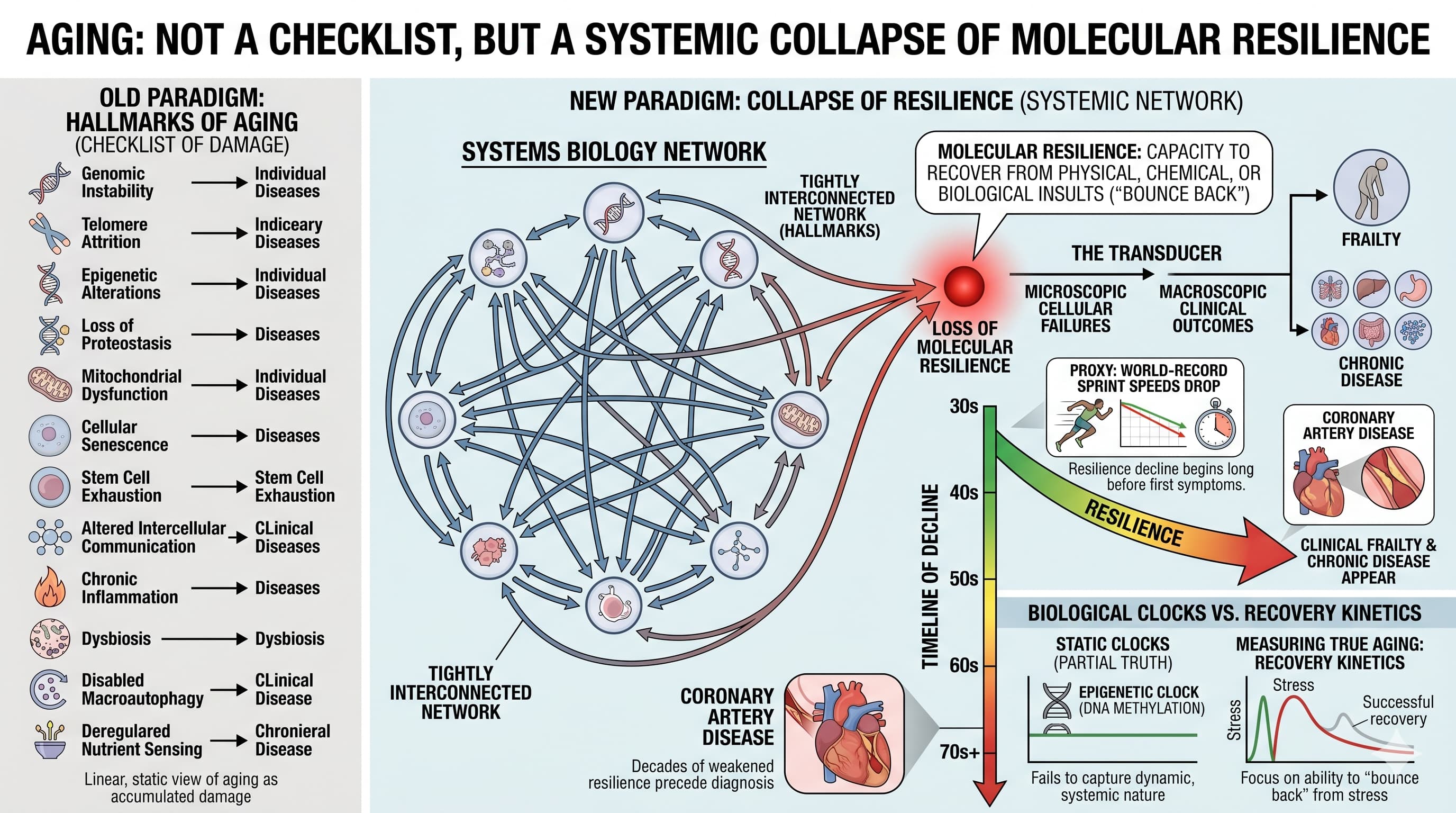
For over a decade, the “Hallmarks of Aging” have served as the holy grail for longevity research, providing a neat list of cellular villains like telomere attrition and mitochondrial dysfunction. However, a provocative new editorial in GeroScience argues that focusing on these individual hallmarks misses the forest for the trees. Authors Felipe Sierra and Viviana Perez suggest that aging is not a simple checklist of damage, but a systemic collapse of molecular resilience —the ability of an organism to “bounce back” from stress.
