Thanks a lot for sharing the details!
2 Likes
Vitamin K2 and Heart Health Video

Open Access Research Study:
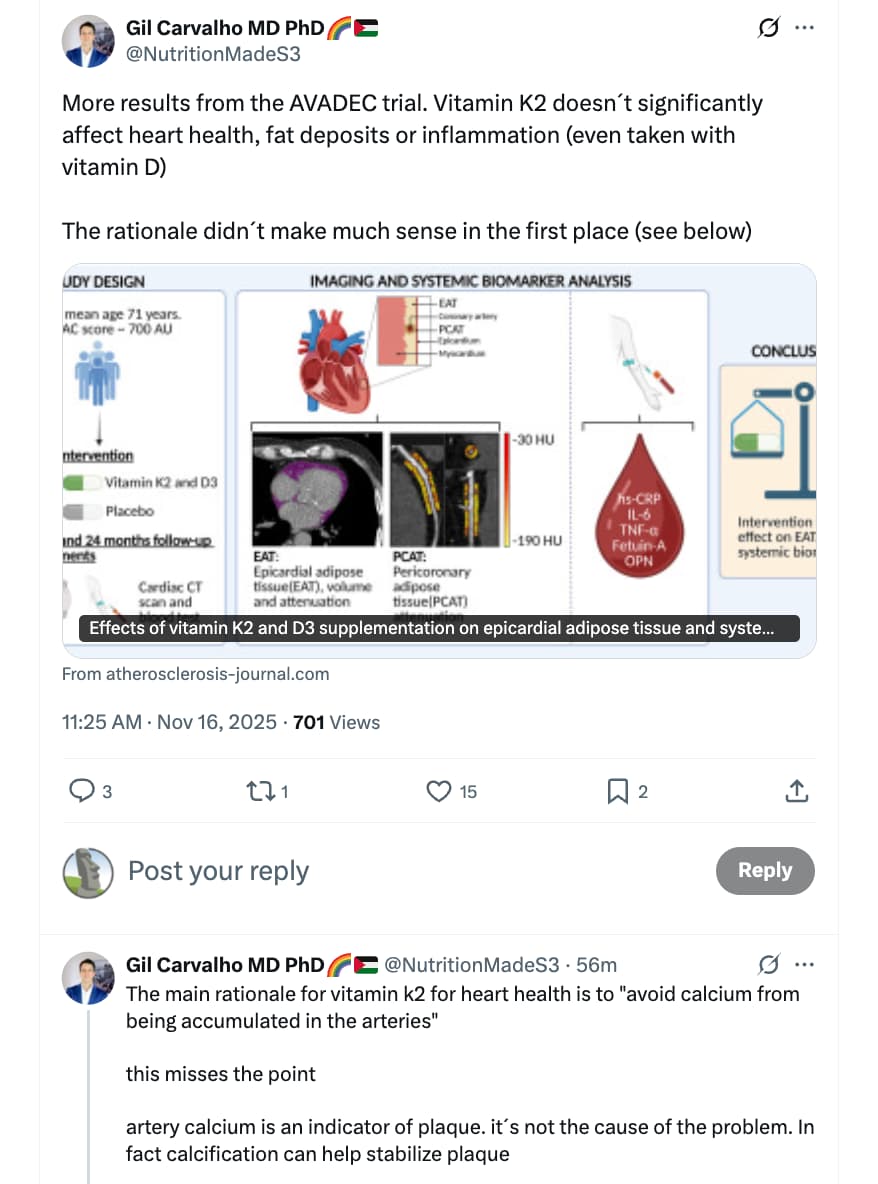
Effects of vitamin K2 and D3 supplementation on epicardial adipose tissue and systemic inflammation: A substudy of the AVADEC trial
Highlights
• High-dose vitamin K2+D3 improved dp-ucMGP and P-25-OH D but did not affect epicardial fat or inflammation.
• Findings align with prior studies: even high-dose, long-term vitamins may not affect cardiovascular inflammation.
• Cardiovascular inflammation involves complex mechanisms, and effective therapeutic modulation remains a challenge.
