" perhaps closer to 30mg [of rapamycin] every day or two equivalent in humans, per Adam Salmon interview ]"
from here: Breaking: 15% Healthy Lifespan improvement via Rapamycin seen in Marmosets
" perhaps closer to 30mg [of rapamycin] every day or two equivalent in humans, per Adam Salmon interview ]"
from here: Breaking: 15% Healthy Lifespan improvement via Rapamycin seen in Marmosets
That’s a lot! It makes me wonder if 9-10 mg every week is enough. ![]()
Its a balance… risk and reward…
as I said in that initial report on Adam Salmon’s announcement:
This new marmoset study suggests that a higher dose may be required for humans to get the same level of benefit, but with higher doses of rapamycin we tend to see higher rates of side effects (diarrhea, gastro-issues, etc.) and if higher doses are taking on a regular basis you typically get some level of immune suppression, and potentially some lipid and blood sugar disregulation; all of which tend to increase health risks in humans. So this may be the key challenge for human translation of this research, how to get higher levels of rapamycin into the blood system, while minimizing the undesirable side effects and risks.
I tend to agree with this. The long-term effects seem to be positive for skeleton and muscle while short term may be slightly detrimental especially if you are looking to build muscle. Looking at it in a more pragmatic way, I think RAPA will help/support the natural composition and muscle while not being beneficial if you want to artificially get bigger, if it makes sense at all.
I’m really curious the rationale here. This study was of old, untrained, people using an Exercycle and seeing how many times they can stand out of a chair. Looking at your profile photo, presumably you’re just a bit more active and capable than that ![]() And both groups did make gains - but the placebo group gained more. (Plus, as we both know, this is the “noob gain” phase when you start any exercise program. It’s pretty different to what happens 6+ month later.)
And both groups did make gains - but the placebo group gained more. (Plus, as we both know, this is the “noob gain” phase when you start any exercise program. It’s pretty different to what happens 6+ month later.)
IMO, unless you’re bodybuilding and need maximum gains, I don’t think this study is a strong deterrent. And if you were bodybuilding, common sense would have told you that mTOR inhibition would be suboptimal. We’ve always known that there’s somewhat of a conflict when it comes to maximising performance and longevity. You can probably maximise lifespan by calorie restriction, but you end up sarcopenic, or you can maximise muscle grown which comes with its own downsides. Or, you can find a sensible middle ground, which is what I hope to do.
I don’t quite get the logic here. Rapa might blunt the muscle protein synthesis, but it doesn’t negate all the benefits of exercise - the connective tissue strength, metabolic adaptations, the anaerobic capacity, stimulation of blood vessel formation, better nitric oxide etc. And even in this study, the people on Rapa still gained - just not as much as the placebo. So it’s not like lifting while on Rapa is harmful. It might just be slightly less beneficial than if you weren’t taking it.
I commend Brad for running the study. But IMO, the biggest problem is simply the short duration. When you start any new exercise program a lot of weird stuff happens. First of all, many people don’t make gains at all, because their body is just struggling to adapt to the new stimulus. So getting a 60 year old first-time lifter to squat the empty bar is going to make them mega sore, and they won’t gain much muscle. So the first few weeks typically actually have very few gains. Then, once you hit adaptation, you get a very rapid increase in session-to-session performance, and they can basically add weight to the bar every week. But that soon (couple months) starts to level off. That’s where the real magic happens IMO. At this point you need more myonuclei, more satellite cells, and you get lots of adaptations in the myocytes themselves - glycogen storage, they get better at glycolysis, they develop more pH buffer capacity, the mitochondria fuse together and become more efficient etc etc. Sadly, this short-term study is really only looking at the first part of the noob gains. I know that’s not Brad’s fault, but it is a limitation for our interpretation and whether it’s relevant to our own situations.
I don’t know of reason to think short term exercise strength gains can be correlated with long term longevity. By that model steroids and excess calories would look great.
You raise some very good points. My initial knee-jerk reaction to the results was to stop because of the muscle interference it causes but upon further reflection, I think I might just reduce the dosing frequency instead. Perhaps a larger dose once a month and then not lift weights for the next couple of days. Still trying to decide. It is still just as important to me to be strong and jacked as it is to live forever.
My thought too Luke… being younger and more athletic… a lower dose and less frequent for atutophagy and cell cleaning … repairing might be best.
That is basically the regimen I use. Mon/Tues/Thurs/Fri exercise, Sat take Rapamycin, Wed/Sun rest.
I took a 4 week break from Rapamycin recently and I did notice exercise improvements. I might look I to once every 2 weeks dosing for rapa going forward.