The authors posit that the hallmarks are essentially a tightly interconnected systems biology network. Because they are so interdependent, trying to identify a single “driver” of aging is a fool’s errand. Instead, every hallmark converges into a single, unified outcome: the loss of the capacity to recover from physical, chemical, or biological insults. This loss of resilience acts as a “transducer,” turning microscopic cellular failures into macroscopic clinical outcomes like frailty and chronic disease.
One of the most striking claims is the timeline. While clinical frailty typically surfaces in the 70s, the decline in resilience begins as early as the 30s or 40s. The authors use world-record sprint speeds as a proxy, showing a clear performance drop long before the first signs of age-related disease appear. By the time a person is diagnosed with coronary artery disease, they have already experienced decades of “weakened” resilience.
The current “gold standard” for measuring age—biological clocks—comes under fire here. The authors argue that an epigenetic clock based only on DNA methylation is a partial truth at best, failing to capture the dynamic, “systems biology” nature of the whole organism. To truly understand aging, we must stop looking at baseline states and start looking at recovery kinetics. The future of longevity science lies not in cataloging damage, but in measuring how fast and how well a system returns to equilibrium after a challenge.
Actionable Insights
The primary takeaway for those seeking to maximize lifespan is a shift in focus from static biomarkers to dynamic stress-testing. Because molecular resilience declines decades before disease manifests, current diagnostic models are “too late” for optimal intervention.
-
Monitor Recovery, Not Just Performance: Baseline metrics (like resting heart rate or fasting glucose) are insufficient. Actionable health tracking should prioritize the kinetics of recovery —how quickly your system returns to baseline after a workout, a high-fat meal, or an illness.
-
Focus on Stress-Response Pathways: Rather than just “removing damage,” prioritize interventions that bolster cellular defense mechanisms (e.g., proteostasis and DNA repair).
-
Utilize Continuous Monitoring: Wearables that provide longitudinal data on blood pressure and glucose fluctuations during “daily living stresses” offer a better proxy for resilience than annual blood draws.
-
Target the “Gap” Years: The window for the most effective intervention is between ages 40 and 60, before the rate of resilience loss accelerates into frailty. Establishing a “maximal” resilience baseline at age 40 is recommended for personalized longevity planning.
Context & Impact Evaluation
-
Open Access Paper: Loss of molecular resilience as the ultimate outcome of aging biology
-
Institution: Geroscience Consulting LLC and the National Institute on Aging (NIA), NIH.
-
Country: USA.
-
Journal Name: GeroScience (Official Journal of the American Aging Association).
-
Impact Evaluation: The impact score (CiteScore/JIF) of this journal is approximately 7.5, evaluated against a typical high-end range of 0–60+ for top general science journals; therefore, this is a High impact journal within the specialized field of gerontology and aging biology.
Related Reading:
1 Like
If anyone has some good questions on this paper, please post them. I ran into the main author of this paper (Felipe Sierra) at the Berkeley Longevity Conference and he was very open to sharing on his areas of focus. He is very interested in the area of “intrinsic capacity” tracking as an area of focus for improving longevity.
Ideas for Practical Implementation:
This protocol transitions longevity medicine from a static diagnostic model—which measures damage already accumulated—to a kinetic stress-response model that assesses the system’s capacity to prevent future collapse. Based on the framework that aging is the progressive loss of coordination between molecular hallmarks, this approach defines health not by your baseline state, but by your Resilience Signature: the speed and efficiency with which your biology returns to homeostatic equilibrium after a standardized perturbation.
1. The Kinetic Resilience Protocol: Systemic Stress Challenges
Traditional biological clocks provide a “snapshot” of aging, but they often fail to capture the dynamic “transducer” effect of resilience. To identify the rate of decay decades before frailty or disease manifests, you must utilize “provocative” testing.
Metabolic Resilience (The Nutrient Challenge)
Standard markers like HbA1c or fasting glucose are trailing indicators. A resilient metabolic system must handle acute caloric and glycemic loads without prolonged disruption.
-
The Stressor: 75g Oral Glucose Tolerance Test (OGTT) or a standardized 1,000-calorie “High-Fat/High-Carb” challenge meal.