• Advanced disease and methodological limits may require alternative strategies for effective reduction in inflammation.
https://www.atherosclerosis-journal.com/article/S0021-9150(25)01438-8/fulltext
AI Summary of Video:
Introduction to Vitamin K2 and Heart Health
- The discussion centers on the role of vitamin K2 in cardiovascular health, specifically its potential to remove calcium from arteries.
- The speaker invites questions about vitamin K’s effects on bone health and glucose metabolism, indicating an openness to future content creation based on audience interest.
- The speaker clarifies their lack of conflicts of interest, stating they do not sell vitamins or supplements.
Forms of Vitamin K
- Vitamin K exists in two primary forms: K1, predominantly found in green leafy vegetables, and K2, which is sourced from animal products and fermented foods like natto and hard cheeses.
- The conversation explores the hypothesis that vitamin K2 could influence calcification in arteries through its role in activating proteins that inhibit this process.
Mechanism of Action of Vitamin K2
- Matrix GLA protein (MGP) is crucial in preventing calcification in artery walls, but its activation depends on adequate vitamin K levels.
- Research suggests that individuals with higher dietary vitamin K intake tend to have lower arterial calcium levels and reduced heart disease risk.
- However, correlation does not imply causation, and the efficacy of isolated vitamin K supplements remains uncertain.
Scientific Evidence on Vitamin K Supplementation
- Randomized trials have been conducted to assess the impact of vitamin K supplementation on arterial calcification and heart disease events.
- Some studies indicate that vitamin K supplementation may slow calcium deposition in arteries, yet the overall benefits for heart health remain debatable.
- The speaker emphasizes the importance of evaluating whether changes in calcium levels correlate with improved health outcomes, rather than merely focusing on calcium scores.
Understanding Calcium Scores
- Calcium in artery walls serves as an indicator of plaque progression rather than a direct cause of cardiovascular risk.
- The presence of calcification often signifies long-standing plaque buildup, and its increase can occur even while the risk of heart attacks decreases.
- Statins, commonly prescribed to lower heart disease risk, may lead to higher calcium scores as they stabilize plaque, which can confuse patients regarding their treatment efficacy.
Risks of Misinterpreting Calcium Scores
- The speaker warns against overinterpreting calcium scores, drawing parallels to HDL-cholesterol and its misunderstood relationship with heart disease risk.
- Relying solely on calcium scores or HDL levels can divert attention from addressing the actual causes of heart disease.
- The ultimate goal should be to assess interventions based on their impact on real health events, such as heart attacks and strokes.
Recent Trials on Vitamin K and Health Events
- Recent trials investigating vitamin K supplementation have shown mixed results regarding its effectiveness in reducing heart disease events.
- One notable study from 2009 lacked sufficient event data to draw conclusive results, while another trial with over 300 participants found no significant differences in calcium accrual rates between supplement and placebo groups.
- Some participants with high baseline calcium levels did show slower increases in calcium, but overall, the evidence remains inconclusive regarding the benefits of vitamin K supplements.
Safety and Side Effects of Vitamin K Supplements
- Most studies have not reported significant side effects from vitamin K supplements, even at higher dosages.
- Concerns about increased side effects in specific populations, such as the elderly, have been noted but are not widespread in the literature.
- The speaker cautions against the false sense of security that may arise from taking supplements without addressing underlying health issues.
Conclusion and Final Thoughts
- The speaker concludes that there is currently insufficient evidence to recommend vitamin K supplements for heart health based on event reduction.
- Future properly powered trials are necessary to establish any potential benefits of vitamin K supplementation in reducing heart disease events.
- The speaker encourages critical thinking regarding health claims and the importance of seeking evidence when considering supplements for heart health.
2 Likes
Digging into this a little more:
Prompt:
What is the scientific and clinical evidence that vitamin K2+D3 provide heart health benefits?
CGPT5.1 Response:
Short version:
- Vitamin D3 alone: Large randomized trials and meta-analyses show no meaningful reduction in heart attacks, strokes, or CV mortality from D3 supplements in generally healthy or mixed-risk adults.
