Thanks for sharing, I had not seen this study before and it’s very insightful.
The paragraph that @desertshores highlighted is also the most significant one for me. It tallies with my anecdotal experience (from cycling) that rapamycin inhibits adaptation to endurance exercise. This was most noticeable when I briefly went up to 10mg/week which would have led to trough levels of >1.5mg (equiv).
Assuming a 62 hour half life and a typical 6mg/wk dose, trough levels only drop below 1mg (equiv) for 12 hours.
Actually an extremely thorough study re biomarkers, and great 1mg/week reference! Arguably, more aggressive than Mannick 2014 using Everolimus at 0.5mg/day or 5mg/week.
Although only of very short duration, generally no big new negative effects especially in the context of the old age cohort. Small increase in TG and TG/HDL, and barely much change in A1C. They likely had an initial dip then recovery re markers…argues to wait some time before doing a blood panel to reassess.
Re inflammatory cytokines:
“No statistically significant RAPA (or placebo) effects were seen in serum cytokine levels. However, it was noted that for one pro-inflammatory cytokine, TNF-α, more than half of the RAPA treated subjects showed increases and the remaining individuals either maintained or had very small declines. The placebo group had a more disparate profile showing the typical heterogeneity seen with serum cytokines”
Rapamycin dosing
“The treatment group received a daily dose of 1 mg RAPA and their blood levels were analyzed at intervals thereafter. The highest concentration attained for each subject is shown in Table 2; the levels varied from 2.5–11.8 ng/ml. Subjects received either 1 mg of RAPA daily (or placebo) with resultant plasma levels of 7.2± 2ng/ml”
