What is your propranolol dose?
20 mg morning, 20 mg lunch, 40 mg before bed
I take it occasionally for headache prophylaxis, 40-80mg, but it decreases my max. heart rate significantly. I read some studies that lactate output and muscle benefit is same as without but still makes me wonder if CV benefits are diminished, since my max heart rate drops around 20 bpm.
Otherwise I really like propranolol, the effect it has on nervous system, helps if stressed and with anxiety too. I also noticed that it drops significantly my BP.
Max heart rate (MHR) is apparently not an indication of fitness. MHR is predominantly genetically determined and does not increase as your fitness level raises. Although the length of time you can sustain your MHR does increase with fitness. And although beta-blockers reduce MHR, and this might impact the performance of elite athletes, Harvard Health says “your beta blocker won’t prevent you from getting the positive effects of exercise. You will still build muscle, keep your bones strong, and lower your cholesterol and blood sugar levels. You’ll also improve your heart’s efficiency and endurance.”
3 Likes
1 Like
Carvedilol vs nebivolol: which one is best?
In the ITP, nebivolol “was also found to produce a female-specific decline (4%, p = 0.03) in lifespan”. In males, there was also a borderline significant lifespan shortening. (poke @LukeMV) The ITP used 60 ppm, so 10 mg/kg body weight/day, so about 1 mg/kg for a human? That’s a lot! A previous study that used a lower dose (1 mg/kg body weight/day, for about 0.1 mg/kg for a human close to the average daily dose of 5 mg/day) found that: “The β-blockers metoprolol and nebivolol, administered in food daily beginning at 12 months of age, significantly increase the mean and median life span of isocalorically fed, male C3B6F1 mice, by 10 and 6.4 %, respectively (P < 0.05).” (β1-Adrenergic receptor blockade extends the life span of Drosophila and long-lived mice 2013) For metoprolol they used 30 mg/kg body weight/day, which is also close to the daily human dose (150 mg/day). So if you trust this earlier study, metoprolol is better than nebivolol at the normal human doses.
On the other hand, carvedilol led to a +25% but NOT statistically significant lifespan increase in the Ora Biomedical challenge. It worked wonders in early age but then had a detrimental effect:
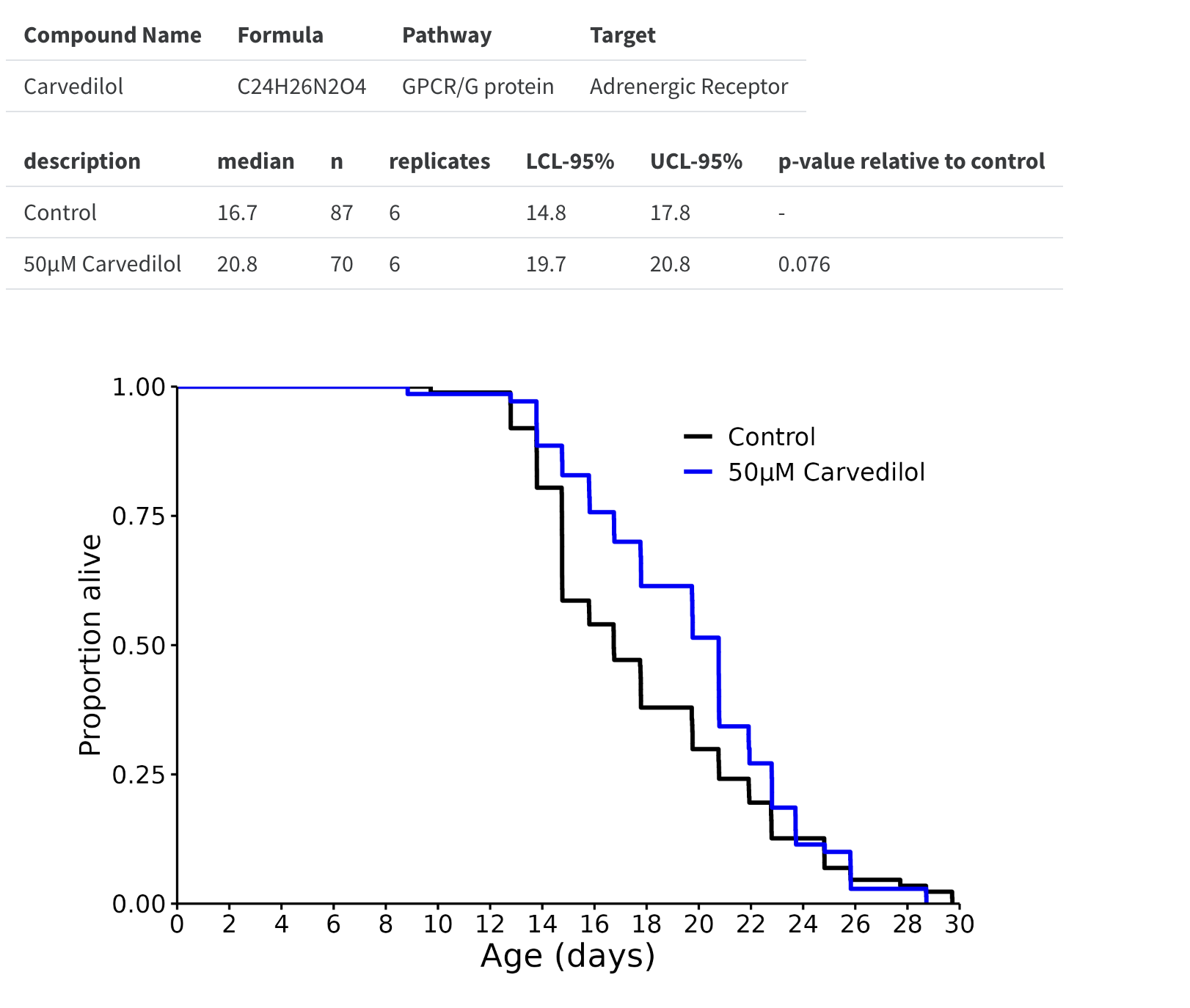
(I think resting heart rate starts decreasing from age ~60, so maybe carvedilol shouldn’t be used in healthy people past that age? Or maybe it should only be used to reach a given resting heart rate threshold?)
