I have found it much easier to lower my LDLc than my HbA1c while taking rapamycin.
No matter what I do seems to lower my HbA1c. I am currently taking 2x500 mg of metformin, and one Glucobay Acarbose 50mg tablet before my evening meal. I recently added one Linagliptin (5mg) tablet in the morning with my metformin, but so far I have seen no effect. I am stuck on the borderline of pre-type 2 diabetes. From some of your posts, you seem to be having a similar problem. I could increase my metformin, but higher doses cause me to have a sour stomach and some indigestion. I eat virtually no sugar or high glycemic index foods. Perhaps my problem is just old age.
Not to get into a diet discussion, but that is what I use to lower my cholesterol. The same diet that I am using to control blood glucose does a better job of lowering my LDLc which is near an all-time low of 40 mg/dL. The lipid-lowering supplements I am using are Pantehine and one
atorvastatin 40 mg tablet.
ApoB is a time and level based risk. A young person has a lot more time to deal with.
Rapa seems to be slowing the rate of aging. An older person is aging at an accelerated rate, and so would get a bigger benefit from rapa.
It’s all guesses but we only get one bet. As an older person, I would prioritize using rapa over perfect apoB. If I didn’t have to choose, that would be even better.
Is it the right approach to assume that a higher Rapa dose is best? What if 2 or 4 mg per week is adequate? How are you determining that more is better?
Seems like you pushing the dose to a level that negatively impacts mtorc2 without knowing the impact on mtorc1?
There may be the danger that elevated hba1c and lipids may only be part of the negative impact of excessive Rapa and the other parts are not being treated.
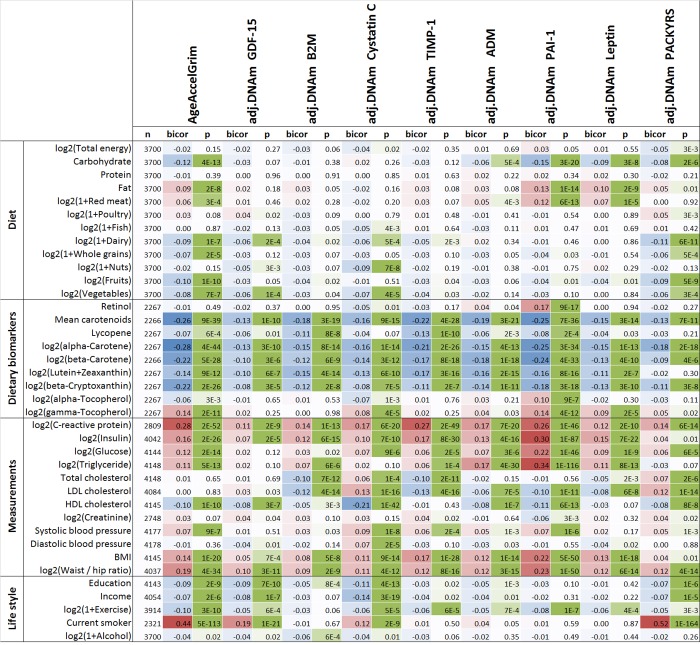
LDL does not look like a strong predictor of mortality compared to other measurements such as triglycerides and glucose. In the correlation table between GrimAge and common diagnostic measurements, LDL had a bicor value of 0.00 and p-value of 0.83 (which suggests no additional predictive value). GrimAge outperforms other epigenetic clocks. Note LDL isn’t even an input variable for Levine’s PhenoAge.
This is to say I don’t believe lowering LDL warrants as much attention as it’s getting here in a general longevity context. Unless one is specifically at risk for/afflicted with cardiovascular disease, there is much more leverage to be gained from optimizing other measurements, such as triglycerides and glucose.
Beyond that, it looks like one could gain more by following a diet rich in carotenoids (orangish vegetables like carrots, bell peppers, butternut squash) and (surprise) not smoking.
That makes me even more confident that those age calculators are bullshit.
The debate about LDL is over on this forum. You can find that debate here:
The LDL/ApoB camp won decisively. Some from the other camp try to sneak in the same arguments that’s been debunked but almost no one cares to take the bait anymore.
If you define “best” as longer lifespans, and if are talking about the range of dosing that we are currently discussing (not even higher doses… I’m sure eventually there are negative repercussions at some high dosing level, as with every chemical). And if you take out the “big” issue of immune suppression (not as large an issue for mice living in pathogen-free lab environments).
Even if you just look at the results from dosing rapamycin (in mice) between 4.7ppm to 42ppm, where we have the best data, it seems to translate to human daily dosing of between 2.7mg and 24mg of rapamycin. Currently, today, the median for us (from our survey) is around 6mg/week. So we are very low on the dosing curve right now.
To really optimize the human dosing protocols, as Dudley Lamming has suggested, we should be testing TREGs to track our immune system function as we increase dosing.
