You are correct! I guess it helps to define what is the standard. I am using Dr. Reedy generic form. I tried a compounded form, but subjectively noted symptom changes and switched back. I am guessing to find the sweet spot that would be to do an QOD vs. cutting dose to 0.5mg QDAY?
I really appreciate you input! Just trying to Rubik’s cube this together.
i need to see where I can get everolimus, but like the lower half life and appreciate you pointing that out. Other options would be to take vacation/ holiday periods to allow everything to reset? I just put the day off on the 1mg / day due to my 6 mg doses that created a better math equation to just take a day off. My approach for now is Safety - based on labs and side effects and then QOL health span improvements. I am pretty healthy for my age related peer group, but don’t want to get cocky on what I risk and appreciate the input you have given with your literature and clinical back ground. i don’t take it as medical advice and full responsibility for my decisions
Haha! You are making me think trying QOD dosing may be smarter and less ballsey I know Rapa is different, but not many medicines are safer give in one big dose vs smaller spread out doses. Again, appreciate the conversation.
“There’s nothing magical about 7 days. We use it because that’s how our calendar works. But maybe 8 days is better, or 9.”
Amen to that.
Rapamycin testing is inconvenient for me, as apparently, only Labcorp is offering it.
For the time being, I will rely on the trough levels of others who get their levels tested to get a very, very rough estimate on timing. No one knows what their actual dose is unless they can get a max or near max reading from Labcorp because even with an appointment you never know exactly when they will see you.
You can calculate the max dose taken from your Labcorp test, but again it is just a rough estimate.
Totally agree. We forget that time seems to be our invention to feel better and that the universe does what it does not based on the hands of a clock.
I may be in trouble with the lab part since I have Quest Labs in my office and just assumed I could use them, but will see what I can work out with Labcorp.
I am curious on how the labs influence what we do? What if you feel great on one peak/trough that seem to NOT be ideal or feel lousy with ‘ideal’ levels - whatever those are? It took me years of being untrained to allow for the patients input to be one of the most important variables - this is more true for health span medical approaches than disease based approaches -
So, this great!! We all get caught up in the dogma of what we crown as the “rules” and then realize that we came to conclusions looking through one set of optics.
What happens if we stimulate mTOR 1 and mTOR2 at the same time we slow it down? Does this create chaos or allow better modulation - my poor mans explanation with the negative feedback loop as in the thermostat modulating the temperature - heater kicks in when to cold and air conditioner when to hot. Is this concept of both availability of mTOR inhibitors and stimulators at the same time very similar to what happens in youth?
To your main point. Just because we change a number to an ‘abnormal’ level does mean we can use the same metrics if the ultimate outcome is improved. Rapamycin improved lifespan in mice with dramatic improvement in organ aging shown at autopsy compared to the control group. We should be open to Pseudo Events / Findings / Lab values when we change the variables but of course not ignore them as possible concern.
Thanks for pulling this. Your patients are lucky to have you:)
The discussion was awesome and opened me to some new information I was not aware of. The two articles @rivasp12 presented were new to me. One very supportive of low dose Rapa and the other showing how close I could get on even just 1mg / day to therapeutic troughs ( 1.2mg in study) for renal transplant patients and mTOR2 inhibition. All valuable information, but @rivasp12 statement below was even more valuable
I am good with the compliment of creativity, but realized I am not up to being ballsey So, a change in approach! I am going to try a 1mg every other day approach. I will check a peak and trough level in about 2 weeks and give subjective and objective feed back.
desertshores and David: I got peak and trough testing at Quest Diagnostics and both times blood was drawn at exactly the time of my appointment. I ordered through Ulta Lab Tests for a cost of $108 each time, including draw fee. One thing that may have made a difference in timing is that I ordered on the phone and was able to set up the appointment at a lab that wasn’t as busy as others. They could see the appointment schedules of all the labs they used. The labs in or near hospitals were the busiest.
Appears you believe 6mg/week is bioequivalent to 1mg/day…absolutely NOT. The pharmacology of biodistribution and pharmacokinetics are highly non linear. With the rapid peak and 62 hr half life, daily dosing will fundamentally alter the balance between absorption and clearance. 1mg/day is a VERY potent dose.
