I get this on a google search: * Email: brad@drstanfield.com
Alternatively try tweeting him.
Yes John, but I don’t know him and I’m sure he’s inundated by emails. You were a politician - I’m sure you know that having the right person making the request is important! ![]() And I don’t have Twitter/X, since I think it’s detrimental to mental health and longevity!
And I don’t have Twitter/X, since I think it’s detrimental to mental health and longevity!
I do understand having lots of contacts. However, email is relatively easy to filter. However, if you email me at john@hemming.email with a draft request I will send that email to him copying you in.
Someone asked him on his discord I wanna say two weeks ago if he would be willing to give us a clue on what the results were, but he said we have to wait until it’s published. I am sure it will be soon enough.
Exactly… you need some previous interaction…which is why I am able to flag Matt Kaeberlein’s response on this site from time-to-time. We have a 5-years long correspondence relationship… as a subject in his rapamycin off-label use research.
Realizing how busy Matt K. is… and how often he must be contacted randomly, I reserve my interactions for things he would be the best primary source on.
Matt K. rocks!!
Finally…
Full Paper/Open Access: https://onlinelibrary.wiley.com/doi/epdf/10.1002/jcsm.70274
Preclinical models have long established that the mechanistic target of rapamycin complex 1 (mTORC1) acts as a central regulator of both aging and skeletal muscle growth. Inhibiting mTORC1 with rapamycin extends lifespan in rodents, but intact mTORC1 signaling remains strictly required for skeletal muscle hypertrophy in response to mechanical overload. This paradox originated the “cycling hypothesis”: deliberately alternating mTORC1 inhibition for systemic rejuvenation and activation for post-exercise adaptation to maximize healthspan.
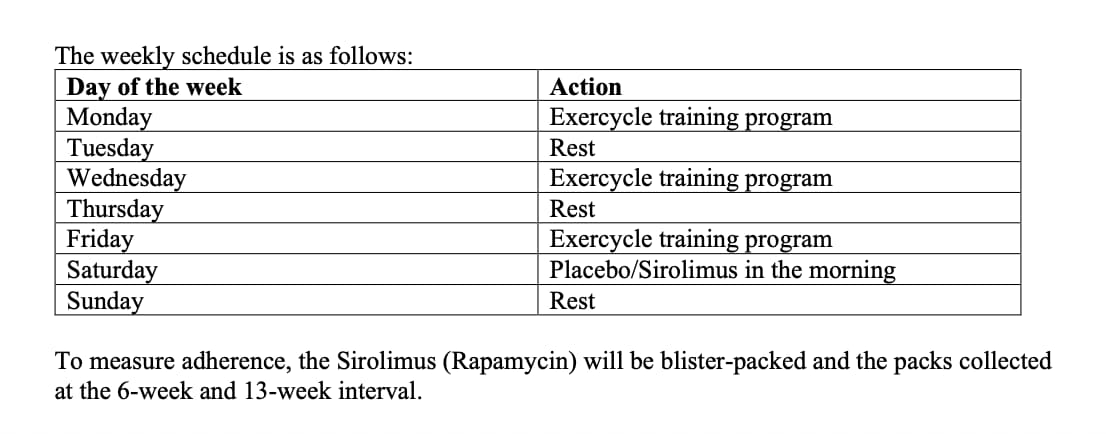
The RAPA-EX-01 trial sought to directly test this hypothesis in humans. Investigators randomized 40 sedentary older adults (aged 65–85) to receive either 6mg of sirolimus (rapamycin) or a placebo once weekly for 13 weeks. Concurrently, both groups executed a progressive, home-based resistance and endurance training program three times per week. To theoretically avoid suppressing the acute anabolic response to exercise, the sirolimus dose was administered 24 hours after the final training session of each week.
