A little bit higher, but considering the inter person variability we’re really not sure how high it actually is.
I’m trying everolimus 4 mg mixed with rapamycin 4 mg . See what that’s like.
1 Like
With the super health of PA, not surprised this dose would likely not register any side effects. Although he said “he didn’t feel anything” on the podcast, wonder about his markers shifting some. He surely would NOT comment on any marker going worse…that would blow up his orbit.
I think his patient doses are far lower, very n=1 specific.
2 Likes
If anyone thinks they are on “high dose” rapamycin, consider this recently FDA approved IV injection for treatment of PEComa
- The recommended dosage of Fyarro is 100 mg/m2 (consider that in typical transplant setting, dosing is < 15mg/m2, albeit daily)
- Each infusion of FYARROtakes 30 minutes
- FYARRO is given twice during a 3-week period (this means you will receive an infusion once
a week for 2 weeks, followed by 1 week off - You can stay on FYARRO as long as your disease continues to respond to treatment or until your side effects require you to stop treatment
12.3 Pharmacokinetics
Absorption
Following administration of FYARRO at the recommended dosage, the estimated mean (%CV) Cmax and AUC0-inf of sirolimus in patients with advanced solid tumors were 2590 ng/mL (30% CV) and 22100 ng∙h/mL (50% CV), respectively.
You can see typical side effects here:
The company said the drug will be priced at a WAC of about $39,000 per month, or $468,000 per year.
2 Likes
This product information was posted 9 days ago.
Also in the same, was posted how it is manufactured.
2 Likes
This is interesting particularly since he is rehabbing from shoulder surgery. Clearly he doesn’t feel it impacts on healing…
Also I think it’s significant how much he minimises the benefits (and I think there are some else he wouldn’t continue). A total lack of hyperbole and in complete contrast to someone like David Sinclair.
The official pharmacokinetics for sirolimus show a mean half-life elimination (in adults) of 62 hours (range: 46 to 78 hours) which is extended in hepatic impairment (Child-Pugh class A or B) to 113 hours.
What does this mean? It means rapamycin has first order kinetics, so the rate of metabolism / degradation is directly proportional to its concentration. What does that mean? It means that for people who don’t have liver failure (in which case the half life would be so ridiculously long that it almost wouldn’t matter how you took it) that taking a given dose (e.g. 6 mg) once a week will result in a lower trough level at the end of that week than if you spread the dose out evenly. (Sorry if this isn’t totally obvious to you, but I can assure you that it is to anybody who went to med school and learned pharmacokinetics.)
3 Likes
Just to be clear, 6mg/week would result in a lower trough level at the end of that week than if you took 6 x 1mg/day? I would agree.
3 Likes
Transplant patients have no choice, of course, but outside of that space the closest I have seen to a recommendation for “daily” dosing was Dr. Blagosklonny saying “I see nothing wrong with a daily dose of 1 mg per day for 6 days.” But he went on to say “This is not very popular now. What is popular now is once weekly dose, mostly based on the right reasons, of course.” For what it’s worth, he seem to favor high doses every two weeks.
2 Likes
He did say a little later that he had recently switched to 1 mg every other day. But he had a specific reason that he did not want to share. So I guess it may depend on what disease you are trying to prevent.
5 Likes
@zazim - Thank you for the update!
It is interesting that Dr. B has always been the voice of a higher dose is now also seeing benefits of lower daily doses. I wonder if he had a health status change - possible a change in baseline labs. Seeing a bump in my liver function testing would make me do the same thing, but all conjecture on my part.
The 1mg every other day is what I settled on - but got hit with COVID and decided to hold for now. I did see some strong subjective changes on 6mg weekly. I really feel like one of the models that we may want to entertain is the concept of modulation mTOR1 instead of pulsed high doses to decrease the aging affect on mTOR1. in our youth, mTOR seems to modulate itself seamlessly without Rapa. - A treatment model that uses low doses of Rapa to mimic what mTOR modulation does in youth seems to be worthwhile approach.
Thanks again for the update!
3 Likes
He definitely didn’t recommend it for others. It was concerning that he had switched to that dosage. Virtually everyone would say that that is unwise and unsafe but he seemed to have a specific reason unrelated to general longevity (my surmise).
