After a few months of being on this site and listening, learning and questioning, I have decided to change up my dosing from 6mg of Rapamycin once a week to 1mg once a day x 6 days and one day off. I am hoping this helps mTOR1 go back to a more “youthful” modulation with less peak and trough variations. I will check a Sirolimus level in 2 weeks 2-3 hours after my 6th dose of the week. I would appreciate any comments, suggestions, discouragements or whatever from our talented Rapa Newsy members to help everyone learn a little bit more.
7 Likes
That’s an interesting decision. It seems like you’re trying to be in some sort of a steady state, but with the long half life of rapamycin you’ll never hit a trough, so there won’t be a recovery time ,and your levels may get quite high, similar to transplant patients.
For what you want to achieve , it might be better to use everolimus with its short half life, possibly every other day. You’ll still get the desired troughs.
9 Likes
Wouldn’t you have similar results to transplant patients? How does rapamycin affect them? I would assume we should have a wealth of information on this as they constantly see doctors…
Great points! 1mg of Sirolimus per day should be sub therapeutic for transplant dosing. if you ever type out a 1mg daily dose on an EMR e-script - you get a warning that the dose is consider subtheraputic and to consider 2mg or higher.
I believe that the peak levels are where you get much higher mTOR 1 inhbition and trough levels are not going to be high enough for mTOR2. Since mTOR 1 is not completely inhibited and I will continue to do my mTOR stimulators - exercise, TRT and protein supplementation, then hoping for a balance or more youthful modulation.
I am trying to use a negative feedback loop approach ( since that is a mechanism I understand) although I don’t think fits perfectly. Pulsed doses unplug the heater from over heating the house - house cools down to normal temperatures vs. more steady low dosing that would hopefully restore the thermostat regulation / modulation to restore the temperature ( sorry, probably lousy analogy )
Thanks your your valued repsonses since I am trying to put my arms around the MOA of mTOR modulation of youth vs. the dis-modulation of age.
4 Likes
Here’s a very interesting editorial on low dose rapamycin prolonging lifespan while reducing side effects. In fact, you’ll see that they reference a Two Fold increase in longevity using low doses. This is separate from the cancer inhibition that is uniformly noticed.
This begs the question, what’s a low dose and how do we best get there? Your approach of daily low dosing is certainly interesting. Please keep us posted.
5 Likes
@rivasp12 Thank you!
Exactly the information I was hoping to get and also have the same questions - Can we get away with 1/2 mg per day or every other day dosing.
In my experience with hormone replacement, most side effect issues happen in the peak windows and most symptom control break through in the trough levels.
Everyone seem to have good reasoning for their approach of taking every week vs. biweekly, but then after making our points give in to the fact that we are all guessing based on mice and dog studies for longevity and safety profiles from transplant patients.
My first goal is aging symptom control ( Health Span) with minimal to no side effects. Obviously longevity would be nice, but better human data needs to be collected.
Thanks again!!
5 Likes
I am looking forward to the results of your trial. My thoughts as an unqualified medical or biological expert:
As an engineer, I really like your negative feedback approach.
It is not known exactly how much rapamycin suppresses mTORC2, but I do know from experience that high doses do. High doses also increase cholesterol levels.
Two very positive effects I think you would get from your low dose regime are; reduced or no rising of lipid levels and low or no reduction in mTORC2.
My personal experience is that you can tell when mTORC2 is suppressed because minor wounds such as paper cuts, hangnails, etc., are slow to heal.
I am in a quandary about what dose regimen to follow when I start taking rapamycin again.
I may follow your example for a while and see what my blood work looks like in a couple of months.
Quoting from the paper “rivasp12” referenced:
"The positive effect of low
doses of rapamycin on longevity in the follow-up study
supports previous observations. The most important
advantage of the new study derives from the significant
reduction of the dose used."
2 Likes
Yep, that’s all of what I am hoping. I am sure there is an answer of when we decided to use pulsed dosing over normal steady state dosing that is more common. I like Sabatini’s explanation of mTOR2 is not directly blocked by Rapamycin. It blocks the mTOR part of what makes mTOR2 at the assembly stage. So hopefully, lower doses and would help avoid it or only partially block it ?
Thanks for your perspective from an engineering back ground.
2 Likes
Another positive effect of low steady dosage as opposed to high peak periodic doses:
You would not experience the negative side effects from high pulsed dosing, such as,
temporary loss of immunity, fatigue, etc.
Yep! I was hoping to not worry about when I work out while I am taking it. Many people on this site avoid working out 2-3 days after their Rapa dose.
1 Like
I would recommend listening to Peter Attia’s podcast episode #118, where they discuss rapa dosing.
Long story short, unlike other drugs, rapa’s side effects come from the trough level, not the peak level. Therefore you want to space out doses so that the trough has a chance to reach a very low level to reduce side effects. I assume that’s why people have landed on once a week (or two weeks) dosing for now.
Also, rapa does not block mTORC2 directly. mTORC2 may be affected indirectly if mTORC1 is inhibited too much through a feedback mechanism. Therefore, it’s important not to inhibit mTORC1 too much if you don’t wan to affect mTORC2.
3 Likes
I would note part of the rationale of higher pulsed dosing vs continuous - particularly in older people (somewhat leakier) vs 1 in 4 with APOE4 carrier (which is why Dr. Green recommends patients for WGS) - is blood-brain barrier uncertainties. (I’m aware of that brain tumor study - but it’s still an uncertainty)
It’s not just mTORC1 vs mTORC2.
Getting CVD/cancer down but not dementia isn’t that appealing to me frankly. “Brainspan” is a big part of “healthspan” to me.
6 Likes
Ideally someone “healthy” can synthesize 11-C radiolabelled rapamycin and do a ultra low dose PET scan (or if they were going to need a craniotomy anyways to check rapa levels) - it would be nice to have frankly.