Given this trend line provided by the past longevity tests (the most well-known ones), we know the dose / response relationship for mice:
I think daily dosing in mice is roughly equivalent to about once every 4 days or so in human terms, given the speed at which mice metabolize rapamycin is about 4 times faster than humans.
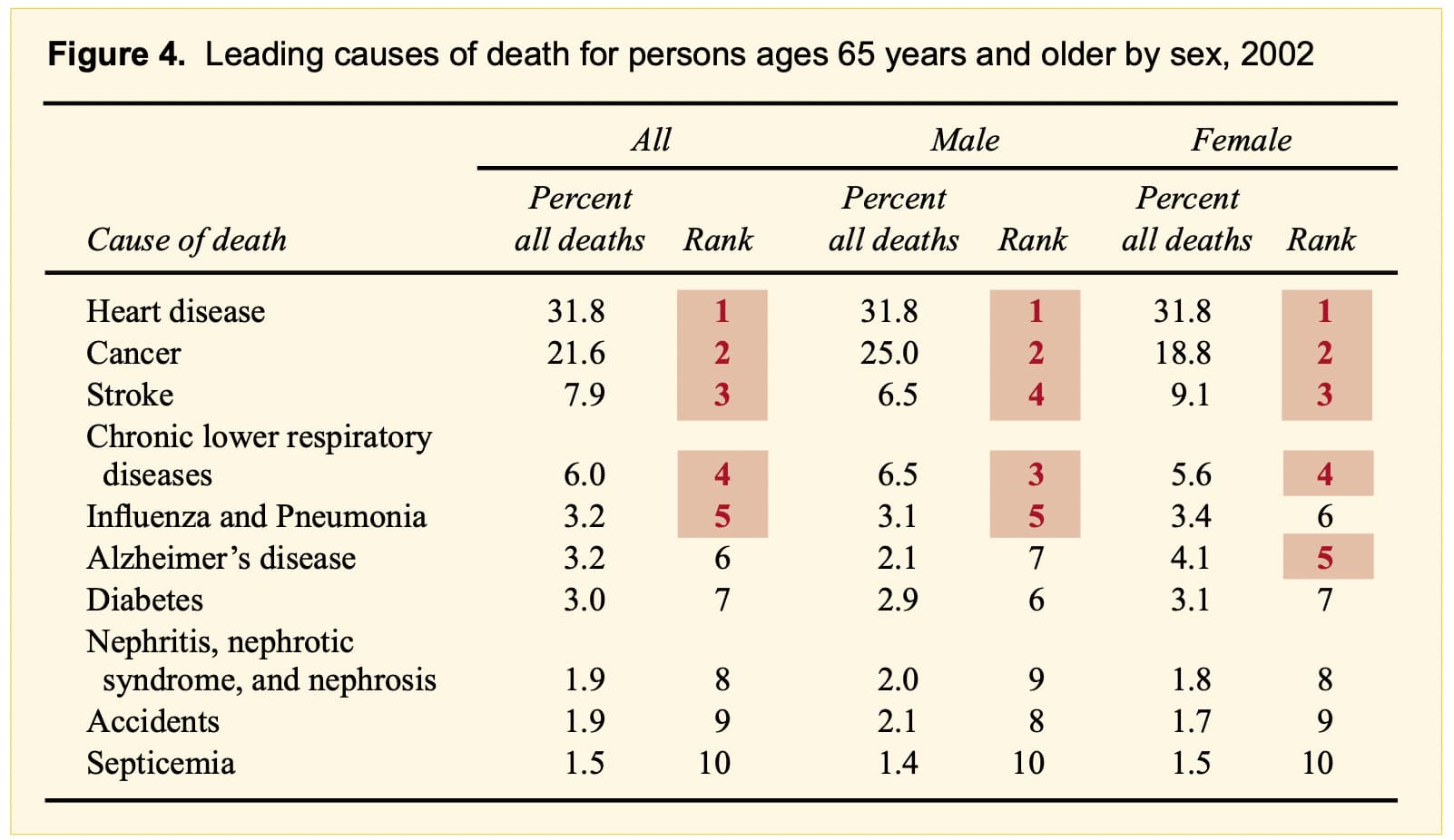
I’m not disagreeing with your data on the GrimAge (or other bioclocks), but how do we reconcile that data, with the fact that “heart disease” is the number one killer:
It may not be a predictor of life span, but it is a predictor of heart disease and stroke.
“Elevated LDL-C level is an independent predictor of atherosclerotic cardiovascular disease. Decreased LDL-C level can reduce the incidence of cardiovascular disease and cardiovascular events such as AMI and ischemic stroke”
That’s a good point and question: the heart disease risk may be accounted for in other biomarkers such as glucose and triglyceride, which make the LDL reading redundant when they are all collected together - the table I posted was for the bicorrelations among multiple variables.