Dr Green: “The side effects of daily rapamycin are TOTALLY different from the side-effects of weekly rapamycin. Daily rapamycin is used to reduce both mTORCl and mTORC2. Reduction of mTORC2 has significant side-effects. Almost all the harmful side-effects of rapamycin use are from lowering mTORC2 and all the beneficial anti-aging effects are from lowering mTORC1.”
We already know this from the work of Lamming, etc. While studies show this, and clinical translation quasi confirms (have we ever seen measurement of mTOR1 and mTOR2 in humans?..NOT), this is NOT to say that the right daily dose cannot produce a better AUC/biomarkers/side effect profile, the purpose of your exploratory protocol. It’s all in the dose.
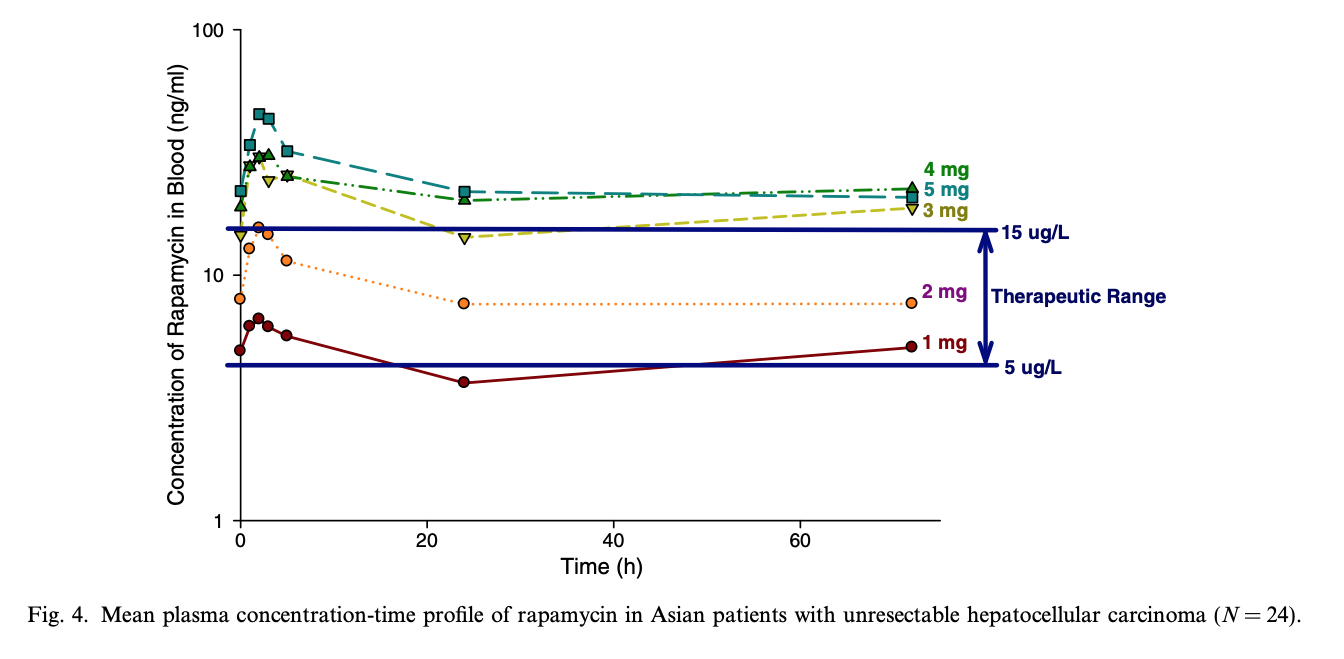
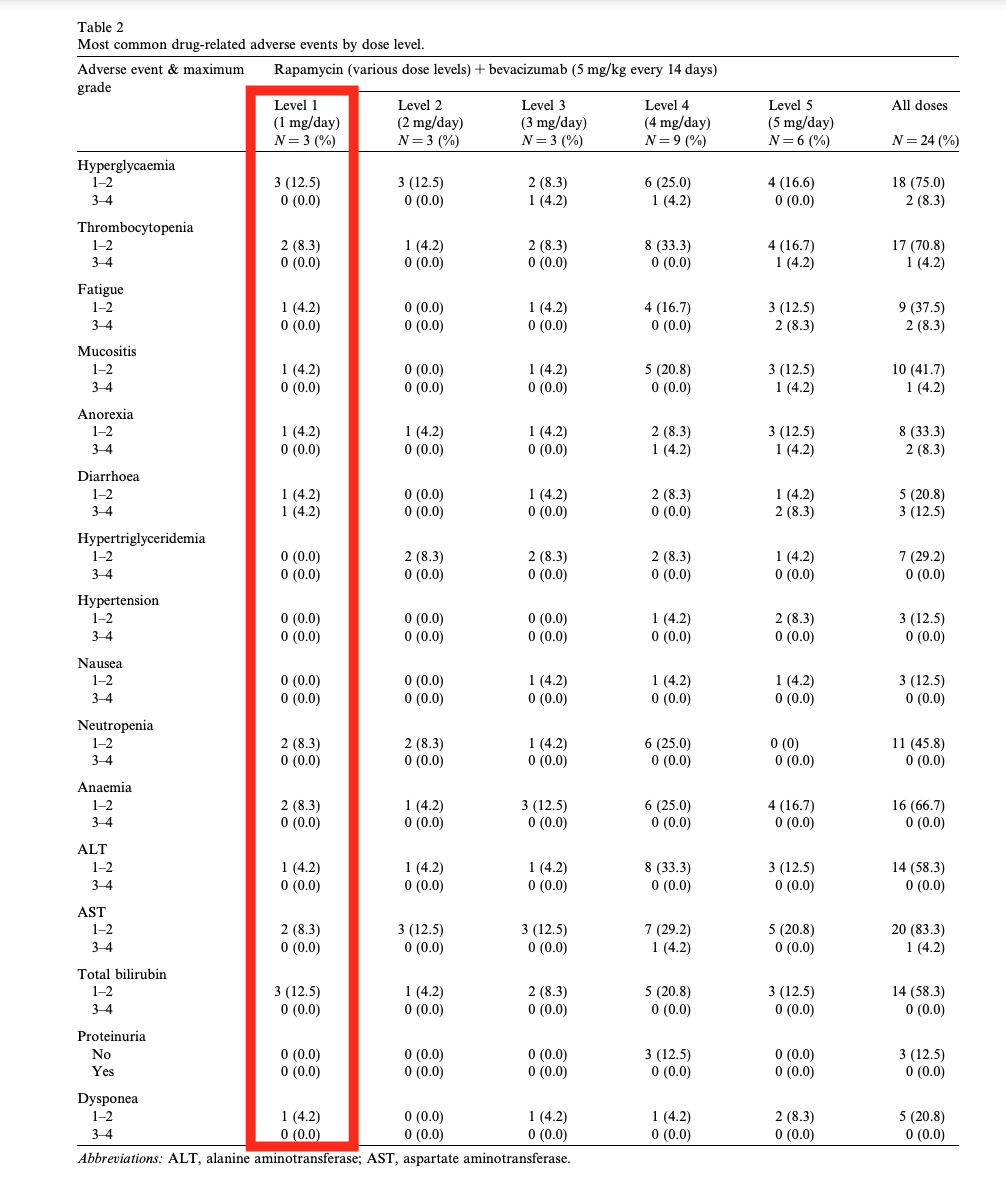
A Phase 1 dose-finding and pharmacodynamic study of rapamycin in combination with bevacizumab in patients with unresectable hepatocellular carcinoma https://sci-hub.se/10.1016/j.ejca.2012.11.008
“First, prior studies evaluating sirolimus pharmacokinetics have suggested a linear relationship between dose delivered and AUC (47, 48). In our study, a nearly 7-fold increase in AUC was seen after doubling the dose from 0.5mg/week to 1 mg/week.”
In the graph below you can see that doubling rapamycin from 1mg/day to 2mg/day produces a far higher than 2X increase in trough and AUC. And even 1mg/day can produce trough above 5 ug/L.
