Resistance exercise (e.g. weight training) is often sidelined in female health discussions, yet new research argues it is a critical determinant of longevity and functional independence. This paper, published in ACSM’s Health & Fitness Journal by researchers from The College of New Jersey (USA), the University of Bologna (Italy), and Monmouth University (USA), introduces the “Female Strengthspan”—a quantitative metric of muscular strength across the lifespan that directly influences health outcomes and life expectancy.
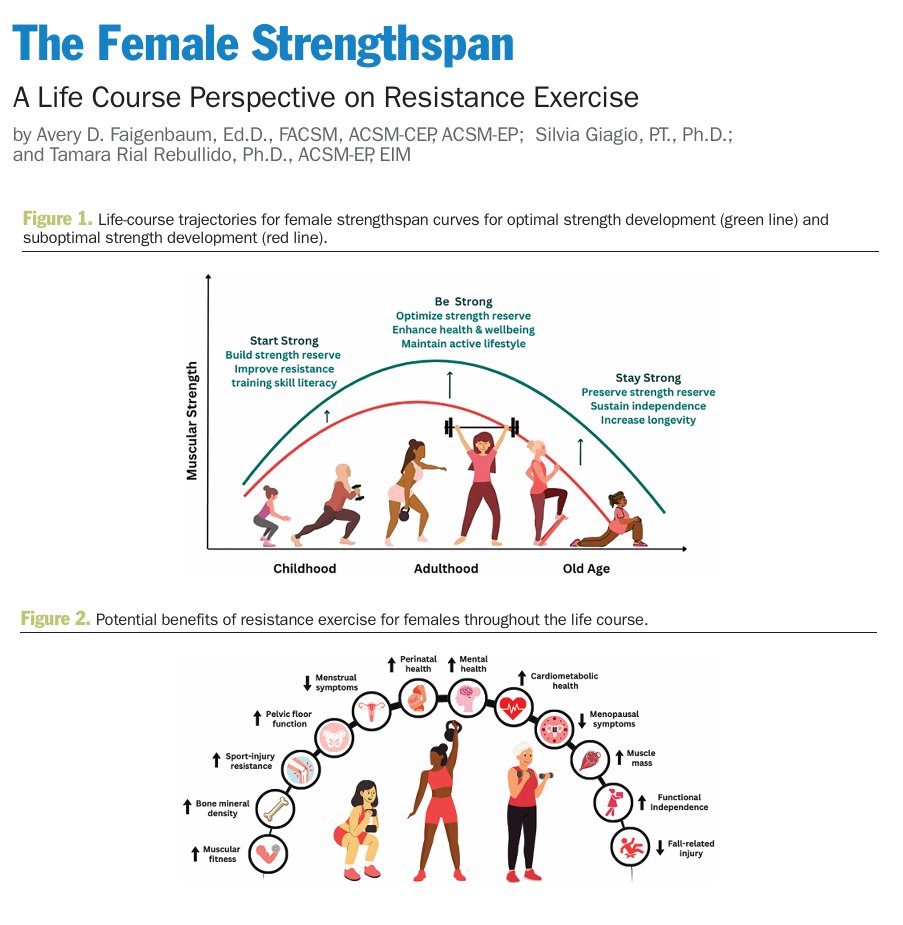
The “Big Idea” is the establishment of a “strength reserve” early in life to buffer against age-related decline. The authors argue that childhood and adolescence are critical windows for weight-bearing activities to maximize bone mass and neuromuscular coordination. For adult women, resistance training extends beyond aesthetics, significantly impacting cardiometabolic health, mood regulation, and pelvic floor integrity. In older age, it becomes a primary defense against dynapenia (loss of strength) and fall-related injuries.
Source:
- Open Access Paper: The Female Strengthspan - A Life Course Perspective on Resistance Exercise
- Impact Evaluation: The impact score (CiteScore) of ACSM’s Health & Fitness Journal is approximately 1.6, evaluated against a typical high-end range of 0–60+ for top general science, therefore this is a Medium impact journal within the specialized field of sports medicine and clinical exercise.
Part 2: The Biohacker Analysis
Study Design Specifications:
- Type: Narrative Review / Clinical Perspective.
- Subjects: Human females across the lifespan (Youth <18, Adulthood 18-64, Older Age ≥65).
- Lifespan Analysis: This study focuses on human healthspan and functional longevity rather than murine lifespan. However, it notes that <60 minutes of resistance training weekly is associated with reduced all-cause mortality Muscle-strengthening activities and mortality (2022).
-
Mechanistic Deep Dive:
- Neuromuscular: Counteracts age-related denervation and preserves neural innervation of Type 2 (fast-twitch) myofibers Resistance training for older adults (2019).
- Metabolic: Enhances glucose disposal and improves cardiometabolic markers Evolution of resistance training in women (2025).
- Endocrine/Vascular: Modulates vasomotor symptoms (hot flashes) in menopause through improved circulation and hormone regulation Resistance training and vasomotor symptoms (2024).
- Organ Priority: Specifically highlights the Pelvic Floor as a specialized target for resistance exercise to maintain core stability and continence Pelvic floor muscle training: mechanisms (2020).
Novelty: The paper conceptualizes strength as a “bank account,” where early “deposits” (training) yield “compound interest” in late-life resilience. It specifically addresses the “mythology” of female training, debunking cycle-based training requirements and the “bulky” muscle growth fallacy.
Critical Limitations:
- Translational Uncertainty: While epidemiological data links strength to longevity, the specific “minimum effective dose” for lifespan extension remains debated.
- Methodological Weakness: As a clinical review, it synthesizes existing literature rather than providing new RCT data.
- Data Gaps: Lacks specific molecular signaling data (e.g., impact on cGAS-STING or specific autophagy markers) compared to pharmaceutical longevity interventions.