Depending upon the dose you need to assess when there is really effectively no rapamycin in your system. There will always be a teeny bit.
The central question is what level is actually significantly inhibiting MTOR. That is the study that needs to be done. Ideally, we all have access to very sensitive blood level testing and we have learn what levels correlate to actual inhibition.
Usually, we look at 4-5 half life’s essentially meaning no drug left in the system even though there is still some. So 10-12 days for Rapa. So getting 50/50 balance, not that this is the right ratio, would be taking every 3 weeks. At the same time, if 1 half life was enough to mostly stop inhibition, then every week would make more sense. Really, it would be 5 days but there would be some significant stacking of dose and level increase.
I do think the logic of younger people taking it less often.
And don’t body builders usually take long breaks in hypertrophy training? I am not up on their “science” which I put in quotes although I have respect for it even though they don’t really use the scientific method.
I am just starting. Had second 6 mg dose this week. I will probably do 3 months on and then take a break. Maybe start some TRT during the break. And by TRT, I mean a bit higher levels than average for my age - for some modest hypertrophy gains.
Nah. They do “blast and cruise”, so steroid cycle when on season and then TRT levels of testosterone to cruise in the off-season.
They continue training however.
I’m curious about this approach. I recall some people saying they strength train without regard to rapamycin dose timing. I can understand it would blunt training effects and healing, but does that mean we should avoid strength training during that period? I don’t know if we can say either way. I certainly feel weaker and more sluggish in the days after a dose during my training. Not sure if that means I should avoid it, take it easy, or go at my usual load.
Been taking rapa every other weekend 3days/3mg/day 9mg total. I’d been thinking about switching it up and now I will; 18mg per month, i.e. 6mgx3days in a row for 18mg. This will probably push me into ulcer territory for awhile at least, but that’s ok, I’ll know I’m getting some effect at least. And I probably won’t slack off on the exercise during that time.
Still thinking out loud here…
I’m still wondering the ideal day to take my dose and if I should consider every two weeks, but in the meantime, I was also thinking about the flip side of gaining more muscle and taking rapa less often.
I definitely don’t have enough muscle.
Having said that, I also know my strength has been increasing dramatically each month over the last two years since I started taking rapa (because I started focusing on resistance training, not from rapa).
Today I started thinking about everyone in my immediate family and extended family who has passed…
While many were frail at the end, they were frail due to diseases.
In learning how quickly one can lose muscle if we are limited, I’m guessing even if they had been extremely muscular when the diseases hit, over time they would have still become frail and their trajectory for passing or being independent would have been similar.
I guess this depends on your gene pool, but not one person I’m aware of had the privilege of living to an old age but had to move to a home because they were too weak to do anything becuase they had not worked out enough… they were too weak from ALS, cancer, parkinsons, or they just dropped dead from a heart attack.
My mom did break her hip at the end, but had she been a muscular stud prior to parkinsons, she would have lost most of it by the time she passed anyway. Had she not broken her hip, if it even made a difference, we doubt she would have lived longer than a few more months.
So, then I think about the potential benefits of rapa (fingers crossed). If it might keep me from developing any of these diseases, blunting some muscle would be an excellent trade off.
Obviously if one is lucky enough to remain disease free, I get that being strong enough to take care of yourself becomes incredibly important.
It’s hard to balance all the scenarios.
You are really lean… if I was as lean as you (of course I am male, so …) , I’d prioritize muscle for a while, and go on less frequent dosing of rapamycin (while doing more resistance training). As you age it will likely get harder and harder to build muscle, so no time like the present!
This is valuable feedback, so thank you for chiming in!
I have a 2 part question.
If I wanted to start every two weeks, and I take 8mg now, can you toss out a number I can experiment with? Would it be double? I realize you won’t want to tell me but your guess will be every bit as good as Claude’s ![]()
And then, as the next step, how do I check my labs. Meaning, I know that now I should check at a certain number of hours after my dose, and the sirolimus levels in my blood should be aprox 3 (can’t remember the unit of measurement off the top of my head)
How easy is it for you go get your blood labs done? I would start by testing your sirolimus blood levels 7 days after dosing just so you have a baseline from where you are now. Then perhaps every 2 or 3 days after that for a week to see how long you are at minimal levels.
For your body weight you take a pretty high dose… so it would be good to find out how your body is processing it over a two week period. You can either adjust the dose, or the frequency, or both. Your goal is probably to have at least a week of minimal blood levels during which you’re doing more resistance training to build muscle. Or perhaps 2 weeks?
Again, thanks for talking this through with me. I could pm at any time, but this might wind up being useful for someone else, so I’ll stay here unless you move this.
