Why? I skimmed through Dr. Joshua Miller’s video and didn’t see anything about riboflavin (B2). On the other hand, there’s a growing body of evidence pointing to potential benefits: Riboflavin and Neurocognitive Decline
Riboflavin (B2) is rarely tested. B2 deficiency seems common among individuals homozygous for the methylenetetrahydrofolate reductase (MTHFR ) 677C→T (TT): Your “MTHFR” Is Just a Riboflavin Deficiency 2019 (is this a good source?)
So, I guess if you have high homocysteine, test for B2, B6, B9, and B12 and check your genes (MTHFR), see which vitamins are low, and supplement accordingly to get them to the optimal level. Homocysteine will be lowerered as a result. The absence of such an individualized approach in homocysteine-lowering trials might explain the inconclusive results: for instance, if someone has high homocysteine due to low B2, giving them high-dose B9 might not help or even be detrimental? And vice-versa?
Yes, the cheap approach that yields junk results seems common, because it is easy to data mine. There needs to be an actual study where levels are tested, and individuals are supplemented and show on retest therapeutic levels, then compare them to a placebo group with similar risks (e.g. homocysteine elevated or MTHFR mutation and homocysteine elevated.
Without doing this there is so much noise that one cannot show benefit, when there is likely benefit.
Association between riboflavin intake and the risk of all-cause mortality of patients with chronic kidney disease: A retrospective cohort study 2024: “After excluding potential confounders, lower intake of riboflavin was associated with the higher risk of all-cause mortality (Q1: HR = 1.33, 95% CI: 1.05–1.69). The similar association was also found in patients at mild/moderate stage (HR = 1.32, 95% CI: 1.05–1.66), in female (HR = 1.35, 95% CI: 1.01–1.81), with hypertension (HR = 1.37, 95% CI: 1.07–1.75), CVD (HR = 1.48, 95% CI: 1.08–2.03), and dyslipidemia (HR = 1.29, 95% CI: 1.01–1.66).”
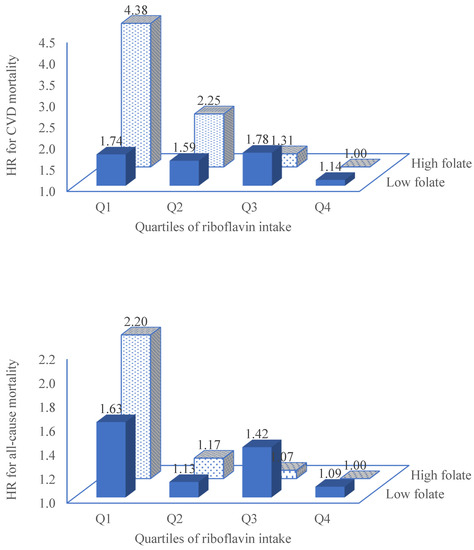
Riboflavin intake associated with decreased risk of all-cause mortality among adults attending NHANES 2005-2016 2023: “High intake of riboflavin was associated with a lower risk of all-cause mortality, and CVD mortality. In multivariable model adjusted for sociodemographic factors, lifestyle factors and chronic conditions, across the quartiles of riboflavin intake, the hazard ratios (HRs) [95% CI] for CVD mortality were: 1.00, 0.92 [0.63, 1.35], 0.79 [0.49, 1.26], 0.52 [0.30, 0.90] (p trend 0.027), respectively. The corresponding figures for all-cause mortality were: 1.00, 0.69 [0.55, 0.87], 0.74 [0.58, 0.94] and 0.62 [0.48, 0.80], respectively. The protective association between riboflavin intake and CVD mortality was further strengthened among those with a high intake of folate (quartiles 3 and 4) with HRs of 1.00, 0.49 [0.21, 1.12], 0.25 [0.10, 0.63] and 0.19 [0.08, 0.47] across quartiles of riboflavin intake (p for interaction 0.039). In conclusion, riboflavin intake was inversely associated with all-cause mortality, particularly CVD mortality. Riboflavin and folate synergistically decreased the risk of CVD mortality.”
