After a long period of contemplation, I believe we should base our Rapamycin dosage on our blood markers. How do we do this?
My thought is that we should take the highest dosage of Rapamycin possible that keeps our HBA1C and LDL (ApoB) just inside normal ranges while taking an optimal dosage of Metformin and Rosuvastatin to help keep us in those ranges.
Here’s how I would do this. First determine an optimal dose of Metformin. I am assuming between 1-2 g daily. Then determine an optimal dose of Rosuvastatin. I am assuming 5-10 mg daily. Then determine a level of Rapamycin that will take your blood markers to the high end of normal and take that dose. Test in 3-6 months.
If your blood markers are out of normal zones, cut back on the Rapamycin. If it’s at the border of high, congratulations, you’ve found your ideal dosage. If your blood markers are in the middle of normal, you can up your dosage.
Why use this method? Well, we have excellent data on the affects of HBA1C and LDL on health so we can base our dosing off of these well researched factors.
This provides a dosage tailored to your individual biology.
Thoughts? Any other blood markers that should be considered?
I had thought of targeting optimal levels of HBA1C and LDL, but for some (like myself) a regular dosage of 6 mg equivalence of Rapamycin (2 mg + GFJ) already takes me to just outside normal ranges for both. So, if I want to hit optimal levels of HBA1C and LDL, I would have to cut my dosage of Rapamycin to below 6 mg equivalent to a dose which would have negligible effect or increase my intake of Metformin and Rosuvastatin dramatically. In my opinion, Rapamycin trumps optimal HBA1C and LDL so long as they both remain in the normal zone.
To back this up, we know from mice studies that giving Rapamycin to diabetic mice actually decreases their life expectancy as the mice die due to diabetic inflammation instead of cancer. So, I believe that going outside of normal levels while taking Rapamycin is detrimental to health.
So, I beleive that:
Taking Rapamycin is beneficial to lifespan and healthspan
Taking Rapamycin with diabetic HBA1C levels is detrimental to lifespan and healthspan
Taking Rapamycin with elevated LDL (ApoB) levels is probably detrimental but not as detrimental as #2 above.
Taking larger doses of Rapamycin is better for lifespan and healthspan than smaller doses.
I’m trying to find a way to combine all 4 factors above to create an optimal dosage. This will vary by person based on their own biology.
Of course this is just a first-pass, and I’m opening this up to the community as to how to fine-tune this process. Consider this a rough draft. Let’s polish it or come up with something better.
Makes sense. I think we should acknowledge an ideal plan vs a practical alternative. You are convinced (rightly so in my opinion) that rapa will help you even if it pushes you out of ideal blood marker zones. But targeting the low All Cause Mortality marker targets is the best start point I’d argue.
Also, should we also look for markers on common rapa issues like immune system (WBC and inflammation), kidney function?
@Joseph_Lavelle I like how you think! If we can come up with a better way through other biomarkers, I would agree. However, if I look at my own blood tests, only HBA1C and ApoB are out of whack due to Rapa. My WBC, CRP, and Kidney function parameters are all excellent and therefore are not a good basis for determining Rapa dosage IMHO.
Of course, if you can lower your LDL levels further, that would be great. This method is a way for you to maximize your Rapamycin dosage. If you decide to weight LDL as more important, you can modify your statin usage or reduce your Rapamycin dosage.
Honestly, I think HBA1C may be the more limiting factor.
An alternative supplement to consider is berberine, which shares a similar effect with metformin but also acts as a PSCK9 inhibitor to lower LDL when comparing equal doses of the two.
It’s also relatively cheap and OTC in the US.
As to the dosing ratio with rapamycin, I would bring up the ITP 2011 trial of rapamycin with metformin as a reference, given this was the ITP researcher’s guesstimated ratio for extending lifespan in mice.
Rapamycin was dosed at 14ppm and metformin at 1000ppm, which suggests a metformin dose at 71 times the dose of rapamycin (i.e. 10mg of rapamycin with 710mg of metformin/berberine).
Its interesting… we’re trying to guess the probability that one of these (e.g. lower LDLs, or higher rapamycin) is more likely to increase our lifespan.
I’m going to try the approach of targeting the optimal LDL, (using all lipid management approaches at my disposal) while trying to maximize the rapamycin doses (while watching all other key biomarkers. I think I’ll do monthly blood testing of all the key variables I can reasonably identify). Will share results. It would be great if other people taking this approached shared their regular data.
I’ve not seen any blood glucose disregulation - but will watch for that also.
Actually, I just re-checked my pre and post-Rapa blood work and it appears that my LDL was impacted more than my HBA1C (although that was impacted as well). I am going to re-test everything in about 3 months and we’ll see how things are progressing now that I have added Rosuvastatin to the mix. I will stay on my 6 mg equivalence of Rapa until then.
