Quite a shame it gets as much press and attention as it did.
1 Like
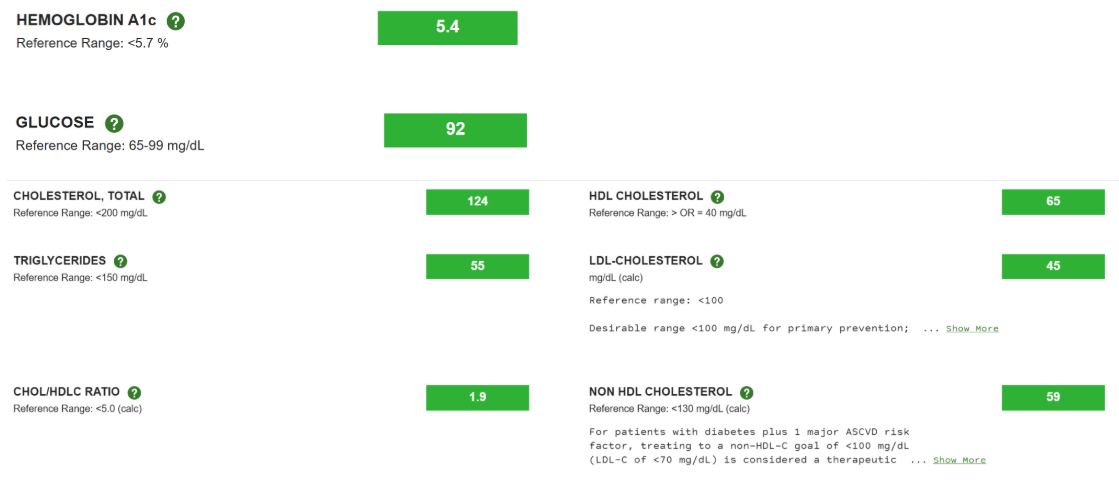
Wrong. Blood work actually showed a statistically significant deterioration in lipid profiles and glucose metabolism—and that was after just 13 weeks. It makes absolutely no sense to assume that taking it for a longer period would somehow improve, rather than worsen, markers like blood sugar, lipids, the epigenetic clock, or grip strength.
At the very least, the 1mg or 6mg weekly regimens are completely untenable in current clinical practice. I personally do not follow the 6mg weekly protocol adopted by the majority, because based on all available literature, 6mg per week is not a scientifically sound regimen. Our current focus should be on determining an appropriate regimen, rather than simply prolonging the trial duration.
1 Like
The logical approach now would be to design a trial that establishes multiple rapamycin dosage arms to investigate which dose improves physiological markers in the short term, before proceeding to long-term trials with that specific dose.
Most people just simply follow the dosage recommended by Alan Green. Because he has a huge reputation in the anti-aging community, criticizing him can easily trigger a backlash. My take is that you just need to watch a few of his interviews to see what his actual level of expertise is.
4 Likes
Wrong…Statistically and clinically significant are two different things. The glucose profile was negligible (increase of 0.1% for HbA1C) for any clinically meaningful change, especially without a repeat measure. Grip strength is silly when the intervention 1) didn’t engage grip strength training at all and 2) it didn’t even approach a statistical significance. It is as general of a measure as BMI. Works well at very large scale but fails when sample size is far too inadequate. Epigenetic clocks have yet to demonstrate any meaningful translation. Maybe wait for some larger scale higher quality studies coming before over-interpreting the results of a single low quality study.
I could complain about their lack of dietary control and activity monitoring outside the exercise sessions but I wont because I know the study had limited funds and the team performing it was naive to the complexities of a drug-exercise interaction study.
1 Like
Wrong.If this were a Phase I anti-cancer drug trial, this slight elevation in blood glucose and lipids would be considered a ‘negligible and completely acceptable mild side effect.’ However, this is a trial exploring ‘healthy longevity.’ Older adults are taking the medication to become healthier.
1 Like
Maybe statistically significant, but it is small. Members of this forum recognized this years ago and took steps to counteract it by adding a statin, which most should probably be taking anyway, or agents such as bempedoic acid and ezetimibe for lipid control and metformin or other glucose meds.
Until recently (I am now going to test a very high monthly dose), I had been taking high weekly doses for 5 years and had no trouble keeping lipids and glucose under control in spite of my age. A younger, healthy person would probably need only minor interventions.
5 Likes
Tiresome. I’ll respond to this kind of post from you one last time. You don’t pay attention, you make unsupported and wrong assertions with zero research that is easily accessible and above all, you ignore what is plainly addressed in the posts either because you don’t read, or don’t understand what you read.
“In this case, it showed that there is blunted exercise benefit* - that’s it.”