2 Likes
Thank you! I admire Dr Attia as true innovator and I will check it out.
Right now everyone is spit balling it on how to approach dosing. If you get a chance and look at Dr Kennedy’s video on how mTOR never really is fully inhibited and that the goal may be more of modulation of mTOR to make it more flexible as in your youth.
I think I am going to check a peak and a trough level
Thank you so much for your comments.

1 Like
@David - Thanks for the video. I’ll take a look.
By they way, rapa only inhibits mTOR partially, not fully.
You’re right, we’re all guinea pigs here and nobody really knows without clinical trials.
I think you can calculate the trough level of a 6mg weekly dose vs. 1mg daily dose for 6 days and see which one gives you a lower trough.
I suppose there are 2 variables that can influence the trough level, your initial dose (if you do it intermittently) and how many days between doses. There’s nothing magical about 7 days. We use it because that’s how our calendar works. But maybe 8 days is better, or 9. Certainly the longer you wait between doses, the lower the trough, and likely lower the chance of side effects such as higher lipids and glucose.
A gap in the literature is ATP competitive mTOR inhibitors. So we can’t even say whether mTORC2 is “bad”, even though a lot of people here are saying that.
There’s enough overlap with mTORC1 that it may be part of the effect. It’s an unknown, but we start putting “good” and “bad” labels on things without knowing at high certainty whether the potential effect may be lowered.
The best argument I currently have for what many are thinking is mTORC2 = side effects = bad - but that’s not strong enough for me.
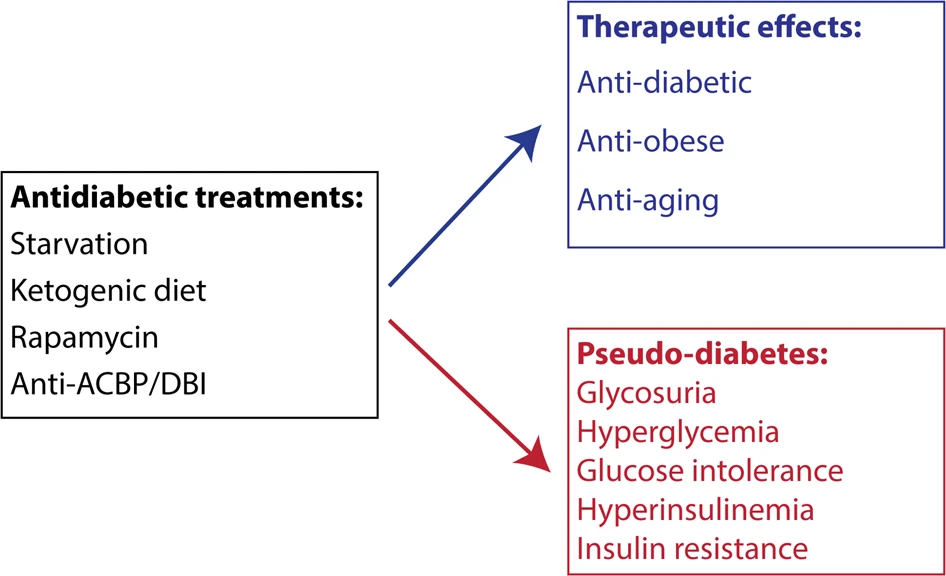
For example, there are plenty of researchers who say mTORC2 inhibition = decreased glucose tolerance, thus rapamycin causes diabetes because they are parroting this article.
But I see it as data misinterpretation. Sounds more like “benevolent pseudo-diabetes” similar to fasting state.
All valuable points!!
I am using Health Span variables as my end point for now. I would love to live longer, but not my primary objective. I am not sure if you are on Rapa, but my primary observation has been a significant decrease in age related symptoms. I am 58 y/o and despite a healthier approach to life with diet, exercise and sleep have experienced the progression of aches and pains from being on the planet longer. My first clear confirmation of Rapa’s value has been, resolution of low back pain, faster recovery from exercise and no joint inflammation pain than I have had progression of for many years. Dr. Kennedy’s point is exactly what you made that mTOR is never fully inhibited.
Thanks again and I look forward to your input in the future.
2 Likes
@David - Thanks for your kind words.
I’m 46 and I’ve only been on rapa for 1 month (4mg a week; 2mg the first dose). I got a prescription from Dr. Green. I’m taking rapa for an autoimmune condition, so any other health span or life extension benefits would be icing on the cake.
Even though it’s only been a month, I had improvements in my autoimmune condition with every dose. So yes, rapa works! It’s a miraculous drug. Rapa probably can be used to treat a lot of diseases, but it’s a shame that nobody wants to do clinical trials because there’s no money in it as it’s off patent.
Since you mentioned David Sabatini…it’s so sad what happened to him. I hope he can come back someday. Otherwise, it would be a great loss to the scientific community.
1 Like
Oh gosh, I have not heard anything about him! Positive thoughts for him whatever his challenges.
Autoimmune issues used to be a rare issue in medicine and now many people have some issues that can be traced to it. Diet, exercise and sleep are great places to cultivate. Low inflammatory diets and depending on your tolerance levels, supportive treatment with hormone replacement and even off label thyroid approaches. Wish you well on your journey!
3 Likes
There is very significant inter patient variability in the pharmacokinetics of rapamycin. In this study in Iran they were checking on what kind of dose would achieve the trough levels of 5-10 ng/ml necessary to be immunosuppressive.
That dose turned out to be only 1.2 mg per day! Certainly that isn’t your goal so I’d be quite careful here. It’s nice to have the TOR debates, and theories are fine and dandy, but immunosuppressed renal patients is a real thing.
3 Likes