Quite the range inter person. I don’t discern in Table 2 the actual time point of RAPA draw relative to dose, but since it’s daily and long half life, this is a fairly high average rapa level…certainly in the context of say a much weaker 7mg/weekly mathematical linear equivalency. Namely, I would say the average (daily level/7) rapa level in a 7mg/week would be MUCH lower than this 1mg/day average.
So…1mg/day with less lipids/glucose dysregulation than high dose weekly/bi-weekly, albeit old cohort??
I would agree, I think it would impact PEAK endurance exercise for sure. But 99.9% of users are not concerned with maximal or high output exercise detriment.
You have NO idea your n=1 kinetics unless you do trough and Cmax exploration Sirolimus tests.
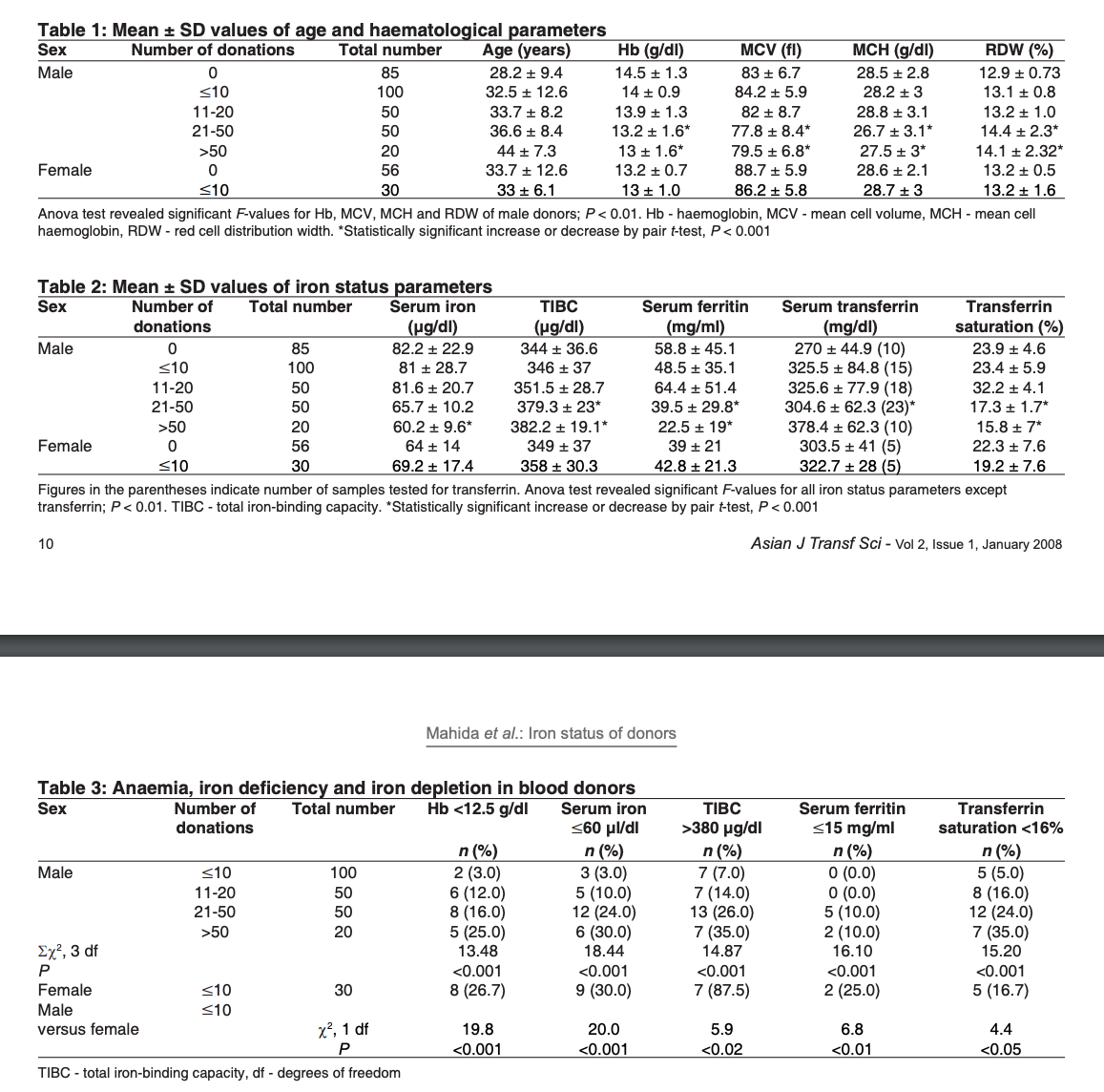
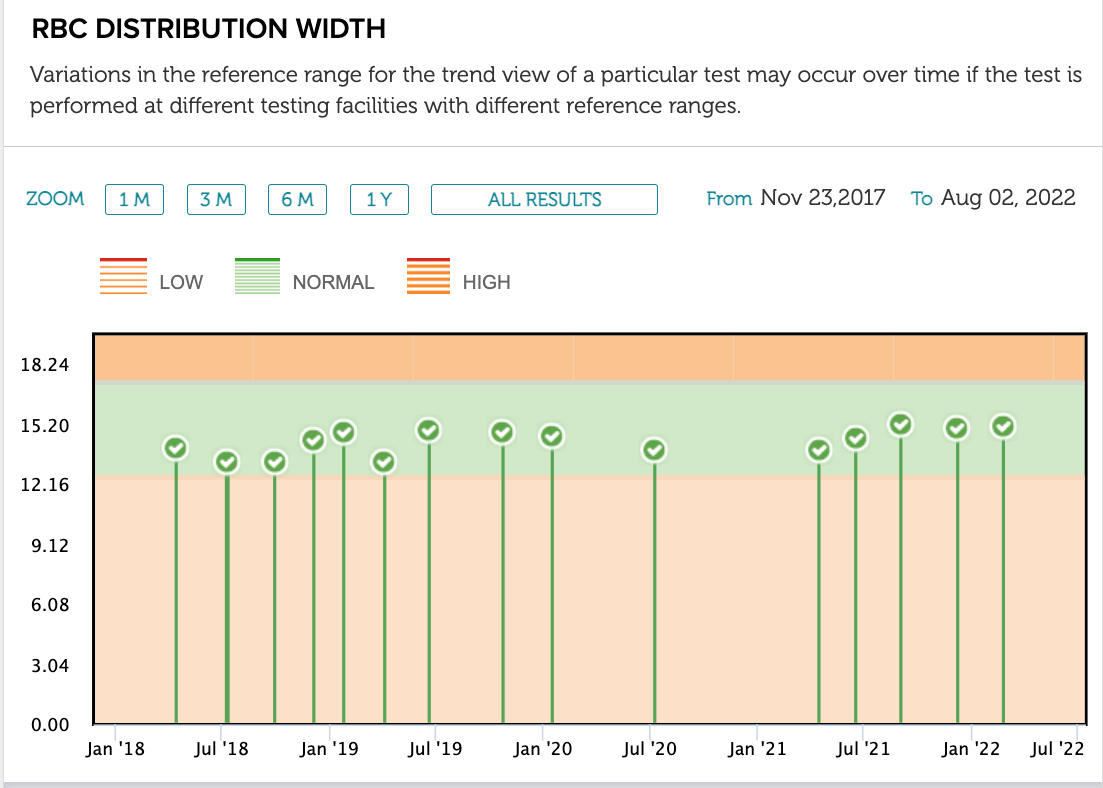
Looks like blood donation increases RDW, so penalizes one in the Levine phenoage, although its clearly a confounder…not rooted in some metabolic aging disorder. So is rising RDW via repeated BLOOD DONATIONS a bad thing? But lowering RDW via Rapa a good thing…only to satisfy a mathematical clock?
These Levine things aren’t done with rapamycin in mind or in any way accounting for that kind of intervention.
Rapamycin leads to smaller hematopoietic stem cell size which makes them healthier, more efficient, and longer lived. Of course, when you donate blood, old cells are being replaced by newer and somewhat larger RBC’s so it will skew the RDW reading a little bit. It’s still a great thing to do along with rapamycin.
Sorry, I didn’t know that giving blood increases RDW. I made the erroneous assumption that making new blood cells would reduce RDW without doing a search. Apparently, there is also an association between iron levels and RDW.
No, I have not had a CAC score. I am 81 yrs old and I don’t think that I could do anything more than I am doing. Fortunately, I am in very good shape at this stage of my life and I don’t think a CAC test would be of any particular benefit to me.
I’m just going to keep on tweaking the supplements, etc that I use based on new information as it becomes available.