I was responding to Nik_017’s point about muscles - as he observed, the study didn’t measure anything regarding muscles except exercise performance. Here, “in this case” refers to muscles because that was under discussion by Nik - the study in the case of muscles only showed blunted exercise benefit (no other muscle related markers or biopsies) - that’s it. Dragging in blood work not related to muscles is completely irrelevant. Read. Understand what you are reading. Pay attention.
Nonetheless, even in that post, I put an asterix wherein I summarized what the whole study showed:
*sum total of what the study showed:
““(1) rapamycin at 6mg (2) once a week (3) over a period of 13 weeks (4) blunted exercise performance improvement (5) in select measures of select domains (sit-stand, walk, grip) (6) in older individuals 65-85 of age (7) who underwent a regular exercise program (8) and who were initially largely sedentary at baseline (9) and the study included some bloodwork biomarker results.” Everything else is speculation, whether scientifically legitimate or not.”
The glucose and lipid and other markers I noted in point (9) - so that was covered too. Pay attention.
As you would say - “wrong”. All the study showed is results after 13 weeks. Unlike you, even Dr. Brad understands that the study is 13 weeks. What does or does not make sense “to assume that taking it for a longer period would somehow improve, rather than worsen, markers like blood sugar, lipids, the epigenetic clock, or grip strength” - is speculation and extrapolation, whether legitimate or not is subject to debate (as I showed at length in my long commentary on the study above), and the import of those markers longer term is in turn subject to debate. Because you don’t read, I will - this time - quote myself from those posts:
“Now, that doesn’t mean that there may not be actual trade offs with CR or rapamycin - the CALERIE study in humans showed lower bone density on CR. In animal models there were hints of CR causing an initial dip in bone density, but compensating for it with superior bone architecture ultimately resulting in superior bone strength in old age. But that is not proven in humans, so from an abundance of caution, I call bone density a genuine trade off in CR. Same way rapamycin can show glucose and lipid disregulation - even though MK claims that in mouse models this normalizes over time, several weeks - I still am cautious and allow that rapamycin may genuinely have a side effect of worse glucose and lipid control. But exercise performance? Nah.”
Rather than pop up like jack in the box with “Wrong”, it would have been useful for you to see that I actually addressed the points you brought up. Read. Understand. Pay attention. And in that paragraph, are the counterpoints to your assertions. Because when you say that it makes no sense to assume that glucose and lipid numbers might get better over time - it is your assertion that is wrong, because MK showed that in mice rapamycin can initially dysregulate glucose and lipid numbers that subsequently normalize within weeks - showing exactly that it does indeed make eminent sense to allow for the possibility that rapamycin may do the same in humans. The body adjusts to any drug. Initial effects may, or may not persist. That too is true of rapamycin. To see the effects of any drug needs longer term trials - a constant observation in multiple trials: we need longer term results, which we sadly often cannot afford in longer trials. Including here, where everyone - even Dr. Brad - understood that the 13 weeks duration is a very serious limitation of the study. Congratulations, you just did what I was warning about in all those long posts commenting on Dr Brad’s study - ignoring the 13 week limitation and illegitimately extrapolating the results beyond that to assert that those effects must remain longer term. Why illegitimately - I explained in those posts the distinction between legitimate and illegitimate extrapolations, the illegitimate ones are the extrapolations which do not take into account contradictory contextual data, in this case the MK data in mice regarding rapamycin and glucose and lipid levels longer term vs shorter term.
But it’s worse than that, because I actually allowed that there may genuinely be long term lipid and glucose dysregulation contrary to MK’s speculation. MK made the point about mice results as a caution that it may be the same with humans - longer term the body may get back to homeostasis (as happens frequently with all kinds of drugs). I’m taking a more conservative approach and allowing that indeed that might be long term glucose and lipid elevations: “I still am cautious and allow that rapamycin may genuinely have a side effect of worse glucose and lipid control.” Read. Understand. Pay attention.
Far from not noticing this, I addressed this directly. You bring up the lipid and glucose effects (after 13 weeks[emph.]) - but what of it? And? So? Is this your point:
“However, this is a trial exploring ‘healthy longevity.’ Older adults are taking the medication to become healthier.”
And what is the implication of this dysregulation - that the net result of taking rapamycin is that people don’t become healthier? You need to show that. You need to show that this effect overrides any possible benefits of rapamycin otherwise. This doesn’t seem to be the case in animal models. It’s called a trade off. Whether that trade off is worth it - a net negative - or not, needs to be shown, not asserted. For humans - we don’t know. You certainly don’t. I don’t. Nobody does - in humans. In animals we do - the negative effects of rapamycin, including on bone health and osteoporosis - are compensated by overall life extension (marmosets). Without human trials we cannot answer that question. It therefore represents a gamble, and each of us gambles differently depending on their own analysis, intuition, risk tolerance and we may each come to different conclusions. Yours is only one of them. Mine is another. To each their own. The data is not there for it to be anything more than a gamble. Assertions should reflect that uncertainty - unlike your assertions. In my part IV of the posts commenting on Brad’s study I addressed this very point - it’s too long to quote. Read. Understand. Pay attention.