Good question. I have wondered why homocysteine lowering therapies don’t show clear benefits in clinical trials, especially since I have seen evidence of homocysteine directly harming the vasculature rathern than just being a marker of poor health. The study below indicates that maybe it’s not serum levels that are most important but tissue-bound or intracellular levels of homocysteine. Maybe most homocysteine lowering interventions mainly lower it in the serum but not so much in tissues. I’m not sure, but it’s an interesting theory. Here are a few relevant quotes:
“studies in animals and in cell culture suggest that Hcy has a vast array of toxic effects on the vasculature, with demonstrated roles in endothelial dysfunction, medial remodeling and adventitial inflammation. It is hypothesized that rather than serum Hcy, tissue-bound Hcy and the incorporation of Hcy into proteins could underlie the toxic effects of Hcy on the vasculature.”
" although B-vitamin supplementation successfully decreases serum Hcy concentrations, it is unknown whether it has the ability to decrease tissue-bound or intracellular Hcy. Current evidence suggests that Hcy elicits its negative effects directly in the vessel wall by inducing modifications to vascular cell function, and by irreversibly incorporating into cellular and extracellular matrix proteins (Fig. 2). These pathological changes induced by Hcy would likely be unaffected by serum Hcy-lowering treatments."
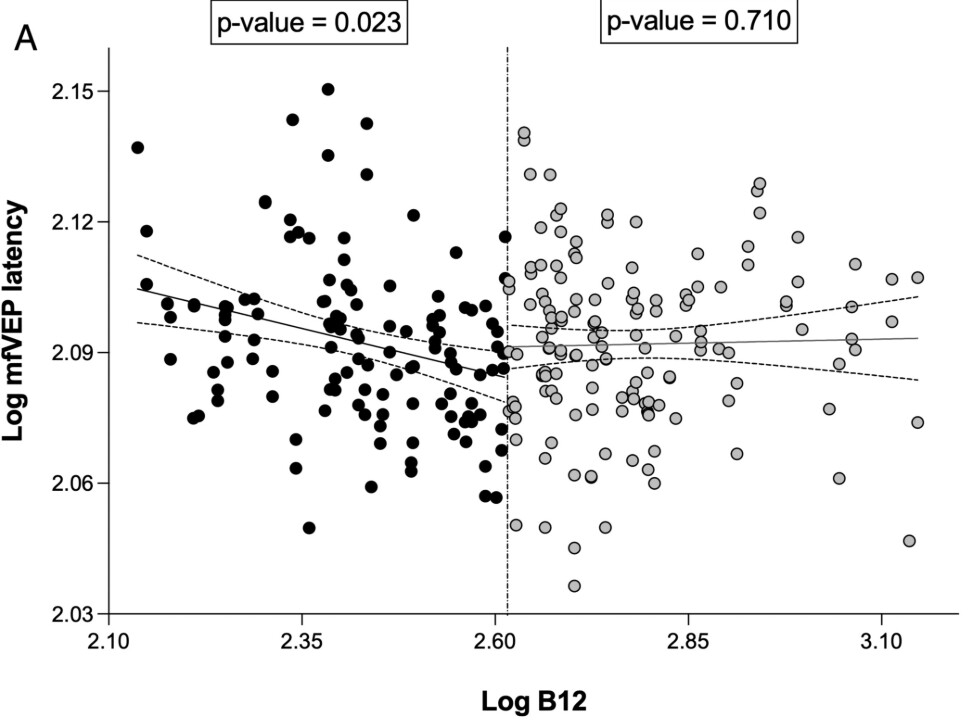
Therefore, and since we postulated that people at the lower ranges of B12 may show signs of abnormalities in their mfVEP recordings, we stratified the cohort for B12 levels above and below the mean (geometrical mean = 408 pmol/L). Albeit these B12 levels were considered normal, patients with lower levels of B12 showed a significant inverse association with mfVEP latency (estimate = −0.04; p = 0.023; Fig 2A) in a model correcting for age, sex at birth, CVRF, BMI, APOEε4 allele, HbA1C, and education. Thus, a measured total B12 below the mean, or below 408 pM, significantly associates with a delay in mfVEP latency, representing slower conductivity in the brain.