1 Like
There’s much to be said for low dosing. We have to remember that one of the most significant human response that we’ve seen is in the Mannick trial. The 20% increase in immune response was seen in the 5 mg per week group using the very short half life everolimus. Side effects were negligible. I don’t believe that the same effect was noted in the 0.5 mg per day group.
Immunosenescence is a major problem with aging and any intervention that addresses it is a big deal. It would be surprising if the benefits were somehow limited to just the immune system.
3 Likes
From the Mannick paper.
“In the intent-to-treat population, the low-dose RAD001 (0.5 mg daily or 5 mg weekly) cohorts, but not the higher-dose (20 mg weekly) cohort, met the primary endpoint of the study”
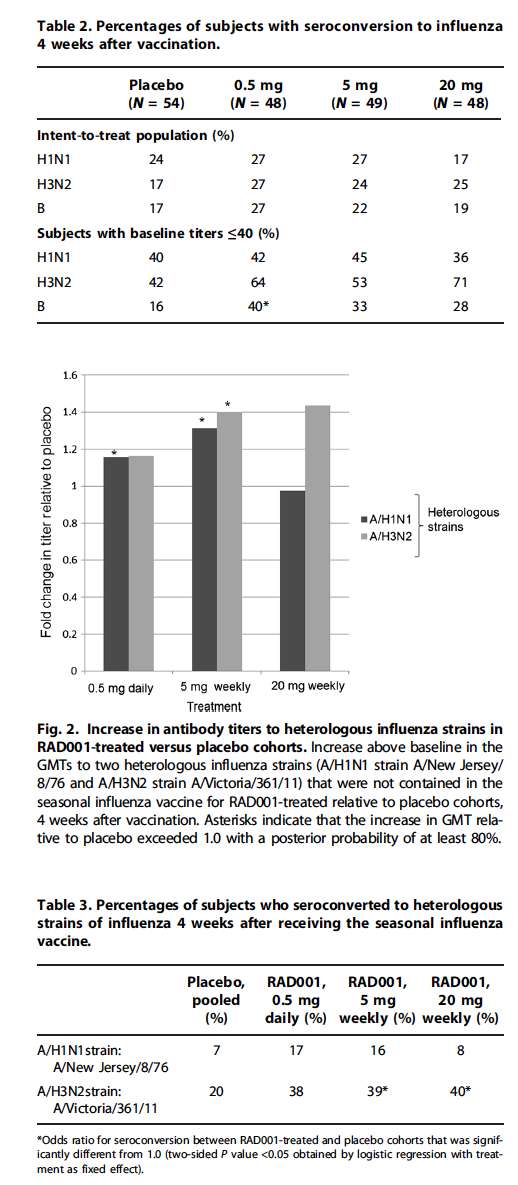
Some more insight from this paper on our dosing regiments/mTOR inhibition discussion:
"Modelling and simulation based on mTOR-mediated phosphorylation of its downstream target S6 kinase (S6K) predicted that the 20 mg weekly dosing regimen inhibited mTOR-mediated S6K phosphorylation almost completely, the 5 mg weekly dosing regimen inhibited S6K phosphorylation by more than 50%, and the 0.5 mg daily dosing regimen inhibited S6K phosphorylation by about 38% over the dosing interval (12). Thus, partial inhibition of mTOR-mediated S6K phosphorylation achieved with a relatively low dose of RAD001 may be as effective as nearly complete inhibition associated with high-dose RAD001 at enhancing the immune response of the elderly volunteers."