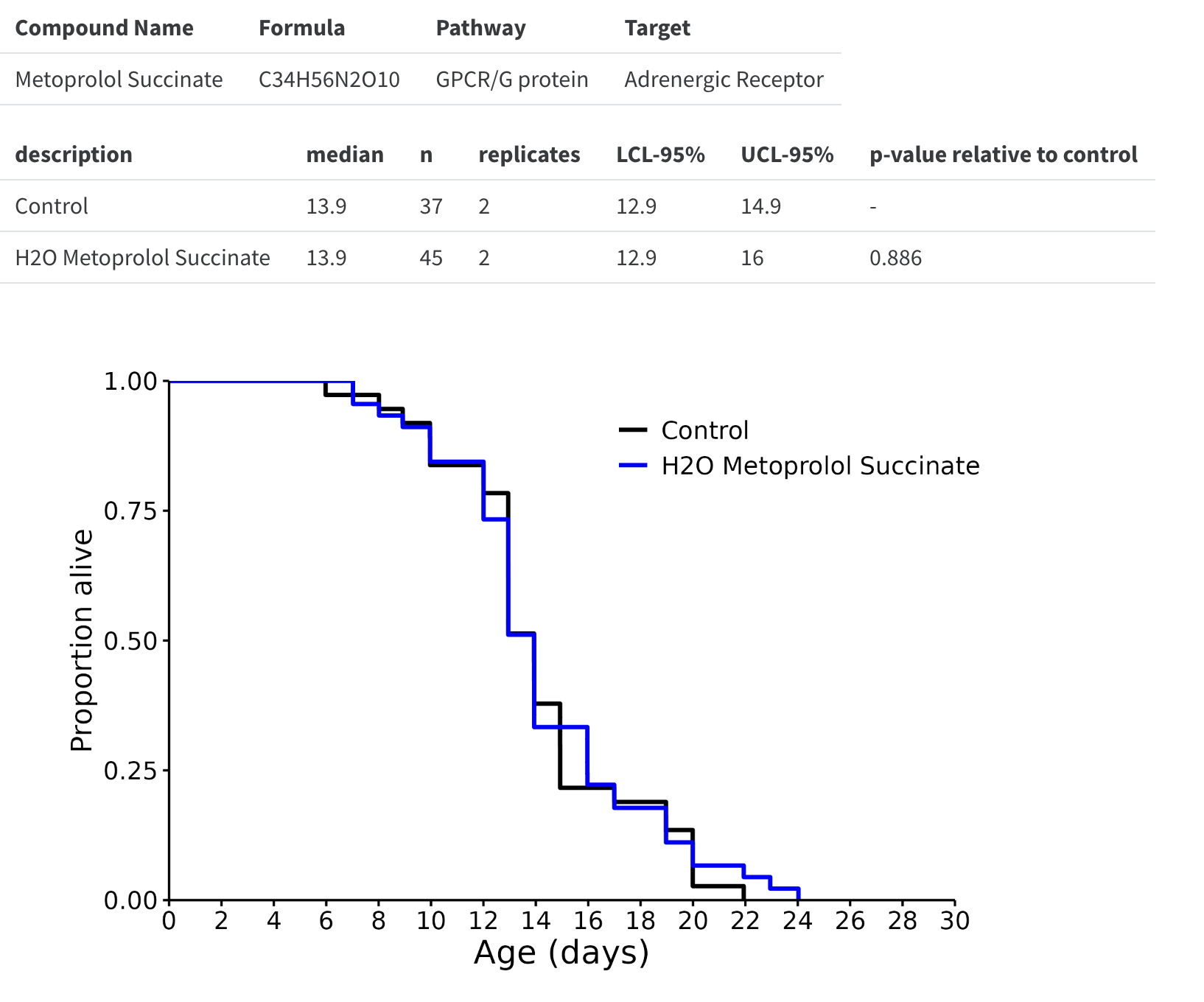
Metoprolol was tested but at a dose probably too low, so nothing happened:
According to Meta-Analysis of Carvedilol Versus Beta 1 Selective Beta-Blockers (Atenolol, Bisoprolol, Metoprolol, and Nebivolol) 2013: “Compared to β1-selective BBs used in HF (8 trials, n = 4,563), carvedilol significantly reduced all-cause mortality (risk ratio 0.85, 95% confidence interval 0.78 to 0.93, p = 0.0006). In 3 trials of patients with AMI (n = 644), carvedilol significantly reduced all-cause mortality by 45% (fixed-effects model: risk ratio 0.55, 95% confidence interval 0.32 to 0.94, p = 0.03, random-effects model: risk ratio 0.56, 95% confidence interval 0.26 to 1.12, p = 0.10), with no reduction in non-fatal MI (risk ratio 0.61, 95% confidence interval 0.31 to 1.22, p = 0.16). In conclusion, carvedilol, as compared against atenolol, bisoprolol, metoprolol and nebivolol in randomized direct comparison trials, significantly reduced all-cause mortality in systolic HF patients.”