However, there might be an upper limit (unclear if causal or not or due to a high inactive B12 %):
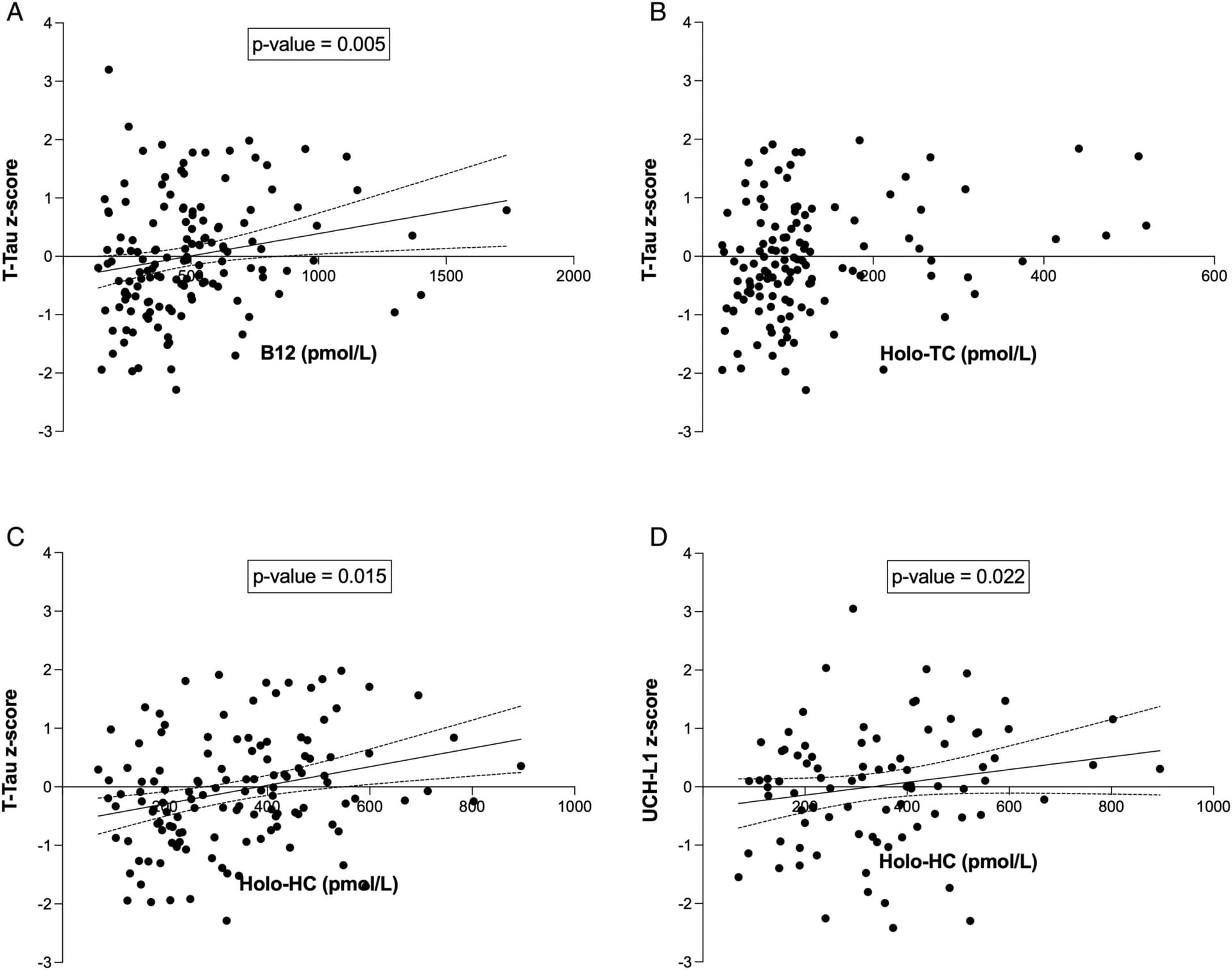
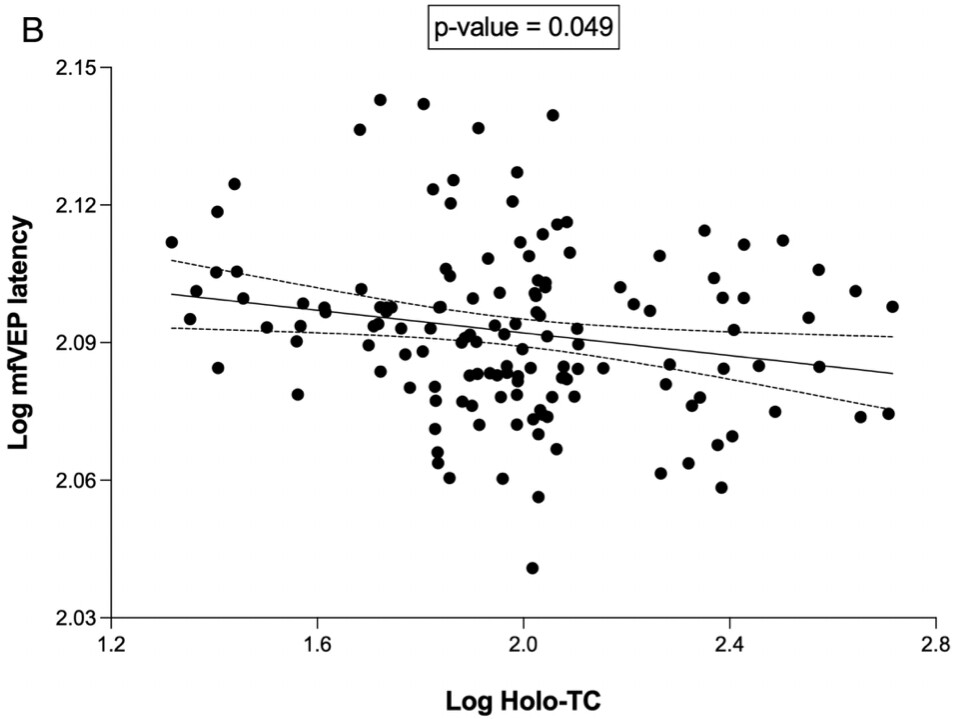
Surprisingly, in a linear regression model correcting for age, sex, BMI, CVRF, education, APOEε4 status, HbA1C, and creatinine, there was a positive association between Tau concentration (z-score adjusting for the factors stated above) and B12 (β = 0.25, p = 0.005, ΔR2 = 0.052, Fig 4A), but not any of the other biomarkers (Table 3). To further investigate this association between Tau and B12, we investigated the correlation between B12 levels and blood B12 components adjusting for the factors mentioned above. While no association could be found between Holo-TC and any of the included biomarkers (Fig 4B), Tau and UCHL-1 increased with higher Holo-HC (β = 0.22 and 0.28, p = 0.015 and 0.022, respectively, Fig 4C,D). Both associations remained significant after bootstrapping (p = 0.012 and 0.042 for Tau and UCHL-1, respectively).
