The downside is quite minimal for most people - you might get a mouth sore, you might get slightly raised lipids, etc.
And while most of the benefits are, the research suggests, likely to accrue over time there are also many people who get immediate benefits. More energy, elimination of any aches or pains that frequently come with higher exercise regimens, etc.
mTOR inhibition is a really hard thing to calculate or measure… we can’t do it clinically yet. So we really don’t know if lean, high exercising, moderate food intake people are vastly different, or minimally different, from rapamycin users.
I think the biggest variable here is “risk propensity”. Some people are comfortable with more risk, others with less risk. From looking at my friends and others who decide to try or not try rapamycin, I think this is the largest factor that decides which side you fall on.
You’re better off taking care of the low-hanging fruits first: control your high LDL to help reduce CV risk, and reduce your HbA1c/insulin/glucose if they’re too high. I assume your BMI is within a healthy range, and your lean mass is adequate. Rapamycin is the cherry on top, and in fact won’t help you much if your LDL and glucose are out of control.
I agree with @relaxedmeatball especially in regard to traditional risks.
Having no family history of CAD is relatively meaningless in regard to risk, and assuming good genes in the family predict outcome is a problem - as it probably only is 15-20% of the outcome with the rest being lifestyle.
Now having a great lifestyle runs in families, and individuals assume it’s genetics when that is the minor part.
I’d be super comfortable with your assessment of being low risk and not treating your lipids if you grabbed a CCTA with Cleerly analysis and it was all clear and got an MRA head/neck and this was all clear including no white matter changes.
I have several patients with great family histories, great lifestyles and lipids that really aren’t bad that have extensive and unexpected disease on this assessment.
I also have a good number who have pretty high lipids and get this assessment and have no vascular disease I can find and have made it into their 70’s. I still recommend they take some low dose lipid medications, but I also tell them that objectively I cannot make a strong argument for that as their phenotype is markedly more important.
There are a lot of factors that go into forming vascular disease - I have my list that I optimize:
ApoB + Lp(a) + 9p21 + Apo E4 are the low hanging ones to consider on the lipid/unexpected risk side.
Omega 3 index
Homocysteine
Insulin sensitivity
Vitamin D level and Vitamin K2MK7
If these are not good, my pre-test probability of disease when I test is quite high.
Additionally, malignancy is a wild card - and surveillance of this including MRI yearly plus all recommended screenings are important.
Sarcopenia/Osteoporosis/Trauma
Infections/Immunizations
Optimize these a few more low hanging fruit … and only then should we be thinking about doing the clever things, like rapamycin is my current approach.
These are not necessarily mutually exclusive . Optimize but move all the levers together, walk and chew gum is my approach, but I may have slightly greater risk tolerance .
So yeah, you’re missing the wood for the trees here. Don’t even think about Rapamycin until you’ve dealt with this, or at least get an all-clear by CTCA scan if you don’t want to lower the LDL-C with medications. @DrFraser is talking 100% sense here.
Just to put this into context: you’re looking at an off-lab use of an unproven medication with unknown benefits, but ignoring something which is the cause of death in 1/4 of people.
Hi Jaak, I’m not well versed in this like the others but would not take it in your situation. I did for 8 months and all it did was raise my lipids and glucose. If your LDL is already 140 it will likely go higher. As for your dad being 97 but not really living and you want to really live to 100, did your dad live his life with your life long discipline/excellent health practices? If not then you already have quite an edge on your dad. I greatly admire your life long discipline for good health.
Thanks for sharing your experience — that’s really helpful.
I’m cautious about anything that might make my Lipids worse, and I feel I first need to get a better understanding of my situation. The ‘right’ amount of lipids or cholesterol seems incredibly complex.(e.g. If HDL is very high, 120 and Triglycerides are low, 40, is high LDL 140 still a problem?.. there seems to be evidence it may not be?)