If you look up the reference 12, where the modelling is for CANCER (hmmm…they basically lifted a cancer model and used for the immuno study):
https://sci-hub.se/10.1200/JCO.2007.14.1127
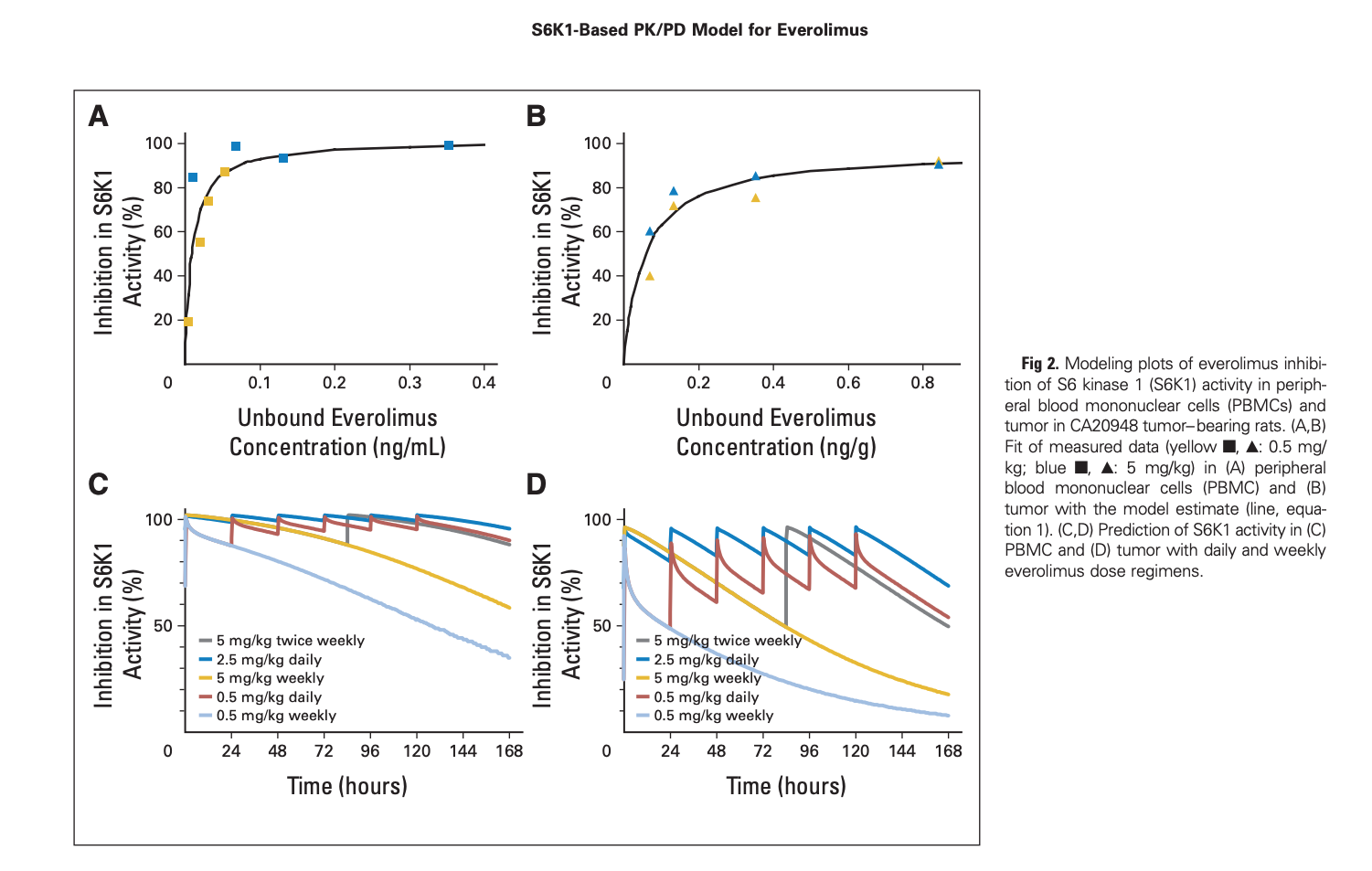
“Inhibition of S6 kinase 1 (S6K1), a molecular marker of mTOR signaling, was selected for PD
analysis in peripheral blood mononuclear cells (PBMCs) in a phase I clinical trial. PK and PD were measured up to 11 days after the fourth weekly dose. A PK/PD model was used to describe the relationship between everolimus concentrations and S6K1 inhibition in PBMCs of cancer patients and in PBMCs and tumors of everolimus-treated CA20948 pancreatic tumor–bearing rats.”