Good luck to you all. Hopefully we can find a way to nail this thing down so that we aren’t taking as many Wild Ass Guesses (WAGs)!
that is assume there is causation there but I think it’s being highly debated by several leading experts including Dr. Blag and Dr. Matt Kaeberlein. Peter Attia also has never mentioned the causation. Perhaps only a subset of the population would have elevated glucose and lipids. We should do a specific survey on how long you are on rapamycin, along with the dose and trendlines of HBA1C and LDL.
Another approach would be to study the glucose and lipid profile of long-term rapamycin users (transplant patients) to see the trendlines over time. And cut risk factors by half because of lower dosing and pulsing?
I think the causation is there for most people. Even the diabetic mouse study shows us that diabetics should not take Rapamycin.
It is possible that many people have biological or other mitigating factors (gym rats, genetics, medications) that can keep lipids and blood sugar down so that any increase is countered and not detected.
For me, there’s definitely a sizeable bump in lipids and blood sugar, and the only major change has been the Rapamycin.
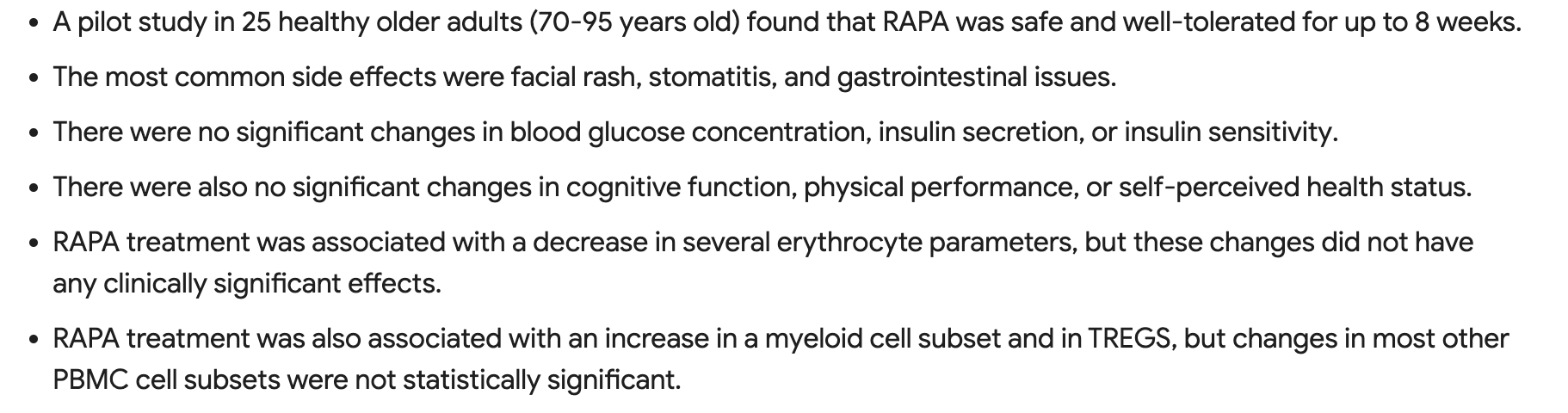
That was a study involving a very low dose of 1 mg daily of Rapamycin. This would probably not inhibit MTOR2 and not cause any lipid dysregulation. Most people have no side effects at that level so the results are not surprising. I would expect different results for much higher doses.
As an aside, 1 mg daily probably is an incredibly safe dose regimen. However will it be effective?
I would not call this dose very low. Depending on your metabolism the blood serum concentration will build over time since this is usually starting therapeutic dose for transplant patients as well.
One of those approaches has actually tens of thousands of people in double-blind placebo controlled trials and genetic studies on the mechanisms… Seeing this objectively, one has clearly superior evidence. It requires one to look past one’s biases, sunk costs, etc…
I’m not touching rapamycin until my lipids are optimal. And I will adjust my dose / other pharma drugs if they go out of optimal range because of a mTOR inhibitor.
It’s not effective in this regard if you compare the mmol/L difference between pharma PCSK9i vs. berberine. Berberine barely moves it, while the non-dirty pharma drugs halves it. Berberine is a dirty drug so not unexpected.
Oh - I’m not disagreeing with you on that. No question the data is much better on lower LDLs/ApoB.
But the devil is in the details. Is the marginal longevity benefit of going from 6mg to 8mg of rapamycin worth the cost of going from (for example) 70 mg/dl to 80 mg/dl? For this type of trade-off we have little to go on.
70 mg/dl is already too high imo, so you’re not even in optimal range.
What sucks is that statins probably can’t get one below 70 mg/dl.
A combination therapy like Peter Diamandis is doing is probably required for most of us.