“The antiangiogenic and immunosuppressive effects of rapamycin are mediated by the drug’s effect on endothelial cells and lymphocytes, respectively. Cmin may not be a good indicator of the drug exposure in endothelial cells compared to AUC0–inf or dose. Hence, AUC0–inf or dose
may be more suitable biomarkers of the antiangiogenic effect of rapamycin”
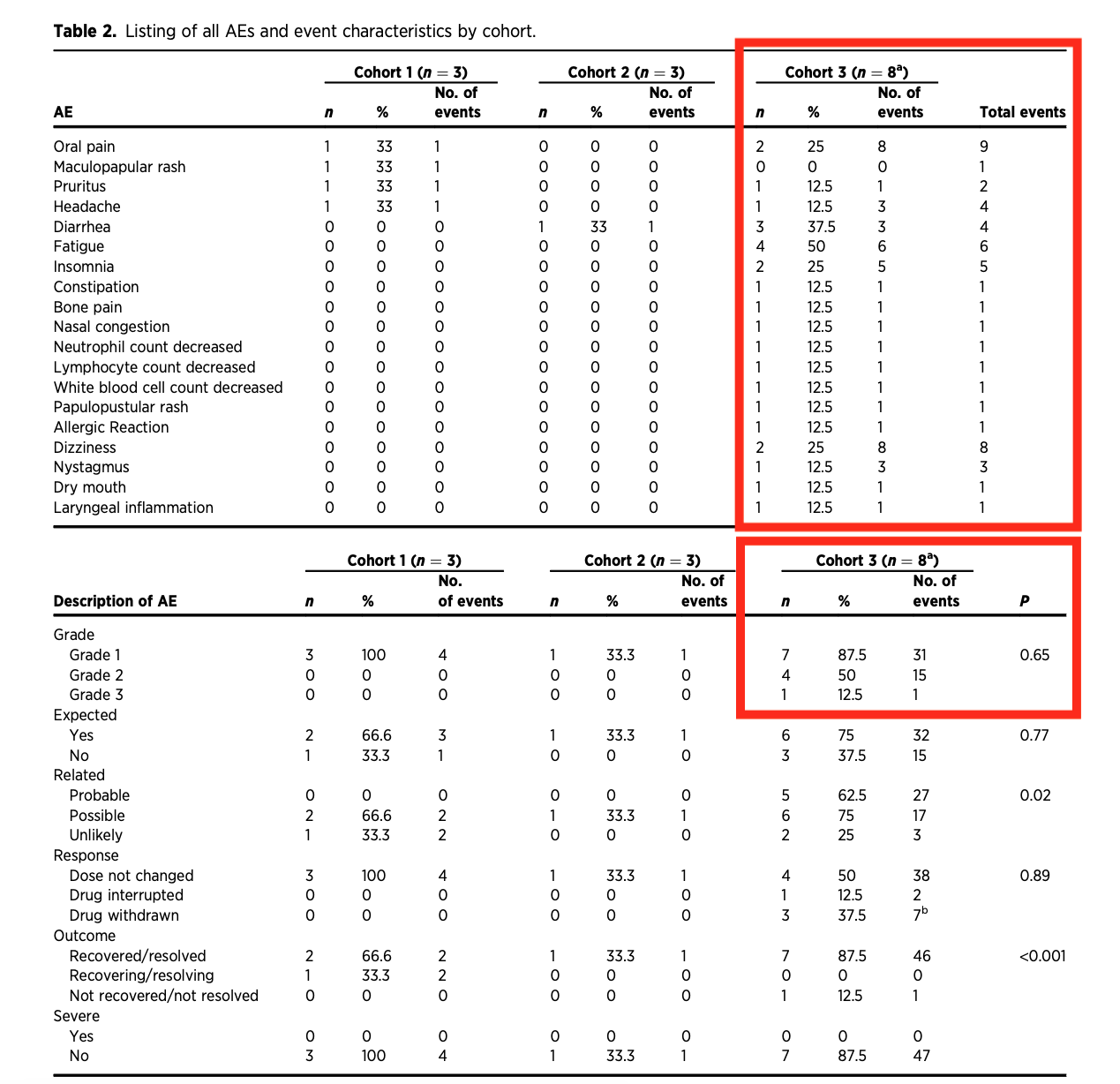
Phase I Trial of Encapsulated Rapamycin in Patients with Prostate Cancer Under Active Surveillance to Prevent Progression
Cohort 3 in the image below is 0.5mg/DAY rapamycin. The range and level of ADE and DLT is far higher than the mathematical equivalency of say 3.5mg/week (7 x 0.5mg/day). Most people and studies I’ve seen, 3.5mg/week has very little impact (population level). Yet, 0.5mg/DAY is quite potent already. They didn’t measure and/or report any lipid or glucose markers.