To find out, I’m thinking about seeing a heart/cholesterol specialist and possibly getting a Coronary Artery Calcium (CAC) scan. I recently looked into my dad’s medical history and discovered he was diagnosed with hypercholesterolemia back in 1998. Genetically, I’m not sure if that’s good or bad news — but he seems to have gotten away with it.
He was a carpenter, worked hard until his late 60s, and stayed active in his garden until about 85. His life was simple and regular — potatoes, vegetables from the garden, some meat, a beer or two every day, no supplements, no formal exercise. He smoked as a teenager but stopped in his twenties and was never really sick.
His legs gave out three years ago, and now at 97 he’s in a nursing home — still healthy in many ways, but no longer mobile.
I’d be happy to reach his age, but I’d like to add one thing he lost in his 90s: mobility and independence.
I have hypercholesterolemia too from my mom, but my coronary calcium scan score is zero at almost 68 years.
Same on 2 tests in past 4 years.
My mom lived to 86 - no heart issues and then didn’t want treated when she had pneumonia.
She knew it would kill her, but she was done living. Took morphine to calm her while her lungs filled… congestive heart failure killed her, but it took a full week. Her heart refused to give up.
So, hypercholesterolemia can just be genetic. And, not a game changer. Your dad… my mom.
I think we all know by now that a CTA , especially with CLEERLY is the best test because it will show soft plaque, even if your CAC is 0. Having said that, because it’s an expensive and more invasive test, as a first step, I do encourage your idea of getting a CAC. It’s easy and cheap, and while it won’t prove you are in the clear, it is a simple way to show that you do have heart disease, and then you can act accordingly.
Even though I have a bad family history (not nothing!), I will share that no one expected me to have any problems, and the cardiologist said there was no reason to treat me (cough cough moron). I had a good diet and lifestyle, my total cholesterol at 210 was high, but it was not heart-attack-on-a-stick high, and my ‘good’ cholesterol was ‘enviable’.
All this is to say, at 40, I had a super high CAC, and the doctors were stunned. So much so that my doc here had me repeat it because he didn’t believe it.
It sounds like you do indeed have great genes and you are most likely fine, but I share this because you just never know and you should test.
Incase you don’t know, you can go get the CAC on your own before meeting with a specialist. Having the result will even make that appointment more productive.
Thanks, I hear you say, “Fix your high LDL”… but I don’t think it’s so simple.
To find out, I’ve made an appointment in Januari 2026 with a heart/cholesterol specialist in a university hospital. Let’s see what he does and says in my specific case.
In the meantime I asked my ChatGPT about taking statins and he/she said:
No single Lipid number or profile automatically means someone must take statins. Decisions depend on overall cardiovascular risk, not just cholesterol values.
Medicine doesn’t work with 100% rules: Even in high-risk cases, treatment choices are based on probabilities and risk reduction, not certainties. Statins lower risk, they do not function as a yes/no switch.
LDL is a causal factor, but context matters: LDL 140 mg/dL is not extremely high, but still above what most cardiology guidelines consider optimal for long-term prevention, especially beyond age 60.
However, very favorable markers like, HDL 120 (very high), Triglycerides 40 (excellent), are not automatically protective and very high HDL is more complex physiologically than once assumed.
The real decision is based on total risk, including:
Coronary Artery Calcium (CAC) score
Family history (especially premature heart disease)
Blood pressure
Inflammation markers (e.g., hs-CRP)
Lifestyle, fitness, diet
Smoking history
Metabolic markers (HbA1c, ApoB, Lp(a), insulin)
Symptoms or plaque evidence
With CAC = 0, many cardiologists would delay statins and monitor. With significant CAC, statins become more strongly recommended.
Summary: Your Lipid numbers are interesting and partly excellent, but no, statins are not automatically mandatory. A cardiologist would likely suggest additional risk evaluation, with CAC being the most informative next step.
No, of course they’re not mandatory. I didn’t say that they were.
