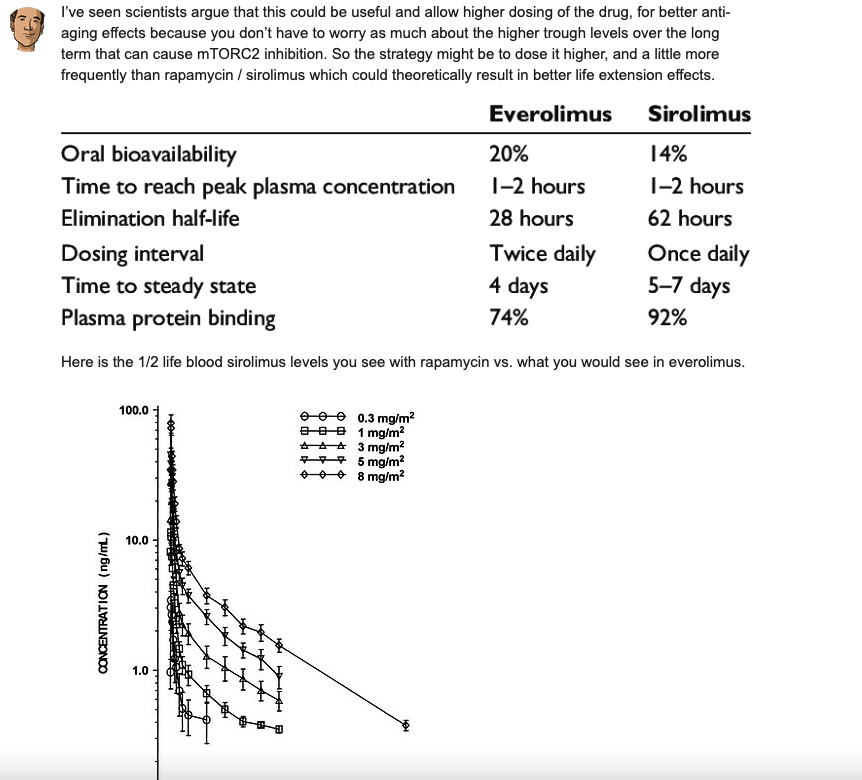
Any benefits drawback to taking my Rapamycin on an empty stomach? I’ve been taking my dose at right after dinner. I usually eat OMAD or one meal a day and dinner it is. Also, just wondering if perhaps the MTOR effect is blunted or enhanced based on feeding state? Just curious what everyone thoughts are?
1 Like
Not really, just that you might be missing a 30 percentage boost in bioavailability if taken with a fatty meal (I take it with sardines, other people here do a shot of olive oil)
4 Likes
Would cooking with butter suffice?
Edit: Thank you on Bioavailability. I did not know this!
1 Like
I don’t know exactly how much fat is required to increase bioavailability… You may want to review this paper: The Effect of a High-Fat Meal on the Oral Bioavailability of the Immunosuppressant Sirolimus (Rapamycin)
Full paper here: Sci-Hub | | 10.1177/009127009903901107
3 Likes
The bottom chart is why I fast when I take Rapa. I want that high peak and then to drop away. I continue fasting for 12 more hours as a part of my weekly 24 hour fast. The fast is more of a body fat control mechanism than a big autophagy boost. But since I can’t workout hard around rapa, this is the time for a fast.
From the paper in this thread

7 Likes
This made me think of something. I normally eat breakfast shortly after I take rapamycin. But if I were going for other bloodwork and getting my rapamycin checked at the same time for efficiency, I would just go 2 hours after the rapamycin, fasted, and get all the labs drawn at once. Of course that means my rapamycin measurement would be different than it would be on a typical day when I would not fast for 2-3 hours after taking the rapamycin. I guess early 20th century physics had it right when they pointed out that taking a measurement impact the thing being measured.