My prior 3 labs:
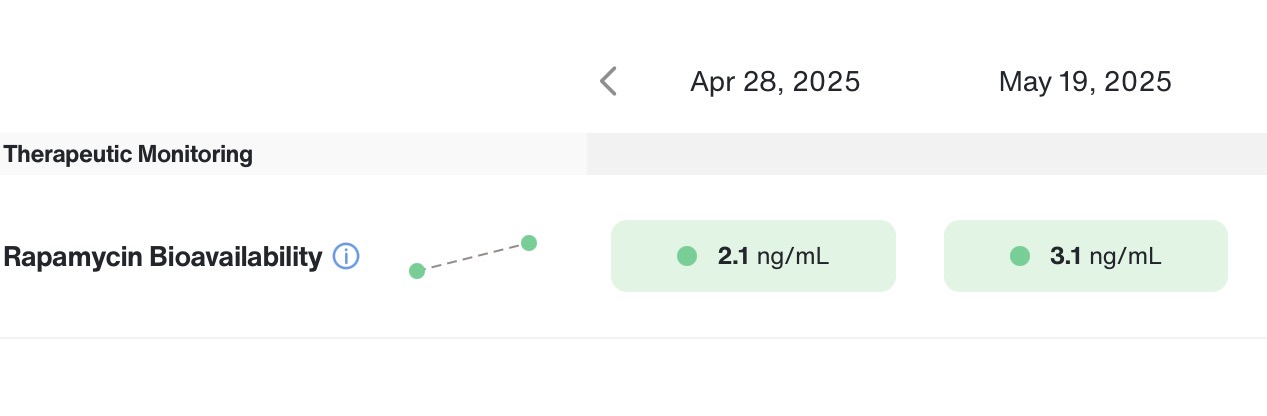
My first lab (after you we met and you told me to test!) was taking 6mg on a Saturday and then getting labs drawn on a Monday. My levels were 2.1 (shocked!)
Then, I raised my dose to 8mg, and my labs drawn on a Monday produced the desired result of 3.1
Based on my size, my doctor was also doubting I could be metabolizing it that quickly and he asked me to test 7 days later. This January, I had labs done on day 6, and I had no detectable levels
I know, it’s so weird that 8mg appears to be the right weekly dose.
I’ll start at every other week. During my off week I’ll add some extra RT.
It’s very easy for me to get labs when I don’t have to fast (otherwise it’s traumatic!)
I feel like I should take a higher dose if I’m going every other week, but what should my first stab at this be?
And I’ll share a workout schedule and if someone could advise which day would be ideal for my dose, that would help.
I always RT on Monday and Wednesday
I always have pilates on friday
On my off rapa week, I could add RT on Sat? I could really do it before or after my other RT days, but skipping a day might make sense?
I could add RT on every Sat too.
PS, because you’ve seen me, I’ll share I shockingly did my first one rep bench of 95 pounds this week! (And no, I can not bring it all the way down to my chest, so no comments from the peanut gallery ![]()
On day 6
Mondays on 6mg and then 8mg
Fwiw, because I have NO clue, I asked Claude opus and he said (I trust him as far as I can throw Dario):
Thinking through the PK from your three data points:
∙ 6mg → 2.1 ng/mL at 48h
∙ 8mg → 3.1 ng/mL at 48h
∙ 8mg → undetectable by day 6
Your apparent half-life looks like ~24–36h, which is faster than the ~62h population mean. One plausible explanation is a CYP3A4/3A5 or P-gp (ABCB1) fast-metabolizer phenotype — sirolimus is cleared primarily by CYP3A4 with P-gp efflux, and variants in either can meaningfully accelerate clearance. You haven’t been genotyped for CYP3A4/3A5 or ABCB1, so this is a hypothesis based on the observed PK, not a confirmed variant. Worth genotyping if you want to know, since it would affect dose translation for anything else CYP3A4-metabolized. Either way, it explains phenotypically why 8mg weekly is your sweet spot despite your size — you clear it quickly.
For Q2W, a reasonable starting range is 12–16mg, with 14mg as a clean midpoint. Reasoning:
∙ 16mg roughly preserves your current monthly AUC (32mg/month either way)
∙ 12mg is conservative — 75% of current monthly exposure, lower Cmax, lower GI risk
∙ 14mg splits the difference
Key PK point people sometimes miss: doubling the dose does not double the washout window. Half-life governs washout, not dose. So 16mg doesn’t wash out at day 12 just because 8mg washed out at day 6 — it washes out at roughly day 7–8 (one extra half-life). That matters for the Q2W framing: you’re buying higher peak inhibition and a longer guaranteed trough window, not “double the coverage.”