- Vitamin K2 alone: There’s decent mechanistic plausibility and some human data that K2 improves surrogate markers (arterial stiffness, vitamin-K–dependent proteins, and possibly coronary calcium progression), but clinical outcome data (MI, stroke, death) are weak and inconsistent.
- K2 + D3 together: Mechanistically they make sense as a pair, but right now there is no solid clinical trial evidence that the combination reduces cardiovascular events. Claims that “K2+D3 protects your heart” are ahead of the data.
Below is the more granular breakdown.
2 Likes
So K2 may not be as important as we thought. Are there any downsides to taking K2?
from CGPT5.1:
Vitamin K2 (MK-7 or MK-4) is one of the lower-risk supplements out there, but it is not risk-free. The negatives mainly appear in specific medical contexts, high doses, or when combined with certain drugs.
So - just check for drug interactions.
2 Likes
I’m still hoping that Vit K1 and/or K2 might be helpful for calcification of the aortic valve (aortic stenosis), which is different in etiology and pathophysiology compared to calcification of atherosclerotic plaques. Unlike atheroma calcification, the pathologic calcification of heart valves is not a protective feature but rather causal in the eventual malfunction of the valves.
3 Likes
Why? Vitamin K2 should be looked at not just in the context of CVD, but other ones like bone health (research in Japan), prostate health, dental/gum health, skin etc. The research is of variable quality, but there’s enough smoke that betting on fire somewhere is a reasonable bet, seems to me. It’s a pity the CVD indication didn’t pan out, but not all is lost. Of course it all depends on why you are supplementing with K2, if it’s primarily or exclusively because of CVD, then this might be cause for reconsideration. I personally see enough other possible benefits to continue with this relatively low risk supplement. YMMV.
7 Likes
Good points. I’ll probably still keep taking it due to it’s other benefits.
People should be sensitive to the issue that there are different types of K2 with different effects.
2 Likes
Good point. That is true - there are some positive signs there.
CGPT Summary of Vitamin K2 research in other areas
Short version:
- Bone: Real human data is strongest here, especially from Japan (high-dose MK-4).
- Prostate, gum/dental, skin: Evidence is mostly observational / mechanistic / very early; nothing close to drug-level proof.
I’ll break it down by domain.
1. Mechanistic background (why K2 might matter)
Vitamin K2 (menaquinones, mainly MK-4 and MK-7) is a cofactor for the γ-carboxylation of vitamin-K–dependent proteins:
- Osteocalcin (OC) in bone → needed to bind calcium to hydroxyapatite.
- Matrix Gla protein (MGP) in vessels and soft tissue → inhibits pathological calcification.
Dietary K2 and supplements lower undercarboxylated osteocalcin (ucOC) and dp-ucMGP, markers of poor K status in bone and vasculature.
Mechanistically, this is highly plausible for bone and vascular effects; everything else (prostate, gums, skin) is extrapolation from these pathways + some cell/animal data.
2. Bone health – especially the Japanese data
2.1 High-dose MK-4 (menatetrenone) in Japan
Japan is where the strongest clinical signal exists. MK-4 at 45 mg/day is approved there as an osteoporosis drug, and multiple RCTs in older, high-risk populations have been run.
Key data:
-
Shiraki 2000 RCT – 241 osteoporotic patients, 24-month open-label RCT
- 45 mg/day MK-4 vs no K2.
- Lumbar BMD: control −3.3% vs MK-4 −0.5% over 24 months.
- Clinical fractures significantly lower with K2 (χ² = 10.9, p = 0.027).
-
JAMA Internal Medicine 2006 meta-analysis (Cockayne et al.) – 13 RCTs, 7 with fracture data, mostly Japanese postmenopausal women on MK-4 45 mg/day:
- Vertebral fractures: OR ≈ 0.40 (60% reduction).
- Hip fractures: OR ≈ 0.23 (∼77% reduction).
- All non-vertebral fractures: OR ≈ 0.19.
- BMD: modest but statistically significant benefit (SMD ~0.27).
