While female reproductive aging has historically dominated clinical and public health discussions due to the clear bio-marker boundary of menopause, male reproductive aging is rapidly emerging as a critical modern health crisis. Driven by global socioeconomic shifts toward delayed parenthood, advanced paternal age is now directly tied to progressive semen degradation, elevated sperm DNA fragmentation, increased miscarriage rates, and a stark rise in neurodevelopmental and psychiatric disorders in offspring . A comprehensive review of the testicular architecture reveals that male reproductive decline is not dictated by isolated cellular defects, but by a self-amplifying, highly interconnected degenerative network . Within this multi-tiered system, chronological aging triggers an upstream cascade that actively destroys both the endocrine and structural foundations of male fertility.
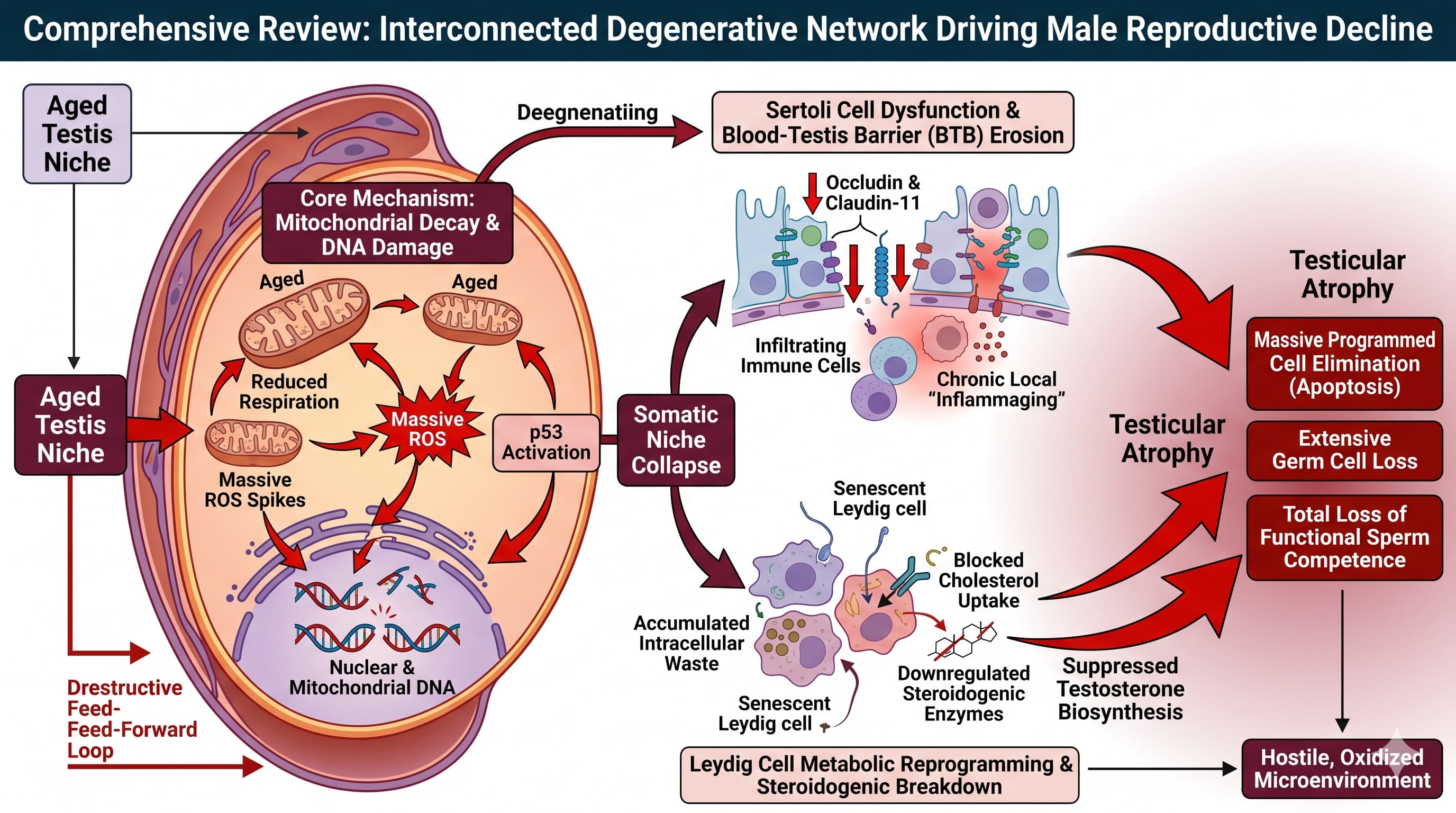
The core of this reproductive decline operates via a destructive feed-forward loop centered on mitochondrial decay. As the energy factories of the testis age, a progressive drop in respiration efficiency triggers massive internal spikes in reactive oxygen species (ROS) . This localized oxidative stress continuously attacks cellular structures, causing extensive nuclear and mitochondrial DNA double-strand breaks . When internal DNA repair pathways are overwhelmed, cells activate checkpoint cascades led by the tumor suppressor p53, forcing the vital somatic niche populations of the testis—specifically supporting Sertoli cells and testosterone-producing Leydig cells—into permanent, irreversible growth arrest, or cellular senescence.