Testing plan:
1. Start at 12mg (conservative first trial)
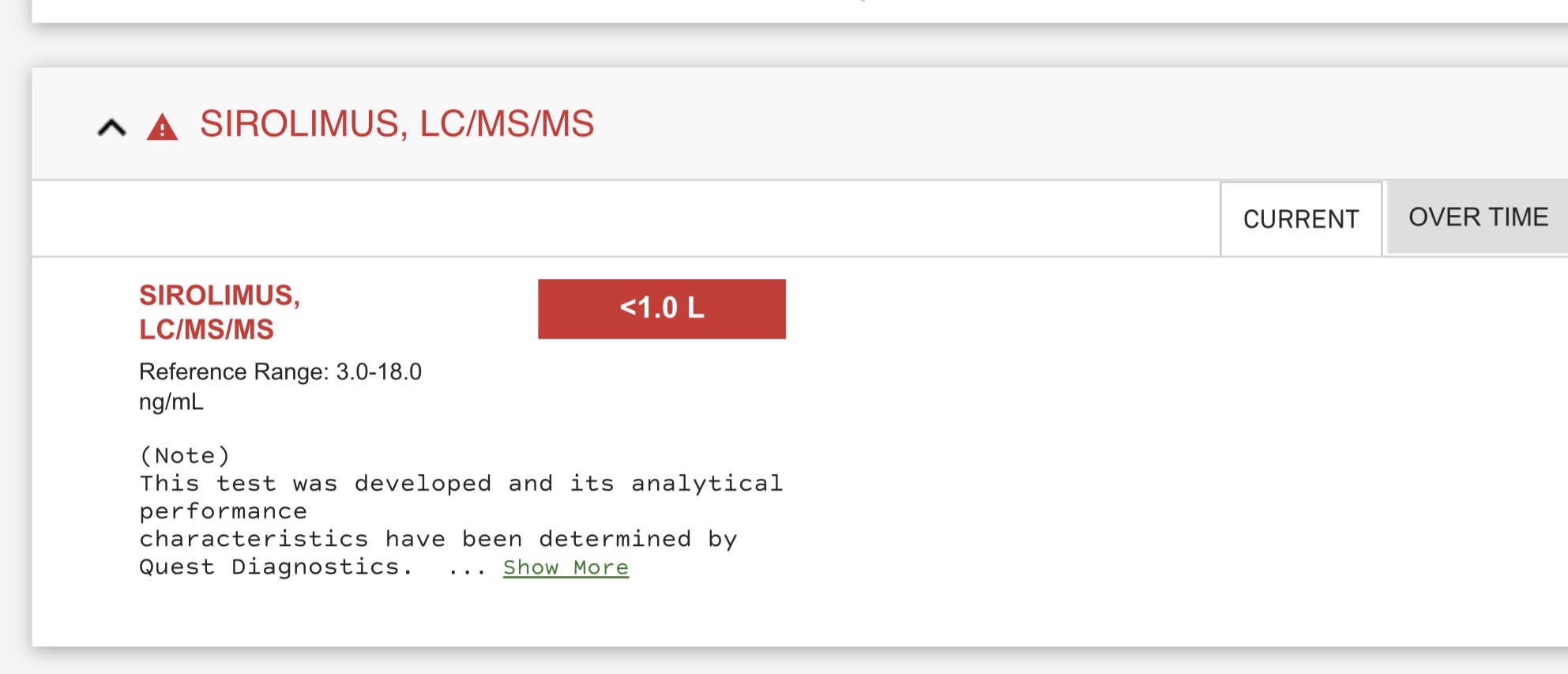
2. Draw sirolimus at day 14, right before next dose — target <1 ng/mL to confirm true washout
3. If tolerated and trough is clean, titrate to 14mg, then 16mg on subsequent cycles
4. Optional: 48h post-dose level on the 12mg trial to verify linearity (should be ~4.6 ng/mL if PK scales)
On dosing day for RT: With your Mon RT / Wed RT / Fri Pilates schedule and an added Sat RT, Thursday dosing is mathematically optimal. It puts both Monday and Wednesday RT sessions in the deepest washout window of the cycle (96h and 144h post-dose). Saturday dosing puts Monday RT at ~48h post-dose, right near peak mTORC1 inhibition — worst timing for your heaviest session.
Caveats: higher Cmax means higher GI side-effect probability (mouth ulcers, loose stool). Watch the first cycle. And the fast-clearance phenotype is worth confirming with one more PK