For more than a decade, aging biology has been organized around a tidy checklist: the “hallmarks of aging,” a roster that has swollen from nine to twelve to fourteen separate molecular faults, from DNA damage to worn-out telomeres to exhausted stem cells. The list is useful as a filing system, but it has a nagging problem — it describes symptoms without explaining why they all show up together, or how to treat more than one at a time.
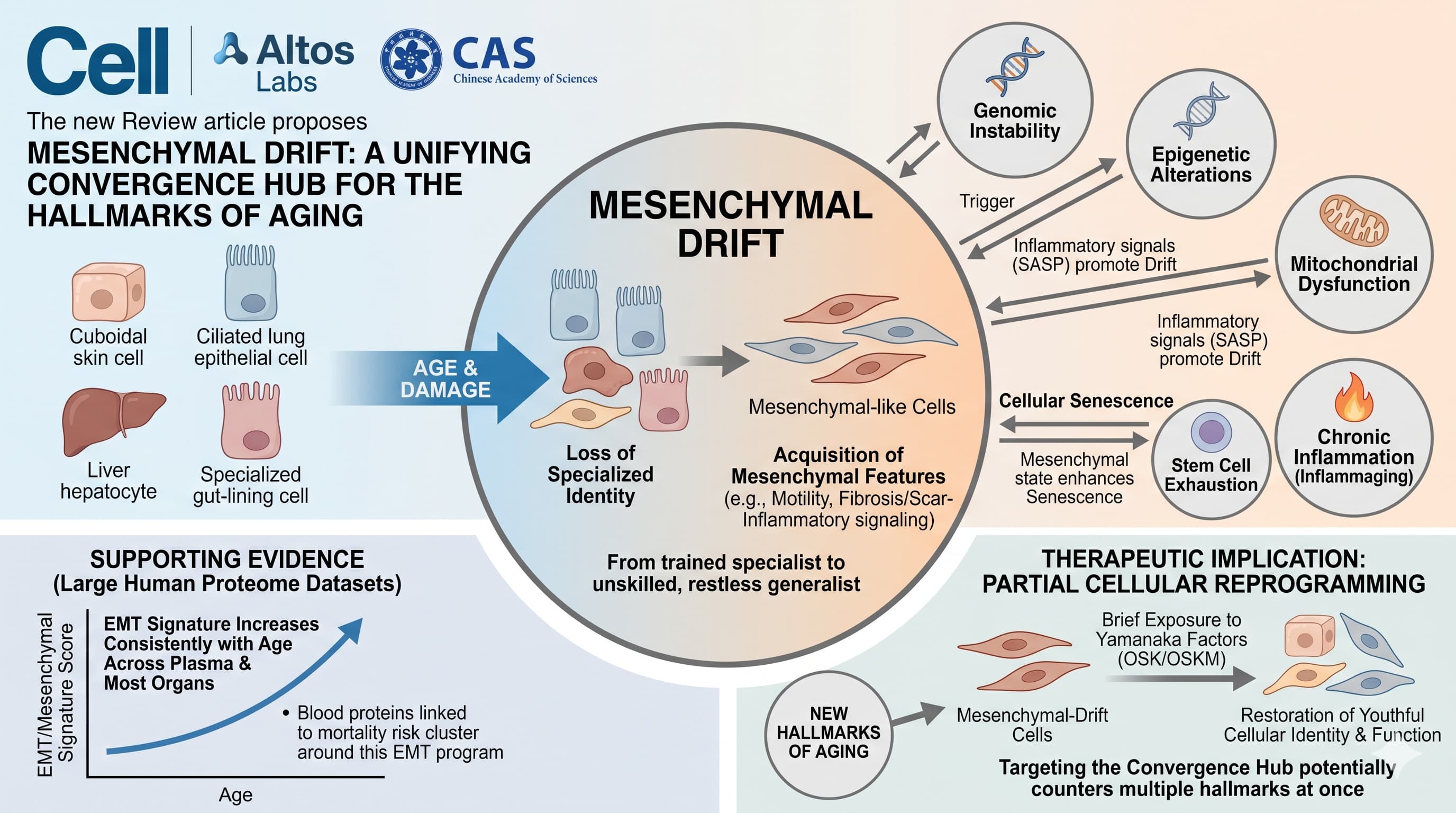
A new Leading Edge Review in Cell, from a team spanning Altos Labs in California and the Chinese Academy of Sciences in Beijing, proposes a single thread that may run through the entire checklist. They call it mesenchymal drift. The claim is that as tissues age, specialized cells — the skin, lung, liver, blood-vessel and gut-lining cells that do the actual work of an organ — slowly forget their identity and slide toward a generic, mobile, scar-producing “mesenchymal” state. Think of a trained specialist gradually reverting to an unskilled, restless generalist who lays down fibrous tissue and inflammatory signals instead of doing its original job.