But if the only measurement you have is for LDL, it may still be a good predictor of heart disease risk. However if you have the choice of what biomarkers to measure, I think the table suggests it is better to focus on glucose/triglyceride vs LDL
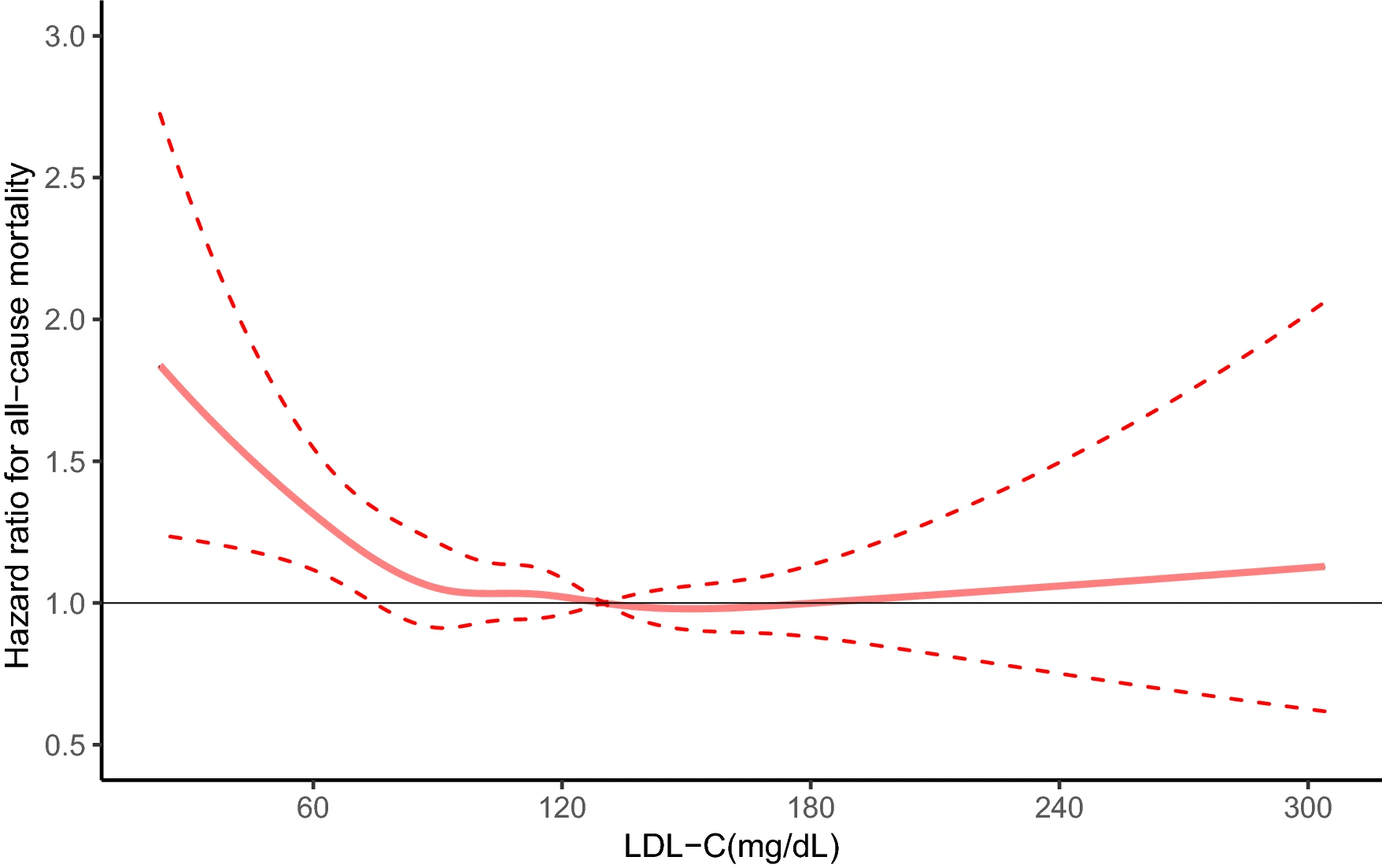
I am aware of the controversies regarding this chart and the optimal LDL level in general. As I said, “overall if I had to guess, I would tend towards lower LDL is better”.
Also there is no such thing as “debunking”. There is only conflicting research, the most recent of which suggests lower is better. But the tide can shift the other way in the future as it did before here.
Since we are much closer to the 4.7ppm dose that produces a 3% and 16% median LS increase in males and females respectively (in mice), this seems to suggest female users of rapamycin on this forum may experience much stronger benefits/effects from rapamycin use. I wonder if that is the case in practice? Made me notice there a fewer posts on rapamycin effects by females on this forum.
After half a century of research, it’s become pretty clear that the lower your apoB the better. Whether there is a lower limit or not is unknown, but it’s definitely lower than whatever clinical guidelines recommend today.