-
The Kinetic Marker: Clearance Velocity. Monitor glucose and insulin levels at 30, 60, 120, and 180 minutes.
-
Actionable Metric: A resilient system shows a rapid insulin spike followed by a return to baseline glucose within 120 minutes. A “long tail” or delayed clearance indicates a loss of molecular coordination in insulin signaling and mitochondrial substrate switching.
Cardiorespiratory and Autonomic Resilience (The Physical Challenge)
Cardiovascular aging is best characterized by the transition between high-stress states and recovery.
-
The Stressor: Maximal exertion via a VO2 max ramp test or a 4-minute High-Intensity Interval (HIIT) bout.
-
The Kinetic Marker: Heart Rate Recovery (HRR) and HRV Rebound.
-
HRR-60: The drop in heart rate exactly 60 seconds after stopping exertion.
-
HRV Rebound: The time required for Heart Rate Variability (HRV) to return to your 7-day nocturnal baseline.
-
Actionable Metric: An HRR of less than 12 beats per minute (bpm) in the first minute post-exercise is a high-confidence signal of diminished autonomic resilience. Resilient individuals should see a significant HRV rebound within 24 hours of the stressor.
Immunological Resilience (The Inflammatory Challenge)
Immunosenescence often remains “silent” until an infection occurs. This challenge measures the kinetics of the inflammatory “spike” and its subsequent resolution.
-
The Stressor: Acute physiological stress (e.g., eccentric muscle damage from high-intensity resistance training) or a standardized vaccination.
-
The Kinetic Marker: hs-CRP and Cytokine Resolution.
-
Actionable Metric: Measure high-sensitivity C-reactive protein (hs-CRP) at 12 hours and 48 hours post-stressor. A resilient immune system mounts a sharp initial response (pro-inflammatory) followed by rapid resolution. Chronic elevation beyond 48 hours suggests a “leakage” in the molecular pathways responsible for resolving inflammation.
2. Actionable Testing Battery for Longevity Enthusiasts
This list prioritizes readily accessible tools that transform “daily living stresses” into actionable data points.
| System |
Tool/Test |
Primary “Kinetic” Metric |
| Metabolic |
Continuous Glucose Monitor (CGM) |
Glycemic Variability: Focus on the “Mean Amplitude of Glycemic Excursions” (MAGE) rather than average glucose. |
| Metabolic |
Kraft Assay (5-point Insulin) |
Insulin AUC: The total area under the curve for insulin response over 3 hours. |
| Vascular |
Flow-Mediated Dilation (FMD) |
Endothelial Response: Percentage of arterial diameter increase after temporary occlusion (measures nitric oxide resilience). |
| Autonomic |
Wearable (Oura/Whoop/Garmin) |
Recovery Slope: The rate at which nocturnal HRV returns to baseline after alcohol, poor sleep, or travel. |
| Physical |
100m Sprint / Power Profile |
Performance Proxy: Current max power output compared to age-matched world records (a proxy for integrated systems resilience). |
3. Implementation Strategy: Establishing the Resilience Baseline
To make this data useful, it must be viewed as a longitudinal rate of change.
-
The “Maximal” Baseline (Ages 30–45): Establish your peak compensatory capacity. Perform the full battery of stress tests (OGTT, VO2 Max, HRR) while healthy to define your “gold standard” recovery curve.
-
The Longitudinal Audit (Every 2 Years): Aging is not linear. Re-testing every 24 months allows you to identify if your “Clearance Velocity” or “Recovery Slope” is declining faster than the expected age-related trajectory.
-
Opportunistic Tracking: Treat every illness or minor surgery as a “natural experiment.” Capture high-resolution data (HRV, temperature, glucose) during the recovery phase to map your unique “Resilience Signature.”
Summary of the Shift
The transition from static to dynamic testing acknowledges that aging is a “systems biology” problem. While measuring a single hallmark (like DNA methylation) is informative, measuring the outcome of all hallmarks—resilience—is the only way to assess the organism’s true biological age. Practical longevity requires prioritizing the kinetics of recovery; if your system can no longer “bounce back” from a high-fat meal or a hard sprint, the molecular hallmarks have already begun their systemic collapse.