The Timing Reality Check: Urolithin A Rescues Aging Brain Biology, But Fails to Reverse Established Memory Loss
Urolithin A (UA) is a widely discussed postbiotic molecule known for triggering mitophagy—the cellular recycling of damaged mitochondria. While previous studies tout its benefits in Alzheimer’s models and muscle health, its efficacy in natural brain aging has remained uncertain. This new research investigates a critical clinical question: Does the timing of mitophagy activation matter for cognitive preservation?
The short answer is yes. The researchers found that while UA effectively prevents age-related cognitive decline when administered early, it fundamentally fails to reverse memory loss once significant mitochondrial and synaptic damage has already occurred.
The study employed two complementary mouse models to test early versus late intervention. For the late-stage model, 16-month-old naturally aging C57BL/6J mice—which already exhibit cognitive deficits—were given UA for eight weeks. On a molecular level, the compound performed precisely as intended. It boosted ATP production, enhanced mitochondrial fusion proteins (Mfn1 and Mfn2), upregulated biogenesis markers like PGC-1a and Nrf2, and cleared pathological tau proteins (PHF-1) from hippocampal synapses. Yet, despite this impressive molecular repair, the mice showed no improvement in spatial or recognition memory. The biochemical rescue did not translate into functional cognitive recovery.
Conversely, the early intervention model utilized 5-month-old SAMP8 mice, a strain that undergoes accelerated aging and typically develops cognitive deficits by six months. When these mice received UA prior to the onset of memory loss, the results were striking. Hippocampal ATP levels surged by over 4-fold, toxic tau accumulation was blocked, and spatial learning was significantly preserved. Intriguingly, after this successful cellular stabilization, markers for mitophagy and biogenesis actually downregulated, suggesting the mitochondrial pool had reached a healthy homeostatic state that no longer required aggressive turnover.
These findings establish a critical reality check: metabolic therapies and mitophagy activators are not magic erasers for established neurodegeneration. Once synaptic networks are compromised, fixing the cellular power grid is insufficient. Compounds like UA must be utilized preventatively to protect brain healthspan.
Researchers: This research was conducted by scientists at the Laboratory of Neurobiology of Aging, Fundación Ciencia & Vida, and Universidad San Sebastián in Santiago, Chile.
Journal: It is published in the journal npj Aging.
Impact Evaluation: The impact score of this journal is 5.6, evaluated against a typical high-end range of 40–60+ for top general science, therefore this is a Medium impact journal.
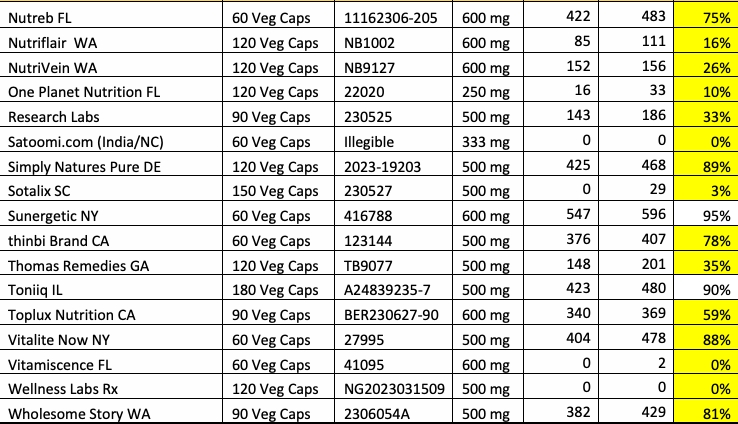
18 of 33 brands tested contained less than 40% of labeled potency, and seven of the 33 tested samples had 1% or less of berberine potency. These seriously flawed brands were tested for the first time by NOW’s program, and may be new brands. These included Earth Bare, Greabby Gummies, GreenPeople Formula, KoNefancy, Satoomi, Vitamiscence, and Wellness Labs Rx.
It seems the current company behind the brand (Health and Wellness Associates, Inc) was incorporated in 2023, even though the brand existed before (probably under a different company?). Rose Cabasso also owns MyLiquidNaturals.
If the above is correct, then Wellness Labs Rx is a very low-quality brand that should be avoided at all costs.
In more recent times, ULA has been proposed as an antiaging compound, leading to the growing use of both diet and supplements to raise blood levels.2 Here we present a series of urinary stones containing urolithin A, the first such, to our knowledge, reported in humans.
Over-the-counter supplements were reviewed with these 6 patients, and none were taking ULA supplements.
Though stones derived from drugs or supplements are rare, their recognition by stone analysis is important so the causative exposure can be stopped. Health fads and drug development may expose people to poorly soluble compounds that crystallize in the urinary tract. Stone analysis laboratories must be vigilant to recognize and identify new stone components.
