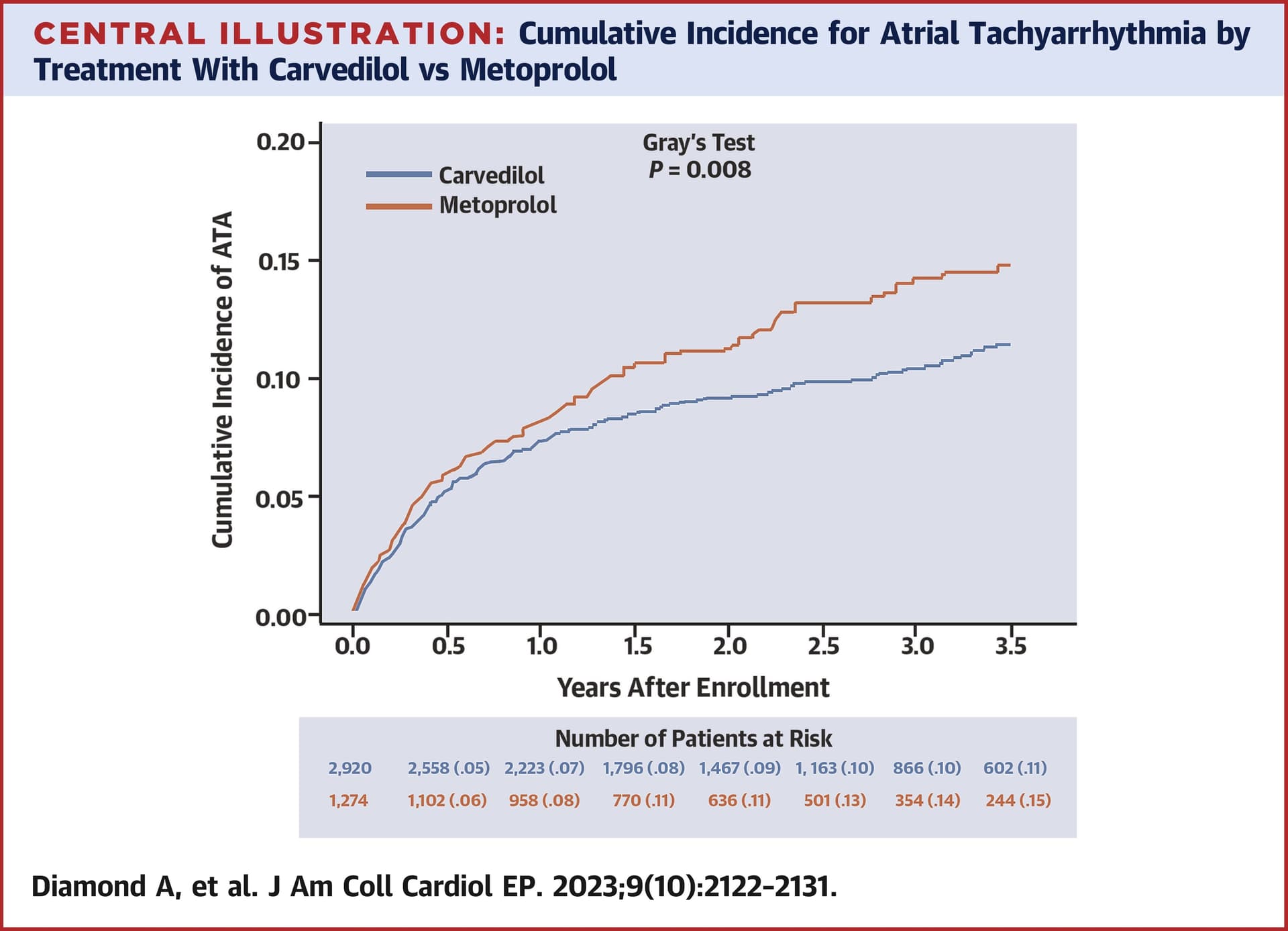
Carvedilol is better than metoprolol for arrhythmias: Effect of Carvedilol vs Metoprolol on Atrial and Ventricular Arrhythmias Among Implantable Cardioverter-Defibrillator Recipients 2023
It also works well in atrial fibrillation:
- Which should you choose for post operative atrial fibrillation, carvedilol or metoprolol? A systemic review and meta-analysis 2024
- Efficacy and safety of once-daily carvedilol in atrial fibrillation patients: a randomized, double-blind, placebo-controlled trial 2024
So, if someone needs a BB (for instance to lower HR), then carvedilol might be the best option. What do you think @Davin8r?