If you look at guidelines from AHA and ESC, they advise getting LDL-C below 100mg/dl as a basic target. Optimal cardiovascular protection comes from getting it below 70mg/dl. Some people on this forum with higher risk profiles go even lower (for example, me: my LDL-C was >200mg/dl for 29 years until I realised I had a genetic condition, and now I never set it go higher than 30mg/dl).
If you look at studies like PESA (prevention of early atherosclerosis) they are finding risk reductions down to 40mg/dl. So on that basis, 140mg/dl is not extremely high, but it’s definitely not a “pro longevity” number.
ChatGPT is totally correct that the decision should be made based on multiple factors. Lp(a) is important, because it’s almost entirely genetic. If it’s high, you need to be much more aggressive with LDL-C (ApoB) lowering. Blood pressure is also a really important one. Doing a CAC would definitely be useful. If it’s anything except zero, then the decision to start a statin becomes easy IMO (here I disagree with ChatGPT that the CAC needs to be “significant”). A positive score, even if tiny, means that you’ve already built plaque many years ago and it’s gone through a whole cycle of inflammation and repair. It means that your current LDL-C level is enough to form plaque, and it also means that you probably have soft plaque which hasn’t calcified yet. If you do come back totally clean with a CAC of zero, then it becomes a more complex decision.
Some people are lucky, and might have high LDL-C and never accumulate plaque. Others might be unlucky and accumulate low of plaque at only moderate LDL-C levels. But for most people, most of the time, higher LDL-C will mean more plaque.
Anyway, it’s great that you’ve got an appointment for January. I hope you don’t misinterpret my advice as me pressuring/bullying you into taking statins. I’m just wanting to point out that in the context of living long and healthy, cardiovascular disease kills about 1/4 of people and the main driver is LDL-C. It’s not something you want to ignore or downplay.
I also don’t mean to hijack your thread about taking Rapamycin
I live where odds are everything. You are in denial if you think your LDL is okay.
If you have been reading the threads, you should know that the preponderance of the evidence says your LDL is too high. Your HDL is a signal that something is wrong.
Odds are you need to be on a statin. You can bet against the house, your choice.
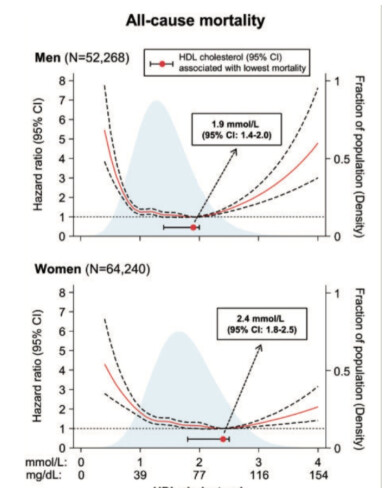
I’ve found multiple large-scale studies showing a ‘U-shaped’ risk curve. This means that both very low and very high HDL levels are linked to an increased risk of mortality, directly
contradicting the old ‘higher is better’ mantra. “The association between HDL cholesterol concentrations and all-cause mortality was U-shaped for both men and women, with both extreme high and low concentrations being associated with high all-cause mortality risk.”
"The causal leap that HDL-C was a cause of protection, not just a marker, created a testable therapeutic hypothesis: pharmacologically raising HDL-C levels should reduce cardiovascular events. This hypothesis was pursued for decades, culminating in one of the most expensive and high-profile series of failures in modern pharmaceutical history.
"High-density lipoprotein cholesterol (HDL-c) has long been referred to as ‘good cholesterol’ due to its apparent inverse relationship with future CVD risk. More recent research has questioned a causal role for HDL-c in this relationship, however, as both genetic studies and numerous large-scale randomised controlled trials have found no evidence of a cardiovascular
protective effect when HDL-c levels are raised."
“A critical revelation was that “HDL” is not a single entity. It is a highly heterogeneous (the quality of being diverse in composition) population of particles of different sizes, densities, and compositions.1 These particles can be classified broadly by density (e.g., lipid-rich HDL2 and protein-rich HDL3) 2 or charge (e.g., pre-β-HDL).”