Incidentally, this glucose and lipid effect is not present for everybody on 6mg/1-week of rapamycin. In fact, it seems to be a minority. I have no such effect at 8mg once a week. And furthermore - as I pointed out in one of the posts above - you can actually address this through other drugs, drugs which you might want to take regardless of whether rapamycin dysregulates your glucose and lipids, exactly as I do with statins and SGLT2i. This is a common approach of minimizing side effects while retaining benefits - this is what any self respecting biohacker would look at in such a context.
And then you wrench in a completely different class of effects in that collection of assertions: “It makes absolutely no sense to assume that taking it for a longer period would somehow improve, rather than worsen, markers like blood sugar, lipids, the epigenetic clock, or grip strength.”
Dear Lord, please give us patience. In one sentence you managed to completely mix up and compound whole classes of wrong assertions. Lipids and glucose I already dealt with. That’s one class. But you threw in there “grip strength”. The whole entire lengthy exhaustively argued point of all these posts was precisely the issue of why muscle performance - ONE MEASURE OF WHICH WAS GRIP STRENGTH - as assessed over 13 weeks by the metric of exercise response tells us nothing about longer term effects even on exercise performance and response. All those posts - completely over your head, with that one marker thrown in by you in that muck sentence - “grip strength”. Sorry, but I am not going to quote all of those posts again - READ. Understand. Pay attention. I actually made a distinction wrt. muscle performance (including grip strength) where I allowed that rapamycin may be deleterious for glucose and lipid BUT NOT MUSCLE: “I still am cautious and allow that rapamycin may genuinely have a side effect of worse glucose and lipid control. But exercise performance? Nah.” The whole point of all those posts, SMH. Yet there you are, blithely tossing in grip strength on top of completely different class of effects on glucose and lipid markers, all in one sentence, whew. A sentence straight from confusion hell. And then for good measure you toss in, like and empty beer bottle - “epigenetic clock” - really? Do we need to do this whole rigmarole about epigenetic clocks? Oh boy. Go do some reading, I’m not going to spoon feed you.
This is exhausting and unrewarding, because there is no value in having to correct for someone not reading or understanding. It takes much longer to untangle the unholy mess of one paragraph where you manage to compact a dense collection of “wrong” everything - assumptions, reading comprehension, lack of basic knowledge in the subject matter. You are like my cat - I get up to make coffee and he in the meanwhile walks across the keyboard and then it takes me great effort to untangle the mess he makes with a few seconds walk. Not worth it. This is akin to the gish gallop style of argument which amounts to flooding the zone with sh|t that then takes hours to clean up. Not worth it.
So, from now on: if you do not bring any novel points, if you do not take care to at least read what you are responding to, if you make no effort to understand what you read or acquaint yourself with at least 101 level in the subject matter, I will no longer respond. We went through this in the imeglimin post - here we are repeating this gish gallop pattern. Careless throwaway posting with dramatic assertions “WRONG!” backed up by nothing that then takes endless effort to untangle and put into some kind of context - not worth it. Nobody benefits. Read. Understand. Pay attention. If you continue to post in this style, I will not bother responding. Make novel points with at least a minimum of care, otherwise it’s all a waste of everybody’s time.
6 Likes
RIP to Alan Green but I felt similarly when I heard his interviews. Seemed like a great man though.
I do hesitate to take another dose of Rapamycin. I took one last week after about 3-4 weeks off and started to develop a minor sore throat a day or two later. Honestly, I hesitate to take it again since none of us really know what the best way to take it is. There seems to be a relatively small margin of error with the dosing. If we mess it up, it can be a net negative. That being said, if we figure it out, it could possibly be a home run. I think I will wait a little before we know more.
I think you mean “he used to have” a huge reputation, because he’s passed away already, or maybe you didn’t know it?
C’mon man! ![]() He was almost dead when he started taking rapamycin.
He was almost dead when he started taking rapamycin.
2 Likes
I wasn’t actually implying anything, I simply was telling him he’s passed away (seemed like he didn’t know)
Don’t be a “Karen.”
1 Like
If you don’t understand the physiology then don’t even start the study. Every result that Brad got in this study was as completely predictable and adds nothing to our knowledge base of Rapamycin.
In short, elderly people taking Rapamycin once a week effectively dialed mTOR down. We know it dialed it down because that arm of the study improved muscle strength but at a lesser rate than the placebo arm (who were obviously not dialing mTOR down and so were free to build muscle).
