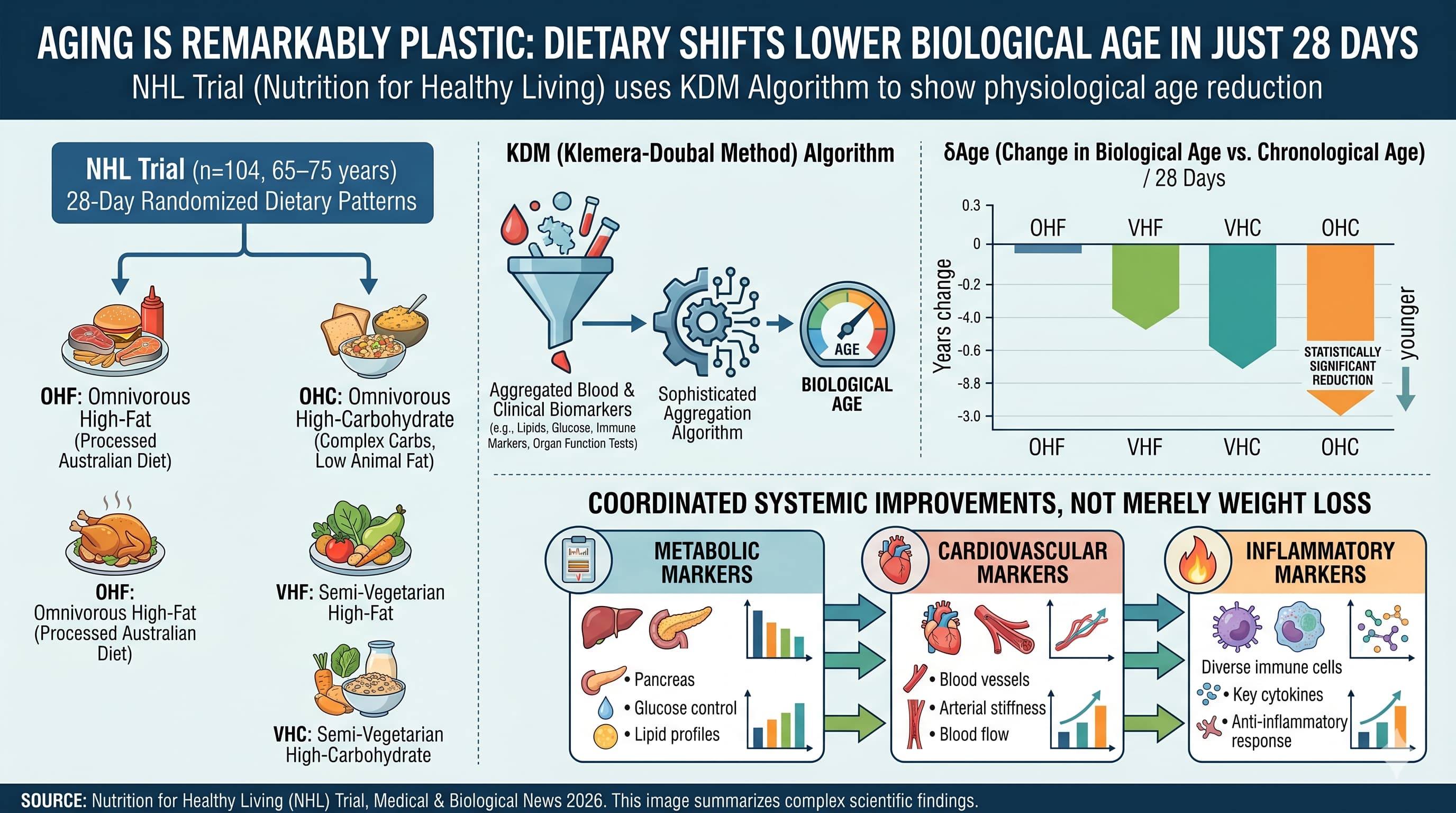
Biological aging is often viewed as a relentless, unidirectional progression of systemic decay. However, new research from the University of Sydney suggests that the “physiological speedometer” of aging is remarkably plastic, responding to dietary shifts in as little as 28 days. Utilizing the Klemera-Doubal Method (KDM) —a sophisticated algorithm that aggregates blood and clinical biomarkers into a single “biological age” score—researchers demonstrated that older adults can significantly lower their physiological age profile by altering macronutrient sources and ratios.
The study, known as the Nutrition for Healthy Living (NHL) trial, randomized 104 participants (aged 65–75) into four distinct dietary patterns: omnivorous high-fat (OHF), omnivorous high-carbohydrate (OHC), semi-vegetarian high-fat (VHF), and semi-vegetarian high-carbohydrate (VHC). While the OHF group—which mirrored the standard, highly processed Australian diet—showed no change in biological age, the other groups experienced measurable shifts toward “younger” physiological states. The OHC group, emphasizing complex carbohydrates over animal fats, emerged as the most effective, producing statistically significant reductions in δAge (the gap between biological and chronological age).
Critically, the research highlights that the benefits were not merely the result of weight loss but of coordinated systemic improvements in metabolic, cardiovascular, and inflammatory markers. While the investigators warn that a four-week trial cannot definitively prove “age reversal,” it does confirm that biological age estimates are highly sensitive to acute nutritional inputs. This suggests that KDM-based metrics could serve as a “real-time” barometer for longevity interventions, allowing individuals to gauge the efficacy of lifestyle changes long before chronic diseases manifest. The findings reinforce a growing consensus in longevity science: the composition of the plate acts as a biochemical signaling kit capable of rapidly modulating the body’s functional state.
Actionable Insights
-
Prioritize Complex Carbohydrates: Shifting from a high-fat, meat-heavy diet to one rich in complex carbohydrates (legumes, whole grains, and starchy vegetables) is the most robust lever for lowering KDM-based biological age estimates.
-
Emphasize Fiber and Plant-Forward Eating: Diets that diverged most from baseline in fiber and fat content (moving toward higher fiber and lower animal fat) produced the greatest physiological benefits.
-
Short-Term Changes Matter: Systemic biomarkers of aging can improve in as little as four weeks, providing early positive reinforcement for dietary adherence.
-
Monitor Systemic Integrity: Use biological age calculators (like KDM) rather than just single markers like glucose or cholesterol to understand how diet affects overall “systemic health”.
-
Beware of Processed “Normalcy”: The “standard” diet (high in processed foods and saturated fats) acts as a baseline for accelerated aging; even “healthy” omnivorous patterns benefit from higher complex carb ratios.
Source:
- Open Access Paper: Short-Term Dietary Intervention Alters Physiological Profiles Relevant to Ageing
- Institution: University of Sydney, Charles Perkins Centre.
- Country: Australia.
- Journal Name: Aging Cell, 27 April 2026
- Impact Evaluation: The impact score of this journal is 11.0 (based on current 2024-2025 trends), this is a High impact journal in the field of gerontology and cell biology.