No idea how they’d tweak, when there is no underlying basis (large data base) for a singular rapamycin intervention.
I might argue, that if you’re doing interventions that have very strong anti-aging studies support, and they confound the biological age tool (uses raw large population epidemiological data)…perhaps dispense with it entirely or do not use it SOLELY?
The fact that RDW is so massively weighted in the Levine clock, and donating blood is HUGELY associated with positive health outcomes, it’s quasi useless to me.
The albumin, glucose, ALP, creatinine, hsCRP…we already know which direction is generally positive association.
And the fact there’s no lipids markers…lack of data power, or does it TRULY believe TG, TG/HDL, APOB, LDL is meaningless to longevity? I do NOT believe that.
Here’s just a few studies (there are many!), using same NAHANES III data pool as Levine clock, using different INPUTS and analysis for all cause mortality outcomes.
“Multi-systemic biological risk (MSBR), a proxy for allostatic load, is a composite index of biomarkers representing dysregulation due to responses to chronic stress. The sample included n=13,628 adults aged 20–90 from the NHANES III Linked Mortality File (1988–1994). .The MSBR index included autonomic (pulse rate, blood pressure), metabolic (HOMAir, triglycerides, waist circumference), and immune (white blood cell count, C-reactive protein) markers. MSBR is positively associated with risk for cancer mortality in a US sample, particularly among those who are overweight or obese”
“We observed an increased risk of all-cause mortality associated with higher levels of serum C-reactive protein, thyroid stimulating hormone, lactate dehydrogenase, gamma glutamyl transferase, and plasma fibrinogen, and urine albumin. In contrast, higher levels of serum sodium, alpha carotene, and albumin were associated with a decreased risk of all-cause mortality.”