MMA and HC can diagnose B12 deficiency despite normal B12 levels:
There are two enzymatic reactions that are dependent on vitamin B-12. Vitamin B-12 is required for methylmalonic acid (MMA) to be converted to succinyl-CoA, and in combination with folic acid, for homocysteine (HC) to be converted to methionine [9]. Therefore, MMA is clearly more specific to vitamin B-12 deficiency compared to HC. A deficiency of vitamin B-12 at the tissue level can lead to elevation of both MMA and HC [1] even when serum vitamin B-12 concentrations are within the reference values. Elevated MMA and HC levels together have been found to be 99.8% sensitive for diagnosing functional vitamin B-12 deficiency [10], which is defined as elevated MMA and HC levels despite normal vitamin B-12 levels in asymptomatic individuals [11–13]. Therefore, using serum vitamin B-12 testing alone may under-diagnose the deficiency of this vitamin.
MMA and HC have been identified as early markers of vitamin B-12 deficiency in different subjects such as general population [14], elderly [15–17], Asian Indians [18], infants [19], pregnant women [20], healthy women [21], type 2 diabetes [22], phenylketonuria [13] and renal insufficiency [12]
That paper is clearly competing with the Chinese ones to reach the lowest quality ever.
we compared a linear with a polynomial regression model. The polynomial model showed a better fit (R2 = 0.023) than the linear model (R 2 = 0.007), suggesting a non-linear association.
I mean seriously? Their models have an R-squared of 0.023 and 0.007, which basically means that there is no meaningful correlation between the model and the data, and they write a paper about it.
Their plots do show that and the funny (or sad) part is that they bravely plot the 95% confidence interval lines while it’s obvious that most of the data points are outside that interval. Look at that one for instance.
Yes, that’s a problem, but I wouldn’t discard it entirely. UCSF team publishing in the Annals of Neurology, so I give them the benefit of the doubt. I see that paper as a signal (you might say it’s just noise, and you might be right!). Would the trend be more evident with a larger cohort? Only 231 healthy elderly volunteers here, but it’s unlikely we would get all these biomarkers in a large cohort.