However here carvedilol, although the best performing beta-blocker, ranks below placebo (not sure it’s a great paper though): EFFECT OF ANTIHYPERTENSIVE AGENTS ON RISK OF NEW-ONSET AND RECURRENT ATRIAL FIBRILLATION: A NETWORK META-ANALYSIS OF RANDOMIZED CONTROLLED TRIALS 2024
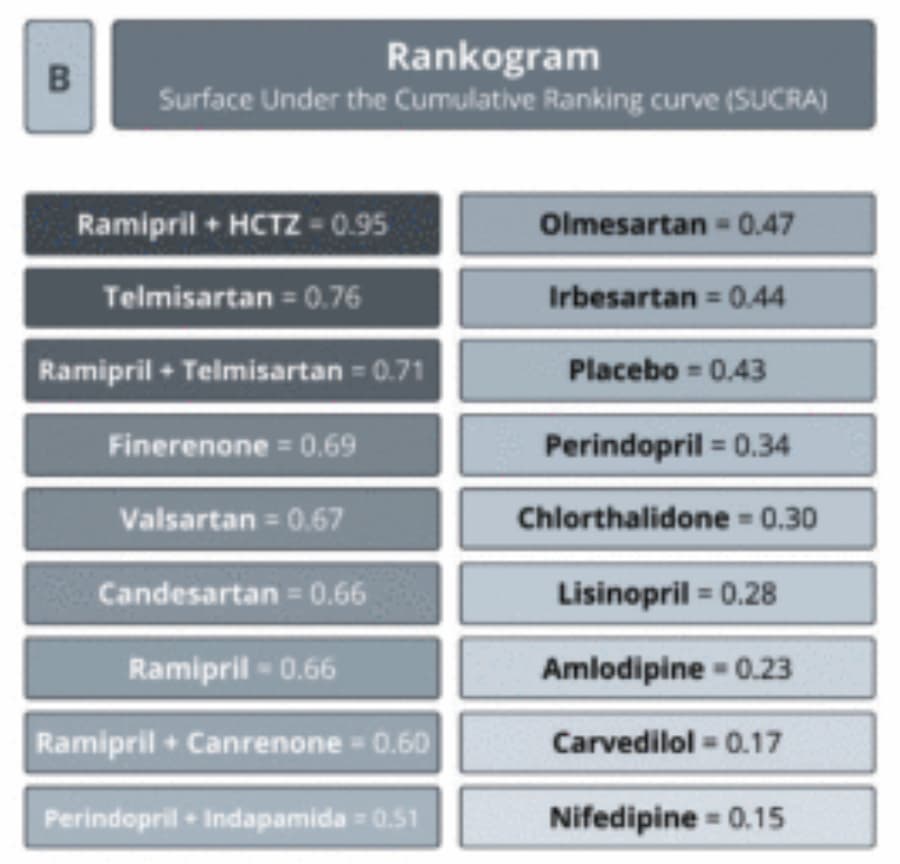
Ramipril + HCTZ is the best combination to reduce the risk of new-onset and recurrent AF among patients with hypertension, diabetes, or AF. However, not all combinations were tested (due to a lack of trials). Telmisartan was the best-performing single agent. As ramipril + HCTZ = 0.95 vs 0.66 for ramipril and perindopril + indapamide = 0.51 vs 0.34 for perindopril, I can imagine that telmisartan + indapamide would be even better than ramipril + HCTZ.
2 Likes
Carvedilol and nebivolol have always been the two “different” beta-blockers that stood out from the others. I did lit reviews on them about 15 years ago to help determine which one I wanted to try, also tried both of them. Since nebivolol gave me zero side effects while carvedilol made me tired and gave me a headache, I went with nebivolol.