“A score based on serum concentrations of C-reactive protein (CRP), albumin, gamma-glutamyl transferase (GGT), and HDL cholesterol was positively associated with death from cancer, circulatory disease, and all-cause mortality. Baseline measurements of CRP, albumin, GGT, and HDL were available for participants with mortality follow-up (n=13,056). A biomarker score, ranging 0-4, was created by adding number of markers with abnormal values (cut-off: CRP>10mg/L, albumin<35mg/L, GGT>36U/L, HDL<1.04mmol/L). Its association with mortality was analyzed with multivariate Cox proportional hazards models. The score was positively associated with death from all causes, cancer and circulatory disease. These findings correlate with results from a Swedish study”
“The purpose of this study was to evaluate the associations of serum biomarkers of fruit and vegetable intake (vitamin C and carotenoids) with cause–specific mortality and all–cause mortality in a nationally representative sample of US adults. We analyzed data from 12,530 participants from the National Health and Nutrition Examination Survey III (1988–1994). Inverse associations were found between serum vitamin C, carotenoids, and composite biomarker score and outcomes expect for cerebral disease, heart disease, and cardiovascular disease mortality.”
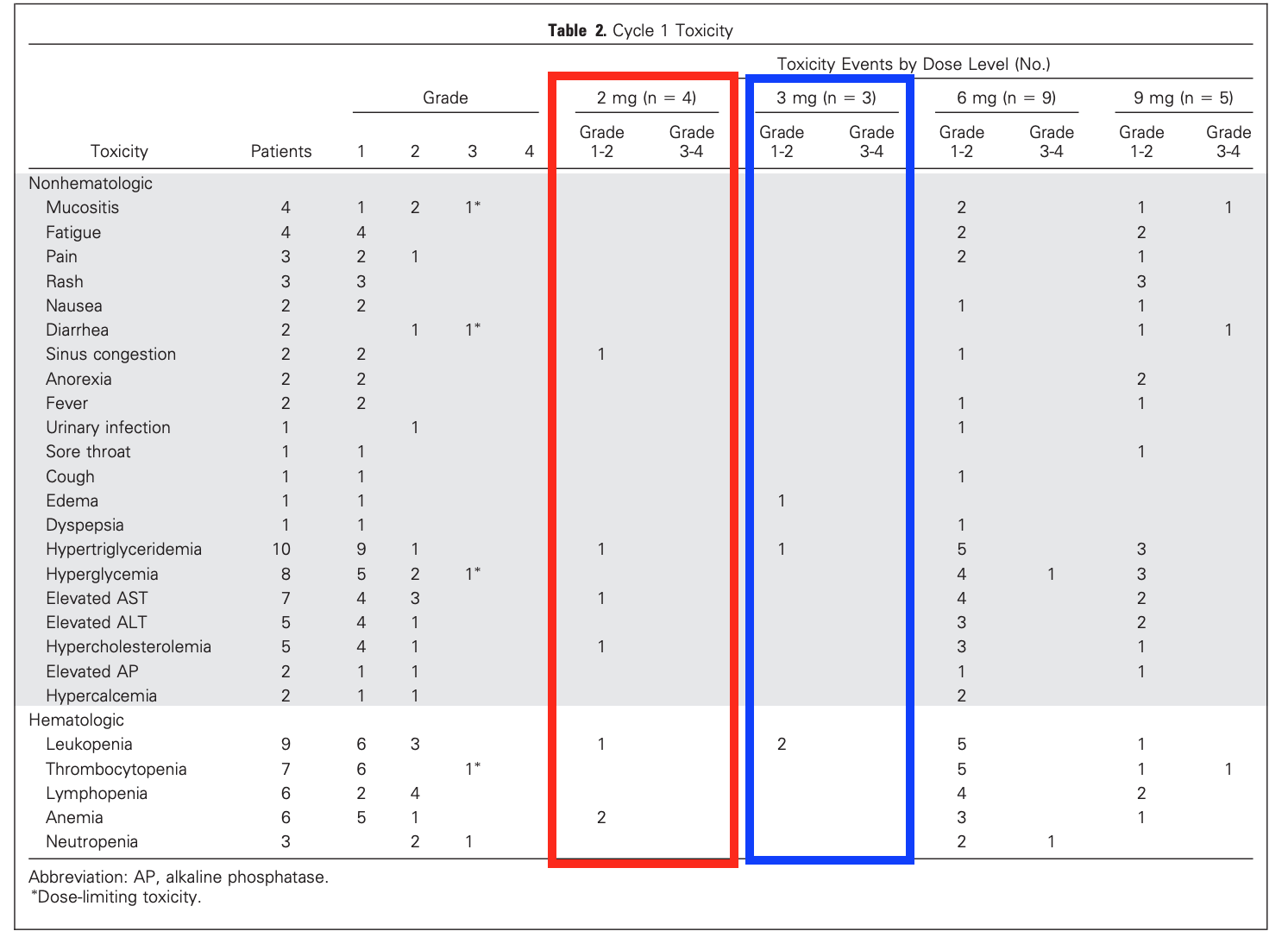
Looks like 2 and 3 mg/day were well tolerated with minor side effects. Of the 7 people in this cohort, only 2 hypertryglyceridemia Level 1, and no hyperglycemia.