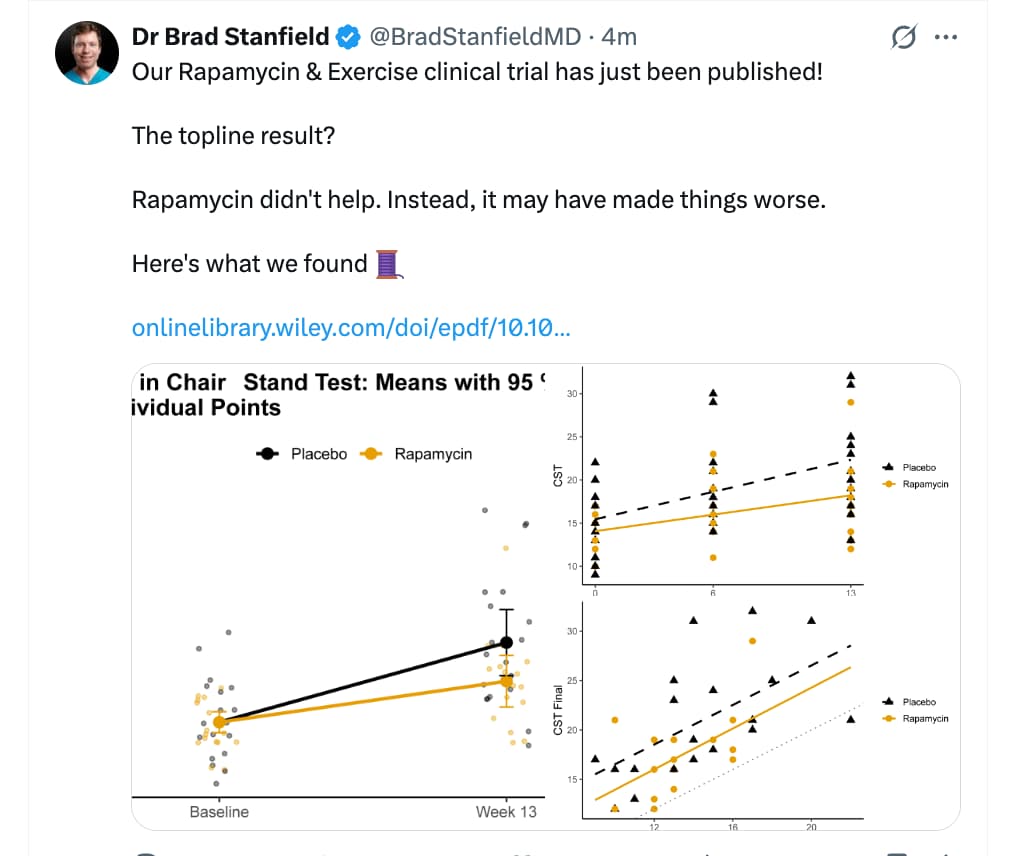
The trial results severely challenge the translational viability of this cycling hypothesis. While both cohorts improved their baseline 30-second chair-stand performance, the intention-to-treat analysis revealed a negative effect size for the sirolimus group compared to placebo (-2.13 repetitions). Furthermore, per-protocol and complete-case sensitivity analyses demonstrated a statistically significant attenuation of functional strength gains in the active treatment arm. Secondary functional measures, including 6-minute walk distance and grip strength, also favored the placebo group, although they did not reach statistical significance.
The safety profile dictates caution. The sirolimus arm experienced a higher aggregate burden of adverse events (99 versus 63), driven primarily by minor infections and constitutional symptoms. One serious adverse event—hospitalization for community-acquired pneumonia—occurred in the active group, underscoring the drug’s immunosuppressive mechanisms.
The failure to achieve concurrent geroprotection and muscle hypertrophy is likely a consequence of pharmacokinetics. Sirolimus possesses a terminal half-life of approximately 62 hours. Consequently, a 6mg weekly dose maintains biologically active concentrations well into the subsequent training week, partially inhibiting mTORC1 during critical post-exercise recovery windows and actively dampening structural adaptation.
Study Design Specifications
Mechanistic Deep Dive
Novelty
Critical Limitations
Brad started this effort about 4 years ago, and the full outline of the original clinical trial proposal and protocol can be viewed in this thread: Rapamycin Exercise Study Moves Forward: Dr. Brad Stanfield's Study Registered in NZ
Rapamycin didn’t help. Instead, it may have made things worse.
That’s what rapamycin does. Blocks mTORC1 => no muscle protein synthesis => blunts the effect of strength training I you do it while the rapamycin concentration is high enough.
Basically the rapa group had less training days than the placebo group.
Sadly the study design was not good.
That’s why there is no point doing strength training the days after taking rapamycin. No issues with endurance training where rapa helps.
To be fair with Brad Stanfield, he gets it:
For all the effort that went into the study it is much like PEARL. no new knowledge
Here is the exact timing/protocol for the exercise and dosing:
With 2 days rest after dosing rapamycin on Saturday morning, I would have thought that the effect of rapamycin on exercise would have been very minimal. I still need to read more to see exactly what percent less the benefits of exercise were for the non-rapamycin group.
Perhaps the take-away from this is that if you want to maximize muscle and strength increases we need to space our rapamycin dosing out beyond weekly…
My view is that we need mTOR to operate normally a lot of the time. As Rapamycin has a long half lilfe that means material breaks between dosing. I am currently taking a *large dose, but no more frequently than every 6 weeks.
My last dose was quite interesting in the effect it had on delaying the repair of my weekly venepuncture. Because of the weekly full panel blood tests I can see the effects on platelet count, RBC and WBC as well as knock on effects.
What I am doing is testing the geroscience hypothesis with a combination of interventions arranged to be synergistic on the acetylation pathway. Rapamycin is only one of those interventions.