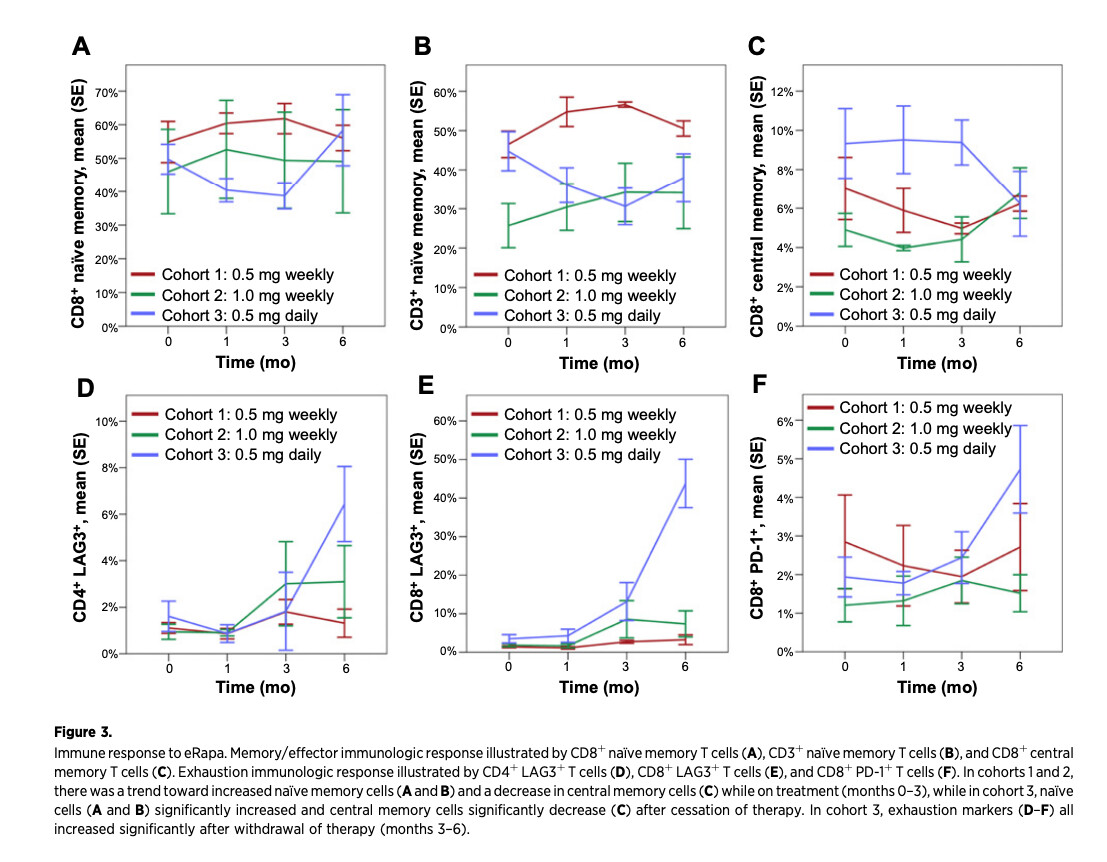
“The impact of rapamycin on tumor cell proliferation is also likely secondary to modulation of the immune system, a process that would require a longer treatment period than 2 weeks in both in vivo and clinical studies to reduce immune exhaustion and senescence while stimulating an effector response.”
Immunologic effects
“Immunologic data were available for all patients in cohorts 1 (0.5mg/WEEK) and 2 (1mg/WEEK) at each specified timepoint. In cohort 3 (0.5mg/DAY), samples were collected from all patients (n ¼ 8) at baseline, from 7 patients at the 1-month timepoint, and from 5 patients at the 3- and
6-month timepoints. Weekly dosing (cohorts 1 and 2) tended to increase na€ve cell populations and reduce central memory cells, while daily dosing (cohort 3) tended to maintain markers
of central memory”
“The 0.5 mg daily dose, which resulted in the highest cumulative total dose per week of each of the dosing regimens studied, produced a higher degree of mild toxicity and a transient negative impact on QoL”
IF you have a good steady state baseline of 6 mg/week re side effects, biomarkers, trough level Sirolimus, then I’d suggest perhaps starting with 0.5mg/day, and let it run for longer than 2-3 weeks before you take new markers. You are n=1, and your results may be quite different than studies referenced capturing 0.5mg/day or 1mg/day. Perhaps start with 1mg/day and see how it goes, but if you really start to feel like crap, then perhaps back off to 0.5mg/day, and let that run.