The consequences of this somatic niche collapse are profoundly destructive. In the blood-testis barrier (BTB)—the protective immunological gatekeeper maintained by Sertoli cells—aging drives a severe downregulation of baseline adhesion proteins like Occludin and Claudin-11 . Tearing open this barrier allows systemic inflammatory immune cells to infiltrate the seminiferous epithelium, exposing autoantigenic germ cells and establishing a state of chronic local “inflammaging”. Concurrently, senescent Leydig cells undergo dramatic metabolic reprogramming. Crippled autophagic flux causes an accumulation of damaged intracellular waste, which blocks raw cholesterol uptake and downregulates master steroidogenic enzymes. This starvation mechanism severely suppresses circulating testosterone biosynthesis. Ultimately, this hostile, oxidized microenvironment shifts the tissue profile from homeostatic cell maintenance to mass programmed cell elimination, culminating in extensive germ cell apoptosis, testicular atrophy, and the total loss of functional sperm competence.
Actionable Insights
To translate these complex pathophysiological findings into highly practical longevity and biohacking protocols, clinicians and health-conscious individuals must explicitly target the distinct somatic nodes driving testicular decay:
-
Shield the Blood-Testis Barrier from Inflammaging: Incorporate specific natural compounds like curcumin or melatonin, which activate the AMPK/SIRT3 and Nrf2/HO-1 axes to enhance endogenous antioxidant defense systems, quench local mitochondrial ROS, and preserve essential Sertoli cell tight junction architecture.
-
Acknowledge the Ibuprofen Testosterone Penalty: Avoid the chronic, unmitigated use of standard analgesics like ibuprofen; consuming 1200 mg/day for six weeks represses Leydig cell steroidogenic enzymes, driving a state of compensatory hypogonadism and directly lowering the testosterone-to-luteinizing hormone ratio .
-
Upregulate DNA Repair capacity Systemically: Leverage NAD+ precursors like nicotinamide mononucleotide (NMN) or small-molecule OGG1 glycosylase enhancers (such as TH10785) to simultaneously enhance base-excision repair networks, protect spermatogonial stem cells, and limit downstream sperm DNA fragmentation .
-
Deploy Low-Dose Autophagy Flux Modulators: Utilize targeted autophagy enhancers like low-dose rapamycin to facilitate the clearance of damaged organelles and toxic p62 protein aggregates ; note that excessive high-dose mTORC1 inhibition completely backfires by pausing native spermatogenesis.
-
Optimize Endocrine Transport via rHGH Pathways: Monitor first-generation reproductive hormone modulators; recombinant human growth hormone (rHGH) acts through JAK2/STAT5 networks to upregulate cholesterol transport and optimize testosterone synthesis within failing Leydig progenitor lines.
Source:
-
Paywalled Paper: Testicular aging revisited: Current understanding of mechanisms and
emerging interventions - Institution: Key Laboratory of Applied Technology on Green-Eco-Healthy Animal Husbandry of Zhejiang Province, College of Animal Science and Technology & College of Veterinary Medicine of Zhejiang A&F University, Hangzhou, China.
- Country: China.
- Journal Name: Ageing Research Reviews.
- Impact Evaluation: The impact score of this journal is 13.1, evaluated against a typical high-end range of 0–60+ for top general science, therefore this is a High impact journal.