Just take it in reasonable step - unlike some other B vitamins - that you’d to large extent pee out if you have too much:
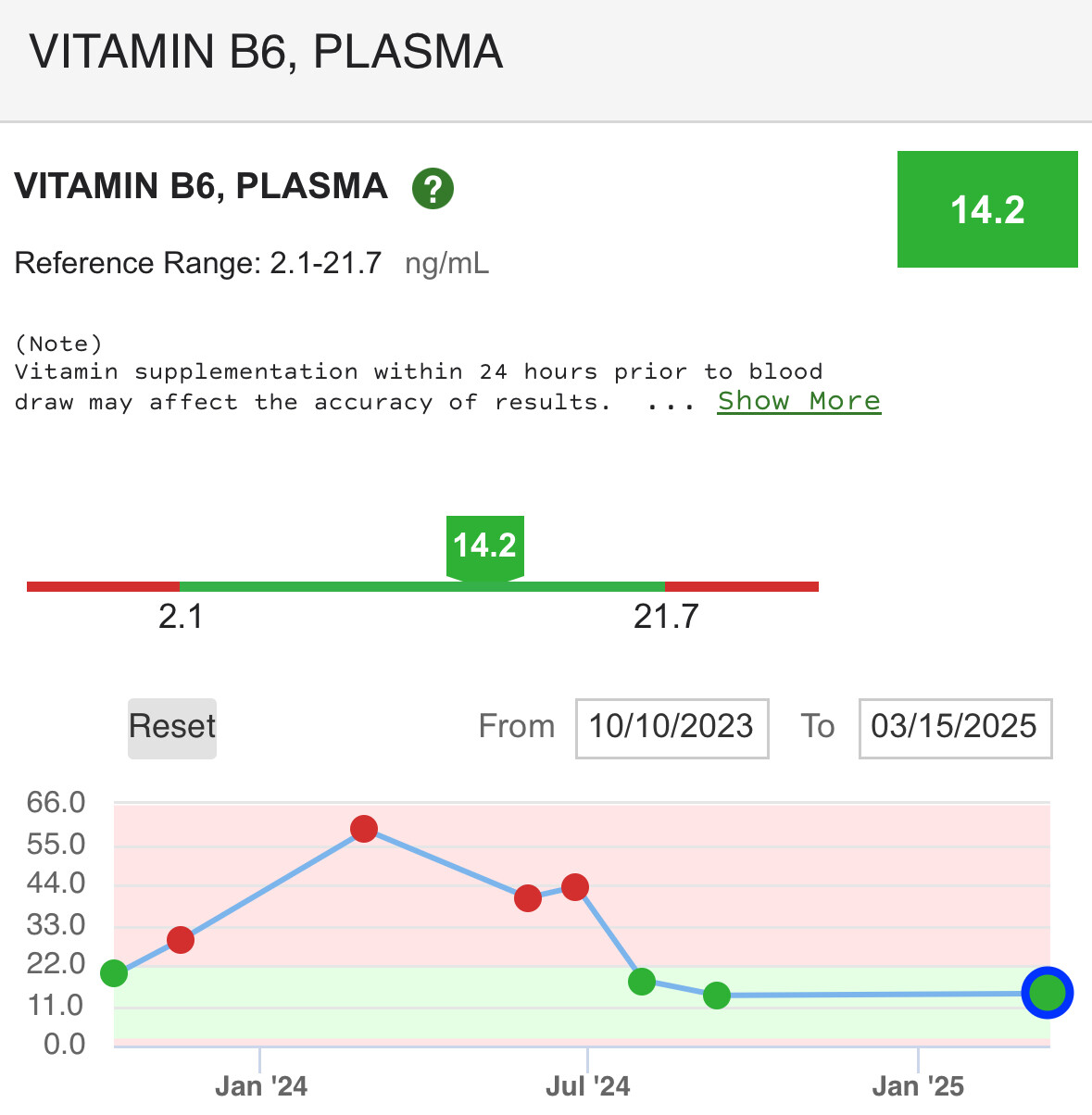
It’s possible to get too much vitamin B6, primarily from high-dose supplements. Excessive B6 intake, especially over extended periods, can lead to peripheral neuropathy, a condition causing nerve damage and symptoms like numbness, tingling, and burning in the extremities.
FWIW, my homocysteine has gone down from 10 mcmol/L where it’s been steady at that level for many years, to 7 mcmol/L in the year after I started taking TMG 1g/day. I don’t know if it was the TMG specifically, but that’s what I suspect (I also started supplementing with taurine daily at higher doses - for years it was 500mg/day - when my homocysteine was at 10 - to 3-4g/day in the last year or so).
Sorry P5P indeed (also called PLP). I think the issue isn’t the blood levels but others forms of B6 self inhibit themselves past a certain oral intake. Otherwise higher is better for B6 serum levels:
“In men, the multivariable hazard ratios (95% confidence intervals) for the highest versus lowest quintiles of folate and vitamin B6 were 0.77 (0.71–0.85) and 0.79 (0.71–0.86) for all-cause mortality, 0.59 (0.48–0.72) and 0.69 (0.56–0.85) for CVD mortality, and 0.68 (0.56–0.84) and 0.73 (0.60–0.90) for cancer mortality, respectively.”
But the B6 turnover might be more important than the B6 levels themselves and that is something that supplementation could not fix?
“Our study found that lower serum PLP levels were associated with increased risks of cardiovascular and all-cause mortality among the elderly population. And higher vitamin B6 turnover rate was associated with increased risks of cardiovascular, cancer, and all-cause mortality.”
I don’t take B6 / P5P but I bought the one you sent to give it a try at some point…
Ok, I don’t know enough, but would make sure to be confident that “ Excessive B6 intake, especially over extended periods, can lead to peripheral neuropathy” is not a risk
—-
Btw, did I recall you saying last year that folate may not be good to get too high? (Even if the all cause mortality above suggest that it might be good to have it relatively high)