ULA supplements have been well tolerated in human studies, though trials have been short-term (up to 4 months). Only 1 urinary stone event was reported, without stone composition details.
This inability to produce potentially-therapeutic ULA from foods in some patients has prompted the development of commercially-available ULA supplements. These supplements bypass microbial conversion and provide significantly higher systemic exposure—plasma and urine ULA levels can be up to 6 times greater than those from dietary sources.9 Nonetheless, none of our ULA stone formers reported ULA supplement use. We anticipate cases may emerge as supplement use increases, given the uniformly high ULA excretion it induces.
ULA, a compound derived from the gut microbiome metabolism of food polyphenols and also sold as an over-the-counter health supplement, can precipitate from urine and be incorporated into urinary stones. Addition of ULA as a standard in IR spectral libraries of stone analysis laboratories is critical to allow ULA identification so clinicians can intervene and identify foodstuffs or supplements that are contributing to stone formation.
I’m not sure it’s relevant unless someone has a history of calcium oxalate/phosphate stones, low urine volume, or hyperoxaluria?
One thing I find interesting that most people ignore is that the solubility of various ions varies by the pH of the solute. (normally urine). I have studied this with gout because it is obvious that a low urinary pH plus low urine volume makes gout more likely.
There are stones eg (Ca-P) which are more likely at higher urinary pH. Hence it is not a one way issue, but there seems to be good evidence that alkaline urine (and oddly enough acidic fecal matter) are both good for healthspan.
It is interesting that UA is being positioned as a geroprotective. I have viewed it as a modulator of other functions that support primary geroprotectives, such as vigorous exercise in old age. I take UA to address a specific muscle problem that appears to be genetic. Going back as far as 1986, my LDH levels have ranged from borderline to clinically low and my genetic profile suggests a predominance of endurance muscles. This combination appears to have proved beneficial in the competitive distance running I engaged in for most of my adult life. Subjectively, my muscles are very slow to “warm up” but quite literally, the longer i ran – up to many hours – the stronger they became. This profile shifted in my mid-70’s when it became clear that I was unable to push my lower body muscles sufficiently on hill climbs to reach Zone 5 periodically, one of my goals. The limitation profile was definitely muscular and not CV. UA has definitely reversed much (maybe 70%) of this problem and I am again able to push my muscles hard enough to move into an anerobic zone with high respiration and heartbeat. I am aware of the nuance in summarizing these issues as briefly as I have, my only point here is to present an example in which UA has resulted in muscle performance gain.
You’re welcome. Btw, I first googled the brand and couldn’t find much, then asked ChatGPT to dig deeper and was surprised it found all those things. Good to know to do a background check on other companies.
To be fair and give them a chance, I wrote an email to the company. We’ll see it they come back with anything substantive or just a third-party certificate of purity that tells you nothing about capsule dose.
Put off by the cost of Urolithin A, I’ve been taking its sister molecule Urolithin B for a month. Everychem sells two grams of powder for about $30. Beyond it’s lower cost, however, the B metabolite has been shown to improve kidney function, exerting anti-fibrotic and anti-inflammatory effects in rats with induced kidney damage. This is what attracted my interest.
A blood test yesterday showed that my GFR has increased from 28 to 34, a rise of 20% in 30 days. This increase may not be due entirely to Urolithin B. During the same period, I’ve been taking 2 tsp/day of sodium citrate, an extremely effective acid neutralizer. I also can’t rule out a possible delayed response to SS-31, which I tried two months ago.
Have you considered pomegranate peel extract?
Assuming you’re the right Metabotype It should get you to an effective dose of urolithin a very cheaply (3g of powder im a bit of kefir).
You can test for Urolithin A - to see if its working - and that’s only a one time test. Or yiu can take my approach - if you start by dosing alongside actual pomegranate: if you find yourself craving pomegranate it’s a decent sign you’ve got the right gur bacteria.
I do balance the citrate. I get about 2,000 mg of potassium from food, 400 mg of magnesium glycinate in capsule form, and 1000 mg of calcium carbonate as an antacid.
From reading your paper on citrate, which warned about taking too much too soon, and from my own experimentation, I think that 2 tsp/day is a safe but effective dose.
It lowers my serum CO2, an acid, and raises my GFR and HGB. As an acid neutralizer, it is far better than sodium bicarbonate, which is by comparison a blunt instrument.
You will get sodium from food as well. If you increase the dosage also you will need to continue balancing cations. I have taken the dosage quite high and intend doing that again in the near future (probably Saturday).
The alkalinising effects are quite good. It is worth getting pH strips to monitor the level.