Of note, in the higher dose groups (6 and 9mg/day) with higher toxicity levels: “Hyperlipidemias responded well to statin treatment”. So whether simply standard of care, “benevolence” was not an option.
Also, “by assessment of pretreatment trough concentrations, steady state was reached by day 8. Accumulation was noted since there was an increase in rapamycin exposure (Cmax; day 1AUCinf vday 28 AUC0-24 hours) between days 1 and 28 (P.05; Fig 2A to 2B)”
So there was an accumulation of rapamycin even up to 28 days (4 weeks).
The leukopenia could be significant, but probably not without the neutropenia. Rapamycin inhibits T cell proliferation and T cell induced leukotrienes, which are inflammatory mediators like cytokines. This allows for an introduction of an antigen, such as a new organ, without rejecting it. That’s good for them, but I’d need to be certain that daily administration isn’t doing that to me.
This is way beyond my pay grade, but are there any clinical examples of constant immune suppression and long term outcomes?
Immune injury associated with poor outcomes…
"The authors found that immune dysregulation (defined as having CD4/CD8 < 0.70) was common among participants virally suppressed on ART, and for the most part persisted over time. Further, an inverted CD4/CD8 ratio appeared to have clinical consequences beyond HIV, as baseline immune injury was positively associated with cancer and death
…but prolonged HIV suppression may reduce risk
However, the authors also found that with prolonged successful suppression of HIV, CD4/CD8 improved, likely reducing the aforementioned risk. CD4/CD8 values and percent of participants with CD4/CD8 ≥ 0.70 increased within each age group (P < 0.001 for all), suggesting that immune injury may recover some over time
Ultimately, although years of viral suppression may diminish the risk of comorbidities and death, the effects of aging and immune senescence appear to be deeply rooted, curbing a patient’s long-term ability to restore immune function."
We’ll, there’s cyclosporine which decreases T cell function like rapamycin but is much nastier in my opinion.