“Comparison of rat and human profiles simulated by the model suggested that a weekly 20- to 30-mg dose of everolimus would be associated with an antitumor effect in an everolimus-sensitive tumor and that daily administration would exert a GREATER effect than weekly administration at higher doses”
For Everolimus:
“This PK/PDmodel of S6K1inhibition has, therefore, provided an indication of which doses and regimens should be investigated clinically, starting at 20 to 30 mg/wk and 5 mg/d, respectively. The model predicts that such doses might inhibit the molecular target sufficiently to exert anticancer effects”
So there you go…one data point on daily vs weekly on a mTOR inhibition pathway of cancer.
You can see the S6K1 inhibition pharmacokinetics (daily vs weekly) in the lower 2 graphs in the image below. Rapamycin would of course have a different graph, but conceptually similar.
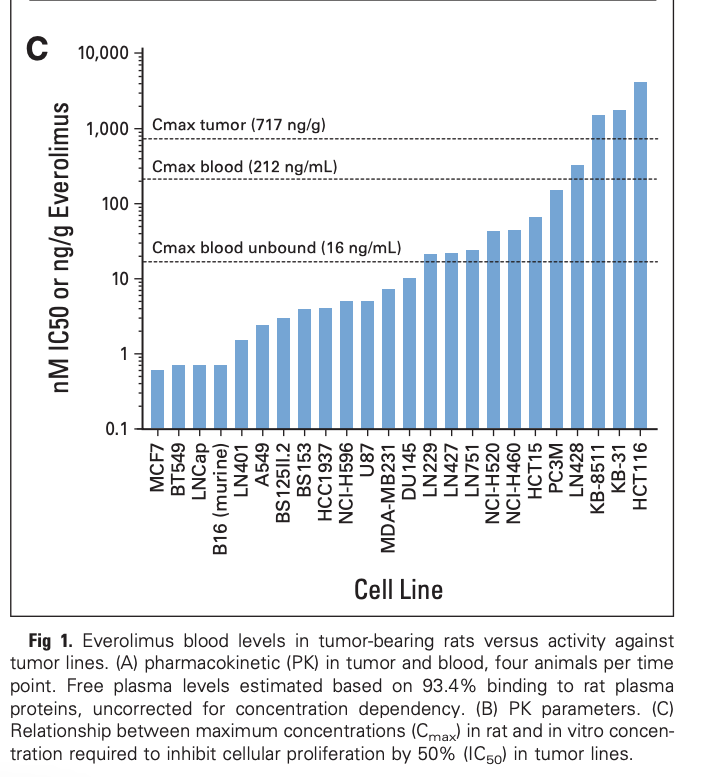
You can also see how Cmax is important for IC50, depending on tumour cell line. Intermittent dosing keeps hitting tumour cells with greater sustained IC50 via higher Cmax pulses.
It’s pretty to clear to me why pretty much every cancer/transplant study…dosing is daily to maximize cancer inhibition, and side effects…as “much as can be tolerated”
1 Like
So - using the imperfect estimation of rapamycin comparable doses (50% to 80% of Everolimus) from the Lloyd Klickstein interview (below) - that should map to approx. 10 to 24mg/wk, and 2.5 to 4mg/day.
So - in the immune suppression / mTORC2 inhibition range. Obviously risky…
perhaps the optimal dosing program is higher rapamycin doses during times when a person is well-isolated and lower risk of pathogen exposure, and lower doses when more socially active?
Was just reviewing an interview with the Novartis exec Lloyd Klickstein who was involved with the everolimus tests and the research papers related to this topic. In the interview they mention what they believe is the dose equivalency of everolimus to sirolimus / rapamycin - see below:
In one experiment. Patients with polycystic kidney disease that were otherwise healthy, took the rapalog (RAD001) and a substantial fraction saw these biochemical changes in their blood
- The dose was 5 to 10 mg a day (equivalent to 2-8 mg of rapamycin)
2 Likes
Are you referring to humans? Seems impractical. Being socially active is not negotiable.