If Brad had rather done a 6 month study, where the Rapamycin arm took the drug for 13 weeks whilst enjoying other autophagy-inducing activities like zone 2 exercise, ice baths, a diet low in leucine, supplementing with spermidine, and thereafter they turned to weight lifting and a high protein. high leucine diet then I predict the Rapamycin arm would have shown far better results than the placebo arm.
The saddest thing is that Brad mortgaged his house to find this unhelpful study.
1 Like
As I understand it he is expecting a profit from his supplement which will pay off the loan.
It remains, however, that lots of studies when they hit the constraints of what is required (such as placebo) and cost end up in a situation were there is no additional information. PEARL for example concluded that if you don’t take a lot of rapamycin not much happens.
Hi John
I agree. I think the PEARL study is reflective of what we can expect with human rapamycin use - mild benefits but unlike the preceding mouse, worm and fly studies, no longevity benefits from rapamycin alone. Doesn’t mean that rapamycin shouldn’t be a part of our long term longevity plan but we should temper our expectations of it
I disagree with that. I think intermittent Rapamycin can produce longevity benefits. The dosing in PEARL (which was driven by the need to have a placebo that could not be distinguished from rapamycin itself) was too low to be able to measure any real effects.
As people know I think the mechanism through which Rapamycin has its main benefit could be called a “spring clean”. I would say of mitochondria, but I am happy to agree on a general metabolic improvement. The frequency and depth of such cleans are things for experimentation. I go for deeper and less frequent. However, there are potentially other negative side effects from going too deep.
4 Likes
A lot of this is supposedly due to loss of neuromuscular junctions (how your brain talks to the muscle). Strength is a function of muscle mass, but also how well you can activate it. That’s why a 60kg trained lifter can be stronger than an untrained 100kg guy. However, the 100kg guy will likely have a higher ceiling if he trained.
Hmm, I think the glucose and lipid effects are well known, minor, and expected. They’re also very easily managed.
Grip strength though at least has some plausibility. In the animal studies, mice treated with Rapa have better performance in the various tests of physical fitness. There is a plausible mechanism where aged cells, including satellite cells, are cleared, basically allowing muscles to recover better. But that’s where this sort of study is just way too short to tell us anything. As I pointed out early, untrained elderly lifters will have a big lag time and learning curve when it comes to any sort of exercise intervention. Even a young healthy guy will make fairly negligible gains in hypertrophy or strength over the first few weeks of lifting, simply because you need to recover and adapt to the new stimulus. The greatest gains usually come in the 3-12 month window.
And again, you have two participants in the placebo group who DOUBLED their performance during the course of the study. Any of the gym bros here will tell you that that isn’t something you should expect in anything except untrained people who probably didn’t push very hard in the first baseline test. So it’s really very limited data to draw any sort of conclusions.
1 Like
“I disagree with that. I think intermittent Rapamycin can produce longevity benefits.”
John, let me qualify that statement - I believe that rapamycin and other autophagy stimulators will have profound benefits in extending the healthspan of humans. However, I do not think that rapamycin alone will extend lifespan. For maximum effect, rapamucin needs to be pulsed along with 12 week anabolic phases. I am waiting for the study to show that this pulsing will, in the long run (after 1 year and not at the end of 13 weeks) give an improvement to both muscle hypertrophy and muscle strength, compared to the arm that just drives muscle anabolism for a month. To extend lifespan a rapalogue may need to be combined with SIRT support, senescent cell reduction and epigenetic reprogramming.
So in the mean time, this is what i am doing - a 3 month block of rapamycin, plus an autophagy lifestyle (zone 2 training, ice-baths, spermidine, Urolithin-A, fasting). This is followed by 3 months of an anabolic lifestyle (heavy weights, HIIT, high protein, high Leucine, higher calories, saunas). What I am finding is that the gains in the anabolic cycles are noticeably greater and the body inflammation is reduced (no stiffness, no injuries) than just by pushing hard on a continuous basis.
There has been a mouse study done showing the histological muscle quality improvement from using sirolimus for i think 12 weeks, but not to my knowledge a human study. As far as I am aware there has been no study on pulsing autophagy and then anabolism. In honour of Yoshinori Ohsumi and his 2016 Nobel acceptance speech for his contribution to autophagy research, I think this aught to be done.
Any thoughts on this approach?
I like the term “a rapamycin spring clean”. Please explain in what way you are going deep?
1 Like
The key point is that mitophagy is selective. Although there will be a limited stochastic element you can consider it for example as going for the least efficient say 1% or 2% of mitochondria. 2% is going deeper than 1%.
I am assuming also that the fission, mitophagy, fusion process is working.