- Authors explicitly caution the effect size looks “too good to be true”, trials not fracture-powered, and all fracture trials were done in Japan with generally low vit D/Ca intake and variable quality.
Later analyses and reviews continue to support some anti-fracture effect of high-dose MK-4 in high-risk Japanese populations, but emphasize trial quality issues and population specificity.
Take-home: In Japanese osteoporotic patients on 45 mg/day MK-4, fracture risk reduction is probably real, though the effect size in meta-analyses is likely inflated. Outside that setting, we do not have comparable fracture-endpoint data.
2.2 MK-7 and lower-dose K2 in Western populations
MK-7 (longer half-life, typically 90–200 µg/day in supplements) has been studied mostly in postmenopausal women:
-
3-year Dutch MK-7 RCT (180 µg/day) in healthy postmenopausal women showed:
- Reduced age-related decline in BMD at the lumbar spine and femoral neck and improved bone strength indices vs placebo.
-
Rønn 2021 3-year RCT in osteopenic postmenopausal women – 375 µg/day MK-7 + all participants on vitamin D3 and calcium:
- No significant difference in BMD, bone turnover markers, or microarchitecture between MK-7 and placebo.
- A 2024 meta-analysis of vitamin K supplementation (K1 and K2) reported:
- K2 supplementation modestly improved BMD in women, with stronger effects in those with low baseline K / high fracture risk, but heterogeneity was high and evidence quality overall low–moderate.
Interpretation:
- MK-7 at “supplement” doses (90–375 µg/day) clearly improves vitamin K status (lower ucOC).
- Evidence that this translates into fewer fractures in typical Western populations is weak/inconclusive so far.
- For someone already optimized on calcium, vitamin D, and standard osteoporosis therapies, K2 is best described as adjunctive with uncertain incremental benefit on hard outcomes.
3. Prostate health and prostate cancer
3.1 Epidemiology
-
Heidelberg EPIC cohort (Nimptsch 2008) – 11,319 men, 199 incident prostate cancers:
- Higher menaquinone (K2) intake associated with lower risk of advanced prostate cancer, but not total prostate cancer; phylloquinone (K1) showed no association.
- Later population studies (including US cohorts) have not consistently replicated a protective effect; some report no association between total vitamin K intake (K1 + K2) and total or advanced prostate cancer.
So: a signal in one European cohort for advanced disease, but not robust across populations.
3.2 Mechanistic / preclinical data
- K2 has been shown to induce apoptosis and inhibit proliferation in both androgen-dependent and androgen-independent prostate cancer cell lines (e.g., LNCaP, PC-3), via mitochondrial pathways and caspase activation.
- K-dependent proteins and MGP are expressed in prostate tissue, so the calcification/anti-calcification axis is at least biologically present.
Clinical reality:
- No convincing RCTs showing that K2 prevents prostate cancer, slows progression, or improves outcomes.
- Current human data = one positive observational signal + several null studies + supportive cell data → hypothesis-generating, not actionable.
4. Dental / gum (periodontal) health
Here the literature is early and messy:
4.1 Observational human data
-
2023 case–control study (Olszewska-Czyz et al.)
- Serum K2 levels were inversely associated with presence and severity of periodontitis (more K2 → less severe disease), even after adjusting for common confounders.
-
2025 epidemiologic study in elderly Americans
- Higher total vitamin K intake (not specifically K2, though K2 was included) was associated with lower prevalence of periodontitis.
These support “better K status correlates with better periodontal status”, but they’re cross-sectional or case–control – not causal proof.
4.2 Interventional / mechanistic data
- A nutrition–periodontitis review notes that vitamin K deficiency can contribute to gingival bleeding, but a specific trial of K supplementation did not reduce inflammatory markers in periodontium in established disease.
- There are older references (often cited in K2 marketing) to “reduced dental caries” with K2, but the underlying primary data are sparse and often not modern, well-controlled trials. A 2015 hypothesis paper explicitly says: “much research is needed to determine why this vitamin can reduce dental caries.”
Net:
- Biologically plausible: K-dependent proteins in dentin/bone; same osteocalcin/MGP story applied to alveolar bone and dentin.