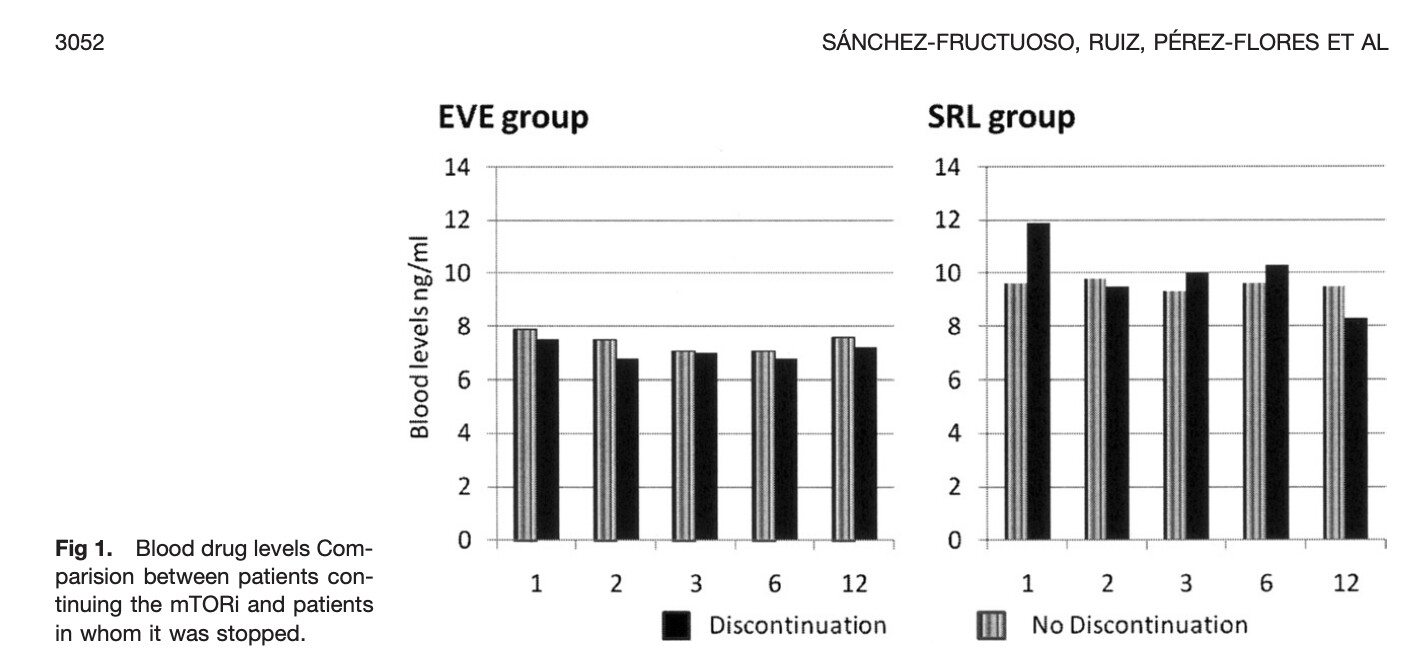
Regarding this “theoretical” bio-equivalency of Everolimus needing 2X dose vs rapamycin, not so sure. A renal transplant study comparing the two.
https://sci-hub.se/10.1016/j.transproceed.2010.07.083
“The initial mean dose was 2.95mg/day EVL and 3.61 mg/day for SRL”
Yet they delivered the same approximate trough levels?
Clearly, it’s all n=1 dosing exploration…YMMV.
Great discussion Thread!! it almost feels like you guys are cracking the code.
@RapAdmin I believe you posted something on the Rapa scientist that used 1mg / day to stave off his stage 4 colon cancer. He must of had his reasons for a daily low dose.
@MAC Your arguments for higher doses creating more cancer / tumor inhibition should be seen with renal transplant patients? You may have run across that comparison in your extensive reading.
Thanks guys! I learn something everyday.
2 Likes
The most beneficial results for rapamycin in mouse studies has been high doses. Full stop. Unless something has changed since June 2022. I don’t think there’s any support for daily dosing absent unusual circumstances.
4 Likes
There are mtorc2i studies for cancer in transplant pt, mentioned it before
1 Like


@David, these are long, but if you haven’t seen either of these webinars, you will get a lot of helpful information from 3 of the best in this field, Dr. Green being one of them.
4 Likes
Generally yes, higher daily doses results in higher trough/AUC, and better cancer and renal rejection outcomes, but more side effects.
2 Likes