A 2025 paper:
Inhibiting mechanotransduction prevents scarring and yields regeneration in a large animal model
A single local injection of verteporfin, an old macular-degeneration drug, at the moment of wounding stops scars from forming and instead regrows near-normal skin (hair follicles, fat, and proper collagen architecture) in the pig model that most closely mimics human scarring, with the same effect confirmed in grafted human skin and traced to a YAP/IL-33 signaling switch.
Almost every adult human wound heals by scarring. Scar tissue is a biological compromise: it closes the breach but cannot reproduce the strength, flexibility, hair, glands, or sensation of the skin it replaces, and there is still no approved drug that prevents it. A Stanford-led team has now taken a major step toward changing that.
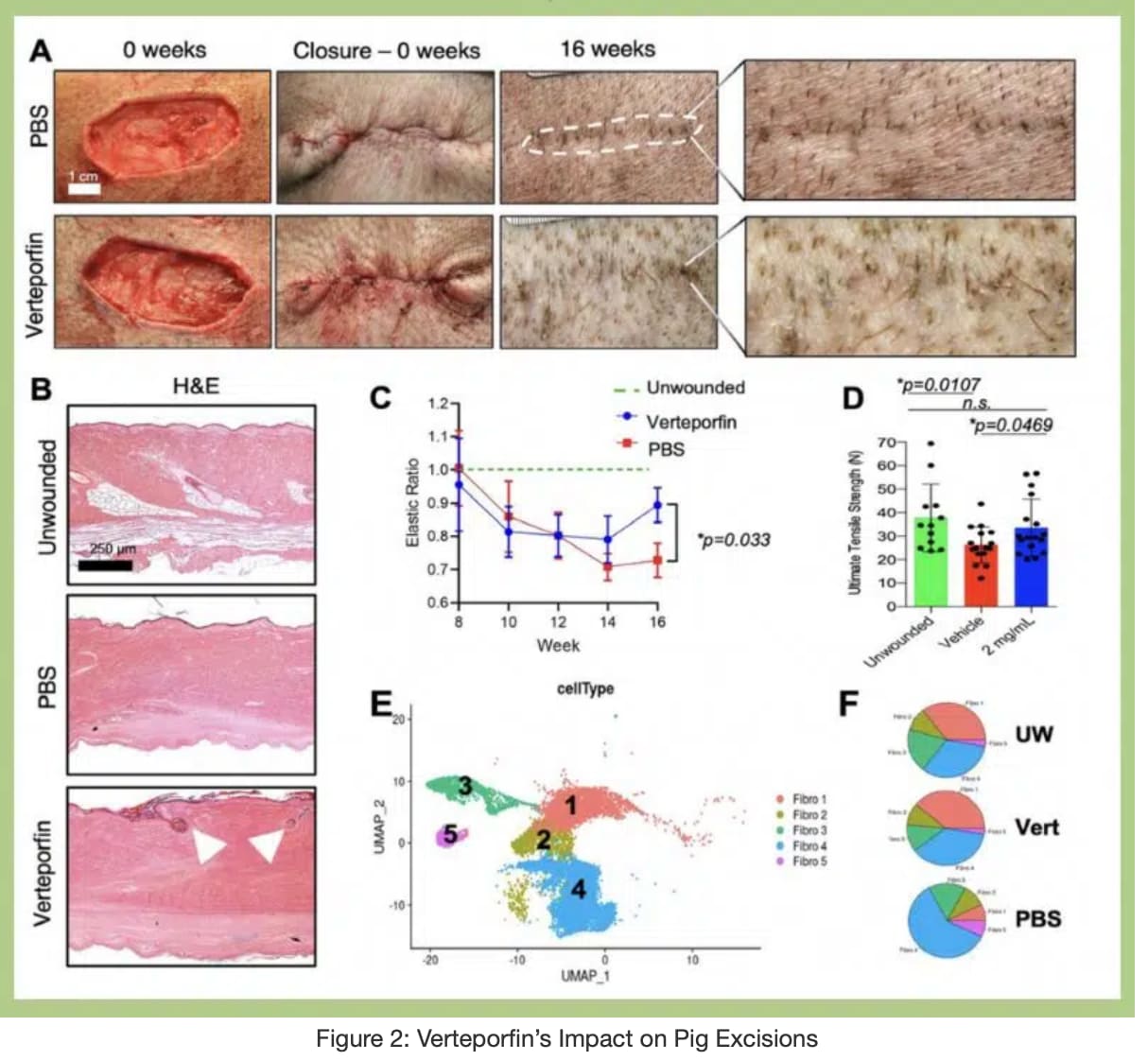
Building on earlier mouse work, the researchers tested verteporfin, a drug already approved for eye disease, in red Duroc pigs, widely regarded as the closest animal stand-in for human scarring because their skin is tight and high-tension like ours. A single injection into the wound edges at the time of surgery was enough. Sixteen weeks later, treated wounds showed almost no visible scar, regrew hair follicles and subcutaneous fat, and recovered the loose “basketweave” collagen pattern and mechanical properties of uninjured skin. Untreated wounds formed the expected dense, stiff, hairless scar.