- Evidence level: a couple of supportive observational studies + sketchy or negative intervention data. No robust RCTs showing that K2 meaningfully improves periodontal outcomes, caries, or tooth retention.
5. Skin / cosmetic aging
This is where the evidence is thinnest and heavily mixed with marketing.
5.1 Observational / niche clinical data
- In certain conditions with pathologic elastic fiber calcification, like pseudoxanthoma elasticum (PXE), vitamin K–dependent pathways are clearly involved, and K status may influence degree of skin elastin calcification and wrinkling.
- A population-based study cited in recent reviews found higher dietary vitamin K intake associated with fewer wrinkles and better skin elasticity in specific cohorts, but this was total K and observational.
5.2 Mechanistic ideas
- MGP is expressed in dermal elastic fibers; under-carboxylated MGP is linked to calcification and stiffening of elastin. K2 theoretically improves carboxylation → less calcification → better elasticity.
- K2 also has general anti-inflammatory and antioxidant effects in some models, which marketers extrapolate to “anti-aging skin.”
5.3 Actual intervention data
- As of now, no solid RCTs showing that oral K2 supplementation improves wrinkles, elasticity, or other clinically meaningful skin endpoints in healthy humans. Most “evidence” in skin-care articles is extrapolation from PXE, vascular calcification work, or generic K physiology.
So for skin: it’s biologically plausible and interesting, but clinically unproven.
6. How I’d summarize the overall evidence
Strongest / most credible
- Bone health in high-risk Japanese populations on high-dose MK-4 (45 mg/day):
- Multiple RCTs and a meta-analysis show meaningful fracture reduction and better BMD trajectories.
- These are essentially drug-like doses in a specific setting, not general supplement use.
- Surrogate markers:
- K2 (MK-4 and MK-7) consistently improves carboxylation of osteocalcin and MGP, which are mechanistically important for bone and vascular health.
Moderate / suggestive, but not definitive
- Bone health in general Western populations on MK-7 (90–375 µg/day):
- Several RCTs and meta-analyses show improved vitamin K status and small BMD benefits in some cohorts, but fracture reduction evidence is lacking/inconclusive and results are not uniform.
- Periodontal / dental health:
- Newer epidemiology and serum-level studies show inverse associations between K (including K2) and periodontitis prevalence/severity. Causality unproven, and intervention studies are minimal and not impressive so far.
Weak / speculative
- Prostate health:
- One cohort suggests lower advanced prostate cancer risk with higher K2 intake; others are null. Preclinical data support antiproliferative effects in prostate cancer cell lines. No convincing clinical intervention data.
- Skin:
- Mechanistic plausibility (MGP in dermal elastic fibers, calcification stories) and a few observational hints, but no solid RCTs showing improved skin aging endpoints with K2.
7. Practical implications & caveats (non-personalized)
Doses studied:
- Japan osteoporosis drug dose (MK-4): 45 mg/day, usually split doses – very different from OTC supplements.
- Common supplement doses (MK-7): 90–200 µg/day; some RCTs used up to 375 µg/day.
Safety / interactions:
- K2 is generally well tolerated in trials; serious adverse events rare. GI upset is the main minor complaint.
- Critical: Any form of vitamin K (K1 or K2) can interfere with vitamin K antagonists (warfarin, etc.), so supplementation in those patients is not trivial and needs physician supervision.
Big-picture summary:
- If you’re looking at hard bone outcomes, the only robust data are high-dose MK-4 in Japanese osteoporosis patients.
- For prostate, gum/dental, and skin, we’re still in the interesting hypothesis / early signal stage. I’d treat K2 as “mechanistically promising, clinically under-proven” in those domains.
3 Likes
The longer menaquinones can can act as electron acceptors.
Been taking combo D3 and K2 at bedtime for the past 3 years. Showed some bone density improvement on my DEXA. Will see if bone density is still improving in January.
What Happens When You Take Vitamin D and K2 Together?
2 Likes
Most patients with Chronic Kidney Disease, including those, @LaraPo, with a renal transplant, are deficient in K2 and advised to consider supplementation.
2 Likes