Based on your updated lit search, carvedilol certainly has potential, but yes those studies on afib do seem contradictory. The last one seems the most applicable for afib in particular to the general population of people with afib, since the previous studies you mentioned were under more specific conditions (post surgical patients, patients with implantable defibrillators). One of the studies you mentioned only showed that carvedilol effectively helped control heart rate during afib and didn’t address afib prevention.
So I’m still aiming to completely get off nebivolol and control BP with telmisartan alone (along with empagliflozin as my “diuretic”), which hopefully also will decrease future risk of afib.
1 Like
Empagliflozin is NOT a diuretic, see the recent: SGLT2 Inhibition: Neither a Diuretic nor a Natriuretic commenting on Water Conservation Overrides Osmotic Diuresis During SGLT2 Inhibition in Patients With Heart Failure.
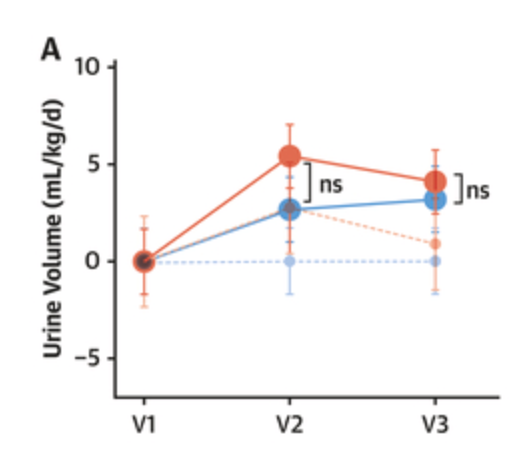
Many investigators attribute the beneficial effects of SGLT2i to the drugs’ natriuretic diuretic or osmotic diuretic effects. The underlying assumption is that, similar to diuretics, SGLT2i increase urine volume and thereby exert beneficial effects on cardiac workload and myocardial energy expenditure, especially in states of cardiac congestion. However, the effects of SGLT2i on solute-driven urine volume formation are different from those of traditional diuretics. The observed natriuretic, osmotic diuretic effects of SGLT2i are often short-lasting, modest, or absent. Retrospective analysis of the currently available data suggests that SGLT2 inhibition does not produce durable decongestion.
Despite the significant early and persistent increase in urine solutes (Figure 3A) and glucose (Figure 3D) excretion, treatment with dapagliflozin resulted in a statistically nonsignificant early increase in urine volume (mean difference 2.8 mL/kg/d; 95% CI: −1.97 to 7.48; P = 0.25), which diminished after 4 weeks (0.9 mL/kg/d; 95% CI: −3.83 to 5.62; P = 0.7)
These findings suggest that SGLT2i may not improve cardiac health status by osmotic diuretic decongestion. An alternative “nutrient deprivation signaling/autophagy hypothesis” assigns the beneficial effects of SGLT2i to reprogramming of mitochondrial function. Similar switches in mitochondrial fuel utilization occur in “aestivation,” an evolutionary conserved survival strategy in response to combined energy and water deficit.The observed ≈150 kcal/d loss of glucose fuel into the urine (Figure 3D) not only requires adaptive energy conservation to prevent an energy deficit but also triggers physiological water conservation to counteract the osmotic diuretic effect of glucosuria and prevent dehydration (Figure 4C). As an extension to the “nutrient deprivation signaling/autophagy hypothesis,” we suggest that SGLT2 inhibition may result in a biomimicry of aestivation metabolism and thereby improve health span.
4 Likes
Sorry, I meant to put “diuretic” in quotes. Empagliflozin as a replacement for a diuretic BP med to hopefully reduce risk of afib and help to keep BP under control.
Yes, but I don’t know if SGLT2i can replace a diuretic BP med: “In normotensive, nonobese individuals, SGLTi-induced changes in BP and weight are minimal to absent.” ( https://www.sciencedirect.com/science/article/pii/S0033062023001068?via%3Dihub#bb0050 )
Ok but I’m not normotensive without meds, which is why I’m taking BP meds ![]()
Ah OK. What’s your BP without meds?