The provocative part is the direction of causation. The authors argue mesenchymal drift is not just another item on the list but a convergence hub: nearly every classic hallmark — genomic instability, epigenetic change, failed protein recycling, broken mitochondria, deranged nutrient sensing, senescence, stem-cell exhaustion, chronic inflammation — can both trigger drift and be worsened by it, forming self-reinforcing loops. As supporting evidence they point to large human proteome datasets in which an “epithelial-to-mesenchymal transition” signature is among the most consistently age-upregulated features across plasma and most organs, and to the observation that blood proteins most strongly tied to mortality risk cluster around this same drift program.
If the framework holds, it reframes aging from a dozen leaks needing a dozen plugs into one underlying instability of cellular identity. That has a clear therapeutic implication the authors clearly favor: partial cellular reprogramming — briefly exposing cells to the Yamanaka factors (OSK/OSKM) to nudge them back toward their youthful identity without erasing it. Because drift sits where the hallmarks meet, hitting it could, in principle, counter several at once.
The honest caveat: this is a unifying hypothesis, elegant and well-referenced but not yet proven causal. “Mesenchymal drift” is a reinterpretation of existing data, not a discovery of a new molecule. Whether it is a true driver of aging or a particularly vivid description of it is the open question the paper itself cannot settle.
Actionable Insights
Because this is a conceptual review, take-homes are indirect — there is no protocol to copy. Still, several practical signals emerge, all consistent with mainstream geroscience rather than novel to this paper:
The strongest recurring lever is restraining the pro-fibrotic, mesenchymal program, and the interventions the authors repeatedly invoke are already familiar to this audience: mTOR inhibition (rapamycin) and AMPK activation (caloric restriction, exercise, and agents like metformin) both suppress drift in the cited models, which the authors suggest may partly explain rapamycin’s longevity effect. Autophagy support (fasting, exercise, mTOR suppression) counteracts the proteostasis collapse that feeds drift. NAD+ restoration is cited as easing mitochondrial dysfunction and one form of drift in preclinical work.
The broader theme worth internalizing: anti-fibrotic and anti-inflammatory living is anti-aging. Anything that lowers chronic low-grade inflammation, preserves mitochondrial fitness, and limits tissue fibrosis is acting on this proposed convergence node.
What you should NOT do is treat partial reprogramming as a near-term consumer intervention — it remains a research-stage, delivery-and-safety-unsolved technology with documented tumor risk in continuous-exposure animal studies.
Source:
- Open Access Paper: Mesenchymal drift: A convergent framework for the hallmarks of aging
- Institutions: Altos Labs, San Diego, California, USA; and the State Key Laboratory of Organ Regeneration and Reconstruction, Institute of Zoology, Chinese Academy of Sciences, Beijing, China.
- Country: United States / China (collaborative).
- Journal: Cell (Cell Press / Elsevier), Volume 189, May 28, 2026
- Corresponding authors: Guang-Hui Liu (IOZ, CAS) and Juan Carlos Izpisua Belmonte (Altos Labs).
- Disclosure flag: All authors are employees of Altos Labs or the Chinese Academy of Sciences. Altos Labs is a commercial longevity company whose flagship scientific bet is cellular reprogramming – the exact therapy this framework elevates. This is a legitimate conflict-of-interest consideration when weighing how strongly the review steers toward reprogramming as the answer.
- Impact: The impact score of this journal is 45.5 (JIF) / 74.8 (CiteScore) , therefore this is an Elite impact journal.