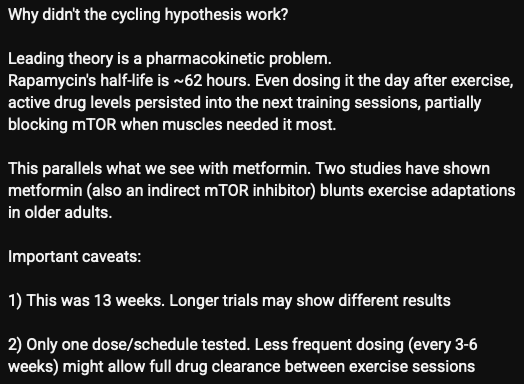
I have asked my standard question in relation to the paper and the response is here:
The AI summary conclusion is: (the analysis at the link)
This is a useful and genuinely novel trial. Its main contribution is to show that weekly 6 mg sirolimus, timed 24 hours after weekly exercise, does not improve short-term exercise adaptation in sedentary older adults and may modestly impair it while increasing minor adverse events. That is a meaningful negative result.
The paper’s main weakness is that it cannot cleanly separate “rapamycin is bad for exercise adaptation” from “this specific dose/timing regimen was poorly matched to the exercise schedule.” So it weakens the simple version of the cycling hypothesis, but does not fully kill the broader idea that a different cadence or longer interval could work better.
My own view on Brad Stanfield’s work is that the outcome is what would be mechanistically predicted. It does warn people off weekly dosing which IMO is helpful, but to me it was obvious that weekly dosing is suboptimal. One should really conclude that mTOR has a function and unless someone has medical reasons to suppress the immune system, it should be allowed to run free part of the time.
There is data pointing to taking high dose rapamycin once monthly or even less frequently than that. The issue is, as Dr. Stanfield pointed out, risk of infections as such doses. Isn’t everolimus patent-free by now?
Although Everolimus has a half life of 30 hours as opposed to 60 there is I think still an issue.
There are risks from high mTOR inhibition other than infection. Edema is another one.
I think the reason I don’t have particular problems although I may have had a mouth sore last time (20th March) is that otherwise my immune system seems to be strengthened. I am not sure what that is although it could be citrate.
I agree that we need material breaks.
My heuristic is to think of rapamycin in terms of fasting - how often should we do a full, say, 3 day fast for optimum longevity? For that, every 6 weeks seems sensible. What size dose do you have?
I’m curious whether others think along similar lines.
I now do fortnightly but just for a part (33%ish) of the year and lower dose - between 4 to 8mg. Focussing on lower impact autophagy agents (urolithin a, sauna, exercise, 8-12 hour eating window, spermidine etc) for base autophagy.
Are you thinking everolimus is superior because its half life is lower?
That would make sense to me - the analogy would be that everolimus approximates to a shorter “food fast”.
Also there’s less uncertainty with everolimus - the half life of sirolimus seems individually highly variable and I do wonder whether everolimus with its shorter mean half life - would be superior because it would have lower individual variance in terms of AUC.
PubMed Central (PMC) (.gov) +1
. Everolimus has a much shorter half-life of about 28 hours,
PubMed Central (PMC) (.gov) +1
.
I don’t comment on the size of my dose as I would not suggest anyone else did this without monitoring.
On the other hand at the moment I am doing a water fast on Mondays, Wednesdays and Fridays. I don’t want to fast so long that I start using up protein.
Understood.
In terms of alternate day fasting. Do you monitor lean muscle mass to make sure you’re not overdoing Mtorc inhibition? Or some sarcopenia monitoring (hand grip? chair stand test etc).
https://www.mdpi.com/2072-6643/17/23/3691
Effects of Four Weeks of Alternate-Day Fasting with or Without Protein Supplementation—A Randomized Controlled Trial
More generally, I’m keen to get a baseline muscle measure of something that i can monitor over the decades but havent decided what’s best. (And so am about 4 years late to get a true pre rapa baseline!)
Hand grip could easily be rendered useful by future arthritis for example. Ditto dead hang times.
It is not perfect, but I judge how well I am doing with an exercise using an exercise frame. I am quite busy at the moment particularly because my wife is a local election candidate in Birmingham and that takes up quite a bit of my time. However, I aim to do an exercise routine every day. Depending upon how well I do I can judge how things are. I start with an extra 10kg on my legs.
In part I am aiming to lose weight at the moment so maintaining strength whilst losing weight is a good objective. There is I think also a cycling effect with Rapamycin, but I take it infrequently so I am not worried about that.
Today I was pleased to wake up at 79.2 kg which gives me a BMI of 22.2. I am reasonably strong (for a 66 year old) so a higher BMI would be sensible.
When i spend a lot of time delivering leaflets that can involve 25,000 or more steps and quite a bit of walking up and down steps (as well as bending down for lower letterboxes).
Good luck to your wife in the election. And good luck to you - I was co-opted into leaflet delivery for my father as a teen. I was always terrified of the dogs!
I am not surprised by these results. And I don’t think the correct conclusion is to adjust the regularity of your dosage down to the point that your strength gains are the same as they would be if you were not taking rapamycin at all. That to me implies that your victories against cancer may be equally diminished. Dose heavy, lift heavy is still the best strategy in my opinion.