Other than biomarkers and side effects, you of course will never be able to assess long term impact (lifespan), but you might be able to titrate closer towards Dr B’s theory of “taking as much as you can without side effects”, which is as good as any human translation goal post. And “as much as you can” meaning, this might implicitly translate to AUC. If you an increase your AUC and not negatively impact long term biomarkers (lipids/glucose, WBC, etc)/ADE, a potentially positive outcome. A worthwhile n=1 experiment!
Patient feelings are absolutely important to track, but we must also consider - overeating feels better than calorie restriction for a sizable amount of people - partly why compliance to CR is so poor - most researchers are on the route to mimetics instead.
On the flip side, when I tried cutting down to ~6% body fat (very briefly) I felt horrible and it appears to be associated with a lot of negative effects if prolonged, and I don’t think I’d ever want to go down near 4-5% again - 11% is close to ideal for me.
As for your mTOR question in terms of different stimuli - I don’t think it’s a particularly big issue but I’m flying mostly blind based on analogy. For example, I don’t avoid all leucine/BCAAs (from food) after workouts - it’s actually tissue-specific in activating mTOR - namely liver, muscle, fat. Okinawans were basically CR but still ate meat like pork occasionally and “worked out” in various ways.
The main theory is hyperactivation of mTOR btw - not always inhibition of mTOR. Exercise isn’t just mTOR either.
Another issue I have is GH/IGF-1 “bad” is not that simple. For example, I’d generally (big generalization) want peripheral IGF-1 generally on the low side, but not necessarily central IGF-1 when it comes to the brain.
Thanks for that very extensive and compelling input.
I was not assuming that a 6mg / weekly dose was equal to a 1mg / daily dose - just looking for an entry point and most of the information I had at the point of was that it was a sub-theraputic dose for renal transplant patients ( usually starts about 2mg and up). @rivasp12 posted a study out of Iran that showed doses as low as 1.2mg/day could reach therapeutic trough levels to complement what you have extensively demonstrated. All good reasons to run the plan by the brain trust!!
My altered plan for now is very close to what you suggested of 0.5mg/ day and do a 1mg every other day. My thought was a little higher peak and hopefully less side effect issues - but then were all back to the game of guessing and how does using mTOR stimulators at the same time alter everything.
Yep, my thoughts exactly! If I feel like crap then time to go back to what has already helped.
Certainly they did eat some meat/seafood, but they were classically 9% protein. I doubt ANYONE on this forum is doing 9% protein. And Okinawans are arguably the longest lived human cohorts studied.
Sorry, but for the laymen here, please use “plain speak”.
I didn’t understand your reference," QOD dosing, so I had to look it up.
Every other day (q.o.d.) I think many of us here do not understand very many common medical abbreviations.
Borrowing from Reddit: “Explain Like I’m Five”
I am really interested in what you have to say and I will be avidly following your experiment.
“Notice the use of q for every and d for day. This abbreviation is now discouraged, because too often it was mistaken for “every day,” so while you may still see it occasionally, you should always write out “every other day” instead of using q.o.d.”
Absolutely - I’m not saying one should go extra high (complete) protein as many bodybuilders do with sipping whey shakes all day - but I’m not quite tied to low protein (<10%) over say lower methionine and higher glycine + perhaps serine (ie collagen peptides, seaweeds/microalgae and fermented soy). My current thinking is moderate to moderate-low if you include collagen peptides as “protein”. But there’s near zero methionine in it.
Arguably, protein is way too crude a measure. So I really don’t buy that line of thinking as a high protein must be “bad” or low protein must be “good”. For example, glycine made it to the ITP and turned out positive, as expected. With a lot of glycine added to standard mice chow - that would not be classified as “low protein”.
Yep I’m not tied to Okinawan only - my main interest with them was the combinations of “food as medicine” they used since they’re probably safe-ish - the problem is identifying the array of compounds in it and food-drug/drug-drug interactions - if I was 100% tied to it, I would have not even considered rapamycin, acarbose, and high glycine/low methionine.