It’s also used for organ transplants. Also used for autoimmune diseases where rapamycin also looks promising. But look at the side effects and you’ll appreciate rapamycin
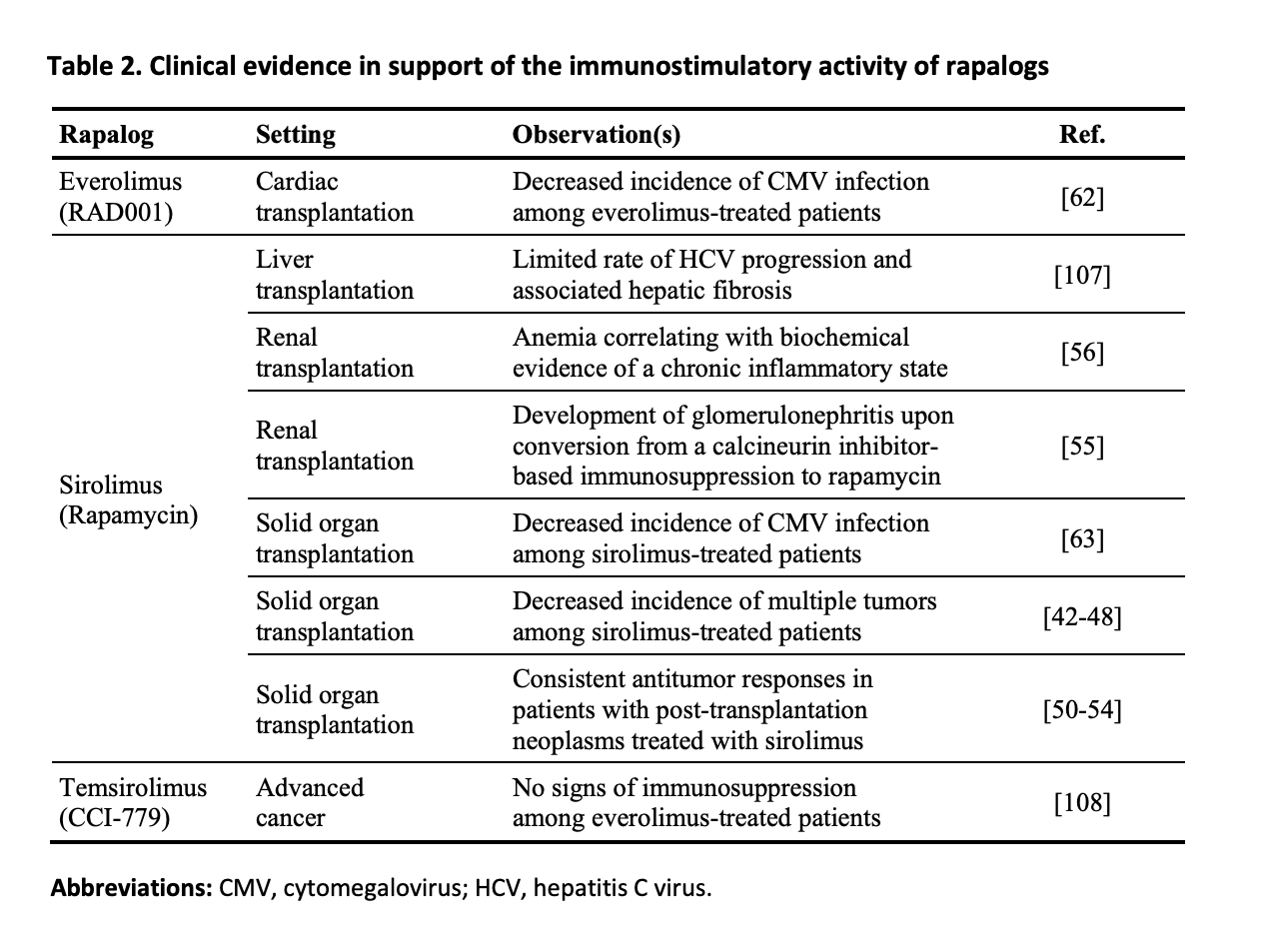
Here’s a very good review paper on the immunostimulatory effects of Rapamycin from 2013, a year before the Mannick study with Everolimus, showing significant improvement in immune function (elderly cohort).
My sentiment is still full steam ahead with extreme diligence, especially escalating dosing.
Immunostimulatory activity of lifespan‐extending agents
“Although such a beneficial (and completely unsuspected) activity of rapalogs was initially ascribed to their capacity to robustly inhibit the mammalian target of rapamycin (mTOR) complex 1 (mTORC1) in cancer cells, accumulating preclinical evidence indicates that the therapeutic and oncopreventive effects of rapamycinlike compounds originates, at least in part, from cancer cell-extrinsic mechanisms that involve the immune system. Taken together, these observations suggest that rapamycin and other rapalogs are capable of stimulating, rather than inhibiting, immune responses, at least under selected circumstances. Whether such an immunostimulatory function truly underlies the antiaging effects of rapamycin remains to be formally demonstrated”
On the topic of dosing, for what its worth, here is the latest update on what dose Peter Attia is taking of rapamycin per week (it would be interesting to know if he prescribes that high with his patients).