1 Like
This does not change much as it’s the rapamycin blood concentration, not the organs concentration. If you absorb it faster it also diffuse faster into the organs but the then elimination time is the same. The only meaningful difference is that the fasted vs high fat has a faster absorption but with less bioavailability so you get less of it but for a similar time.
BTW I’m currently working on a 3 compartment pharmacokinetic model from this paper data. I will post it very soon.
3 Likes
Ive never seen any data on organ residence time for rapa. But until I learn more, I like my fasting curve better than the fat curve plus I get to time my fast with my rapa downtime.
What will your model show?
1 Like
Just a quick question on basic methodological concerns: ‘on empty stomach’ means X hours your after last meal, but how many is X?. 4, 6, 8 hours? It depends on the size of the meal?. What I guess is that you need to only have your stomach empty but not your whole digestive tract, am I right?.
Does it also mean you can take your, lets say, rapa dose and inmediately have your meal or is it better to wait, for sample, 30 mins. before eating your food, so your rapa would fully enjoy its emptiness for a while and therefore, perhaps, get better absorbed?.
I am in your expert hands …
1 Like
If the goal is fast absorption for a higher peak but smaller AUC (my goal, by the way, which might be the wrong way to go), then I would fast (except for gfj if that is a part of the program) for at least 12 hours and then not eat for another 3-12 hours (24 hours total) plus do some easy cardio after dosing. Yesterday I experimented with a 18 hour fast (dinner the night before until 3pm) before Rapa and then ate a small low protein meal 3 hours later and then walked a mile. Had good but short sleep. Today I ate a low calorie, low protein breakfast. I can still feel the Rapa fatigue so it hasn’t cleared as quickly as I like.
1 Like
I don’t know whether we should guide ourselves by the ITP protocol in mice, but for what it’s worth, the rapamycin was mixed in with the chow, so the mice definitely took rapa with food - and the rapa was in small enteric covered units that had to be developed especially for that purpose (such small dose units didn’t exist, so a specific company was formed to develop and market these, I believe they still exist and animal research labs use them; they are commercially available). But the mice also took the rapa on a daily dose, so quite a different schedule from what most here favor.
But there are several questions here. The usual, about how the dosage scheduling translates from mice to humans. But also, we don’t actually know if this dosage and scheduling, and food variable that the ITP protocol used is in fact optimal for the mice. There is a factor of convenience and practicality in labs that may be quite different from strictly optimal for results.
The other guide might be the rapa analogue trial in humans that Mannick did, but unfortunately I don’t know what the protocol was around the taking of the drug - maybe someone here knows? Again, we don’t know if it was optimal, but at least it’s a real life one in humans, where we know the outcomes, with the caveat it was an analogue, not rapa.
2 Likes
To maximize the biologic effects of the rapamycin, you want to slow down its absorption, so it’s better to take it with a fatty meal. Taking it on an empty stomach will increase the blood concentration peak but will also increase its elimination so that when it is distributed to the organs you get less of it.
In the blood, rapamycin binds at 94% to the red blood cells who are short lived (120 days), don’t have mitochondria and lysosomes so don’t use autophagy. Basically they don’t care about rapamycin so people should not care about the initial blood peak either.
Basically you want to move the rapamycin from the initial container (GI tract) to its destination (organs) by going trough an intermediate container (the blood).
If you use wide buckets for the transport, it’s very fast but you are going to spill part of it. If you use narrow opening bottles it takes more time but you have much less waste.
6 Likes
This seems to be contrary to previous conclusions, which were that the benefit comes from its maximum blood concentration and the side effects come from its half-life, as persistent mtor1 inhibition ultimately leads to mtor2 inhibition
Also, the half-life of everolimus is shorter than that of rapamycin, does this mean that everolimus is more effective than rapamycin? Or worse? Thanks. @cl-user
1 Like
The benefits come from the peak in the organs not the peak in the blood. If you slow down the absorption with fat for instance, you increase the amount in the organs. You can combine that with GFJ to ensure an even greater amount is absorbed.
The half life varies with individuals and people should measure their own and use it to determine how long to wait between doses.
2 Likes