The drug works by blocking YAP, a protein that translates the physical tension of a wound into a pro-scarring genetic program inside skin fibroblasts. Using single-cell sequencing of more than 75,000 cells plus spatial mapping, the team showed that verteporfin shifts the balance of fibroblast populations away from a scar-forming state and toward a regenerative one, and reroutes incoming immune cells away from fibrosis-promoting “fibrocytes” toward repair-type macrophages.
A striking mechanistic twist: the regenerative state depends on interleukin-33 (IL-33), an immune alarm signal. When the team blocked IL-33 in treated wounds, regeneration collapsed, and some wounds failed to heal at all. IL-33 appears to be a backup healing pathway that becomes essential once the normal tension-driven route is switched off.
Crucially, the effect held up in human skin grafted onto mice, and the relevant fibroblast populations were conserved between pig and human. Reassuringly, the locally injected drug barely entered the bloodstream and caused no detectable organ or skin toxicity.
The “big idea” is that scarring is not an inevitable feature of adult repair but a tension-driven choice that a single, well-timed drug dose can override, pushing the body toward regeneration. This pig and human-graft evidence is what de-risks the leap to people, and a first human trial has now begun.
Actionable Insights
This is a clinician-administered, injectable intervention delivered at the moment of wounding, using a drug that is not approved for scar prevention. Self-injection of verteporfin into wounds is not a supported protocol and is not advisable.
What is genuinely actionable is what to watch and how strong the signal is. The effect size is unusually large for a fibrosis intervention. On the 1 to 10 Visual Analog Scale (1 = severe scar, 10 = normal skin), treated wounds scored roughly 4 to 5 points higher than controls, about 45 to 55 percent of the entire usable scale, at every time point. Mechanically, treatment normalized both ultimate tensile strength and stiffness (Young’s modulus) back to unwounded-skin values, whereas scars are typically capped near 80 percent of normal strength while being abnormally stiff. In grafted human skin, collagen density in treated wounds fell back toward unwounded values, and vascularization (CD31) rose.
The practical watch-item: the same approach has now entered a Phase 2 human trial (SCARFREE-001), the first test of intradermal verteporfin for surgical-scar prevention. For anyone facing elective surgery in coming years, “ask whether a peri-incisional anti-fibrotic is available in trial settings” is the realistic near-term action, not anything to attempt independently.
Context
-
Open Access Paper: Inhibiting mechanotransduction prevents scarring and yields regeneration in a large animal model
-
Institution: Stanford University School of Medicine (Division of Plastic and Reconstructive Surgery; Institute for Stem Cell Biology and Regenerative Medicine), with NYU Langone Health and the Icahn School of Medicine at Mount Sinai.
-
Country: United States.
-
Journal: Science Translational Medicine, 2025, volume 17, issue 786, article eadt6387.
Impact Evaluation: Current metrics (verified by live search): JCR 2025 Journal Impact Factor of 15.6 (Q1, ranked 3 of 195 in Medicine, Research and Experimental); CiteScore 21.3. Note one Scopus-derived aggregator reports an IF near 13.6; the Clarivate JCR figure of 15.6 is the standard reference, and the journal has been stable in the 14 to 17 band.
The impact score of this journal is 15.6, evaluated against a typical high-end range of 0 to 60+ for top general science, therefore this is a High impact journal