This new paradigm leads to a practical “clinical triage” for interpreting an HDL-C result in 2025:If HDL-C is LOW (e.g., <40-50 mg/dL): Do not treat the HDL-C. Use this as a “risk enhancer”.67 The appropriate response is to be more aggressive in lowering the LDL-C target and to strongly advocate for lifestyle changes.8If HDL-C is NORMAL (e.g., 50-80 mg/dL): Acknowledge it and move on. This number is not the goal. The clinical focus remains 100% on achieving the patient’s LDL-C goal… 63 If HDL-C is “EXTREMELY” HIGH (e.g., >80-90 mg/dL): Do not celebrate. Treat this as an “abnormal level” and a red flag.13 This warrants an investigation into underlying causes, including alcohol use disorder, genetic dysfunction (like $SCARB1$), or other metabolic diseases.
I have ben taking 6mg weekly every other month. Don’t notice anything, but hope to increase health span/longevity. Problem just arose when I was going to purchase a short term/long term care policy (I am 63). The insurance company does not want to write the policy because they think I take it for an organ transplant…
How does the insurance company know you’re taking rapamycin? None of my healthcare providers know I’m taking rapamycin. Nor any other drug that I take that has not been prescribed by my doctor. I take empagliflozin, telmisartan, bempedoic acid + ezetimibe, pitavastatin in addition to rapamycin. None of this is in any database anywhere, certainly not reported by me to any health provider or insurer. None of my friends know. Only my wife, and this website, where I’m active as CronosTempi.
What is the advantage of a doctor knowing you take it? The vast majority have no idea about rapamycin, or any prescription drug in its off label use of longevity indication. So they’re likely to be utterly useless in assisting you in any way - with rare exceptions of doctors who specialize in the field. Of course, you may not feel you have enough medical knowledge to safely take a drug without a doctors supervision. But if that is the case, then odds are you should not be taking that drug at all. If you are taking any drug without it being prescribed by a doctor, it is on you to do all the research to be confident in your choices, and if you get to that level, you will discover that you now know more about this drug and its likely impact on your health than almost any ordinary doctor out there who doesn’t specialize in this field. These can be powerful drugs, and it’s a big responsibility to take upon yourself.
As to insurance companies, the less they know, the better. There is no way in which you benefit by an insurance company knowing your health status. Also, as a patient, you should have an appropriate relationship with your doctor, by which I mean, it is you who should have the ultimate decision making power when it comes to your health. The doctor is an advisor. In that capacity, you can sometimes ask for medical advice and preface it by asking whether you can ask this question off the record, and not have it recorded in your medical file. If they agree, you ask your question. Speaking for myself, I simply do not share everything with my doc. He’s there as a representative of the healthcare system, including insurance companies, and I go there for my yearly physicals to keep my insurance. That’s it. Example: I am soon having cervical fusion surgery, and insurance is paying for it. This is the first time I have used insurance resources in a big way, after a lifetime of paying premiums. This is the purpose of insurance: big, often unexpected, costly procedures and care. This is why I have it, and why I have always paid my premiums. But they need know nothing else. Now it is on me to handle the drugs I take around this surgery. I’ve done my research. We’ll see. My PCP is involved only insofar as absolutely necessary. Your info is your info, and you should share it as little as possible, I think. YMMV.
Thanks. My HDL used to be in the 80-90 range up to 5 years ago. I then started TRE 16:8 and 2 years ago I added weekly 24h fast. I also increased my exercise level from about 10h/week to 15h/week. Now my HDL is in the 120 range while my Triglycerides came down to 40 range. I read that both Fasting and Exercise seem to drive HDL higher and Triglycerides lower… I’ll discuss all of that with the Cardiologist in Januari.
The Economist also has a new piece on LDL/HDL and Cholesterol complexity: https://archive.ph/c0Saj