One reason given to use nebivolol compared to other beta-blockers is the potential beneficial effect on erectile function. However, according to this paper (Effects of major antihypertensive drug classes on erectile function: a network meta-analysis 2022), although nebivolol might be better than non-vasodilatory beta-blockers (such as bisoprolol and metoprolol), there’s no difference between nebivolol and other vaso-dilatory beta-blockers (carvedilol and labetalol) in terms of erectile function.
Nebivolol is still the only beta-blocker that can increase nitric oxide. And carvedilol has a shorter half-life so it’s taken twice daily. Some countries have carvedilol SR, once daily. So there’s a tradeoff…
4 Likes
Great information.
So the ITP used ridiculously high dosages of Nebivolol that a human would never take, which doesn’t make sense to me. What is the point of that? The older rat study and worm studies you mentioned seem to have more credibility since the correct dosages were used.
Combine that with the fact that mice and worms don’t die from heart related problems, which beta blockers are used for. Therefore, I am not sure how much merit I will put into non human studies when it comes to beta blockers.
Cardevilol vs Metoprolol vs Nebivolol remains an interesting debate.
4 Likes
Yes, on this see also this post: Rilmenidine vs Telmisartan or other BP meds for Longevity - #93 by adssx
1 Like
Claude just suggested it to reduce HR increases from concerta
I like metoprolol, and I have been taking it for ~25 years. I would have to see some really significant studies that Nebivolol was significantly superior before I would change.
I take metoprolol in the evenings and telmisartan in the mornings.
“Metoprolol has been prescribed for nearly 50 years and has a long-standing, well-established safety record.”
“One of the most important clinical trials that demonstrated the efficacy and safety of metoprolol was the Metoprolol Randomised Intervention Trial in Congestive Heart Failure (MERIT-HF), conducted between 1997 and 1999. This multicenter, double-blind, placebo-controlled trial enrolled 3991 patients with chronic heart failure who were randomized to receive either metoprolol succinate (a long-acting formulation) or placebo in addition to standard therapy. The primary endpoint was all-cause mortality.[4] The results showed that metoprolol succinate reduced the risk of death by 34% compared with placebo over a mean follow-up of 1 year. Metoprolol succinate also reduced the risk of hospitalization for worsening heart failure by 19% and improved the patient’s symptoms and quality of life. The drug was well tolerated and did not cause any serious adverse events.” ref
2 Likes
I never tried Metropolol, but like how Nebivolol works (take 2.5 mg, lowest dose. It also adds nitric oxide. Telmisartan in the morning works well as well.
1 Like
I do think Nebivolol is better. It is also free of some of the side effects Metoprolol can cause (like impaired cardio fitness)
Here is a brand new study
2 Likes
Not enough to convince me to change since I have been doing fine with metoprolol.
“Although these findings suggest potential benefits of nebivolol in this population, prospective studies are needed to validate these observations.”
1 Like
I’m so glad to finally see a study (in a top-tier journal!) that shows improved long-term outcomes from nebivolol vs other beta blockers. On paper it’s seemed so much better for years and years, but the problem has always been the lack of data on outcomes.
Other side effects that nebivolol doesn’t have vs other beta-blockers: sexual dysfunction and increased insulin resistance.
3 Likes
“Here is a brand new study”
The quote made was from that study. Did I read it wrong?
IMO yes. You’ll be waiting for prospective trials that likely will never happen for a generic medication that has now been on the market for decades.
A heads-up. Like other beta blockers, nebivolol is contraindicated for an RHR of 55 or less.
I was taking it for years but it gets my diastolic BP number in the 50s (not heart rate) so I quit taking it. My BP is already borderline now without anything.
At your age and fitness level, the low BP is probably benign.
1 Like
Yes it was 109/63 this morning so I am not worried about it