I’m implementing a 3 compartments pharmacokinetics model.
The compartments are :
The intestine that absorbs the rapamycin and send it into the blood
The blood is the central compartment that gets the rapamycin from the intestine and has bidirectional exchanges with the organs as well as some elimination (by metabolization)
The organs which exchange Rapamycin with the blood (both ways)
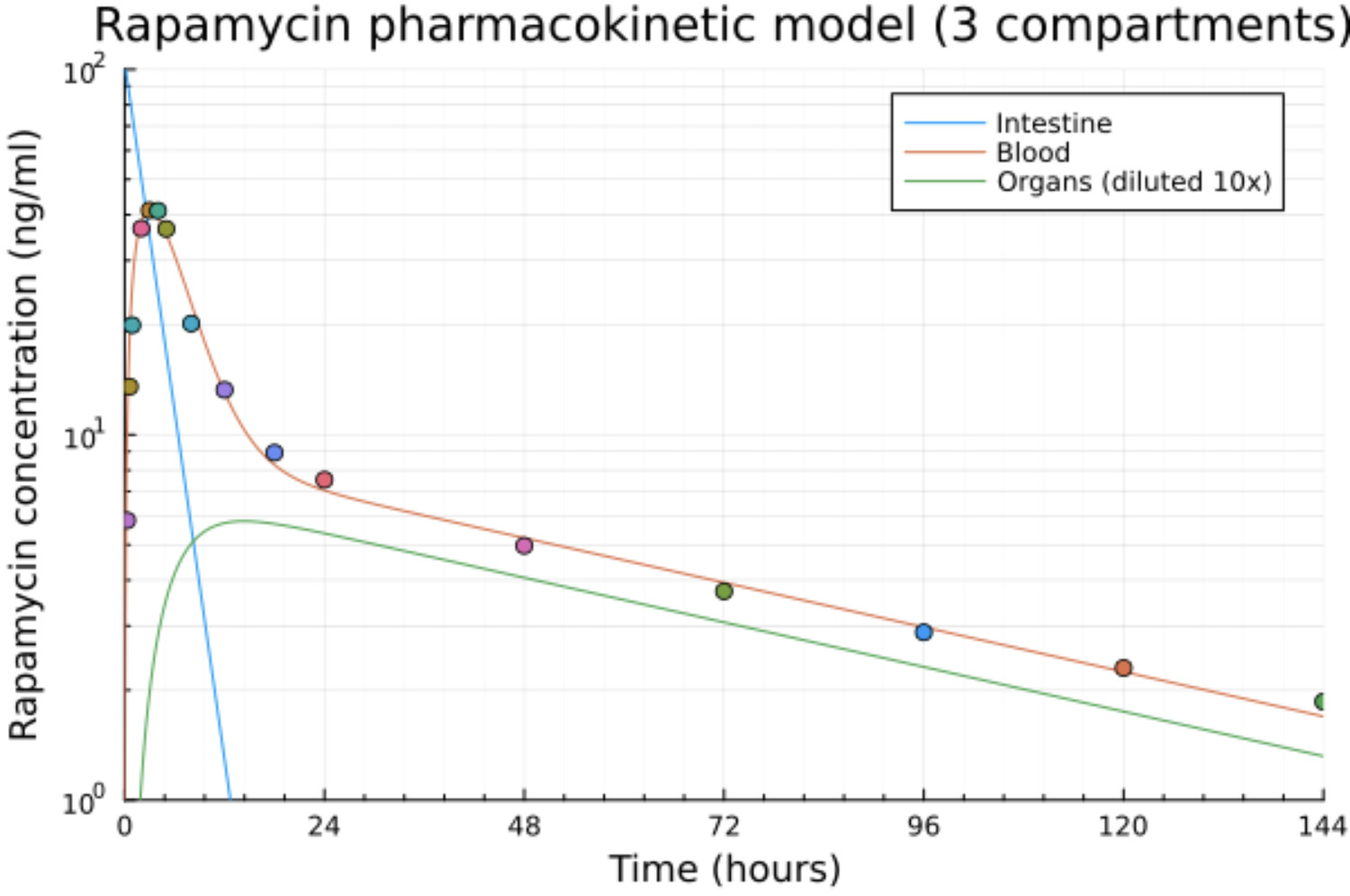
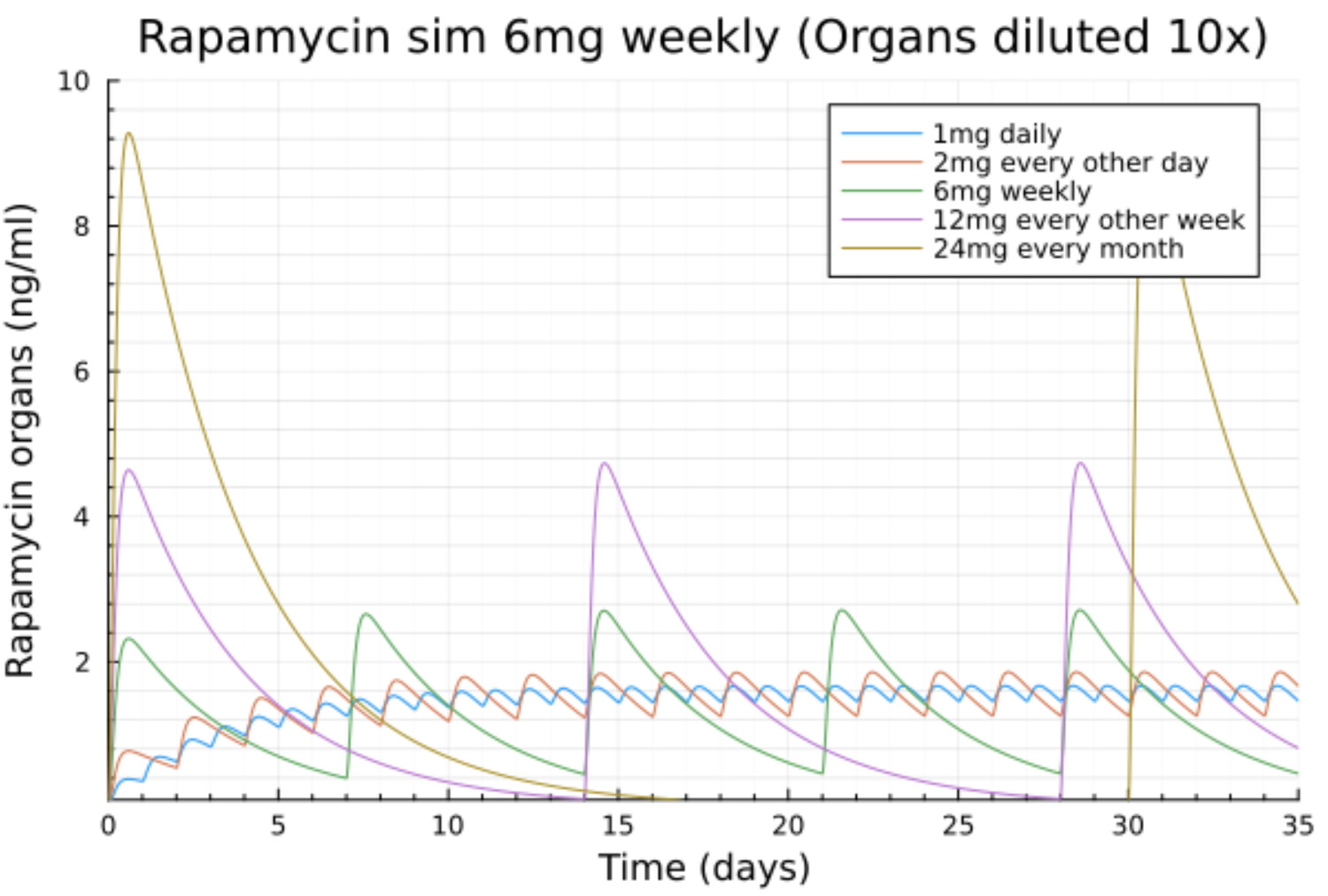
Here is that model with the differential equations fitted to the paper data for rapamycin + fat (dots)
As you can see the fit is very good which shows that the 3 compartment model is good enough.
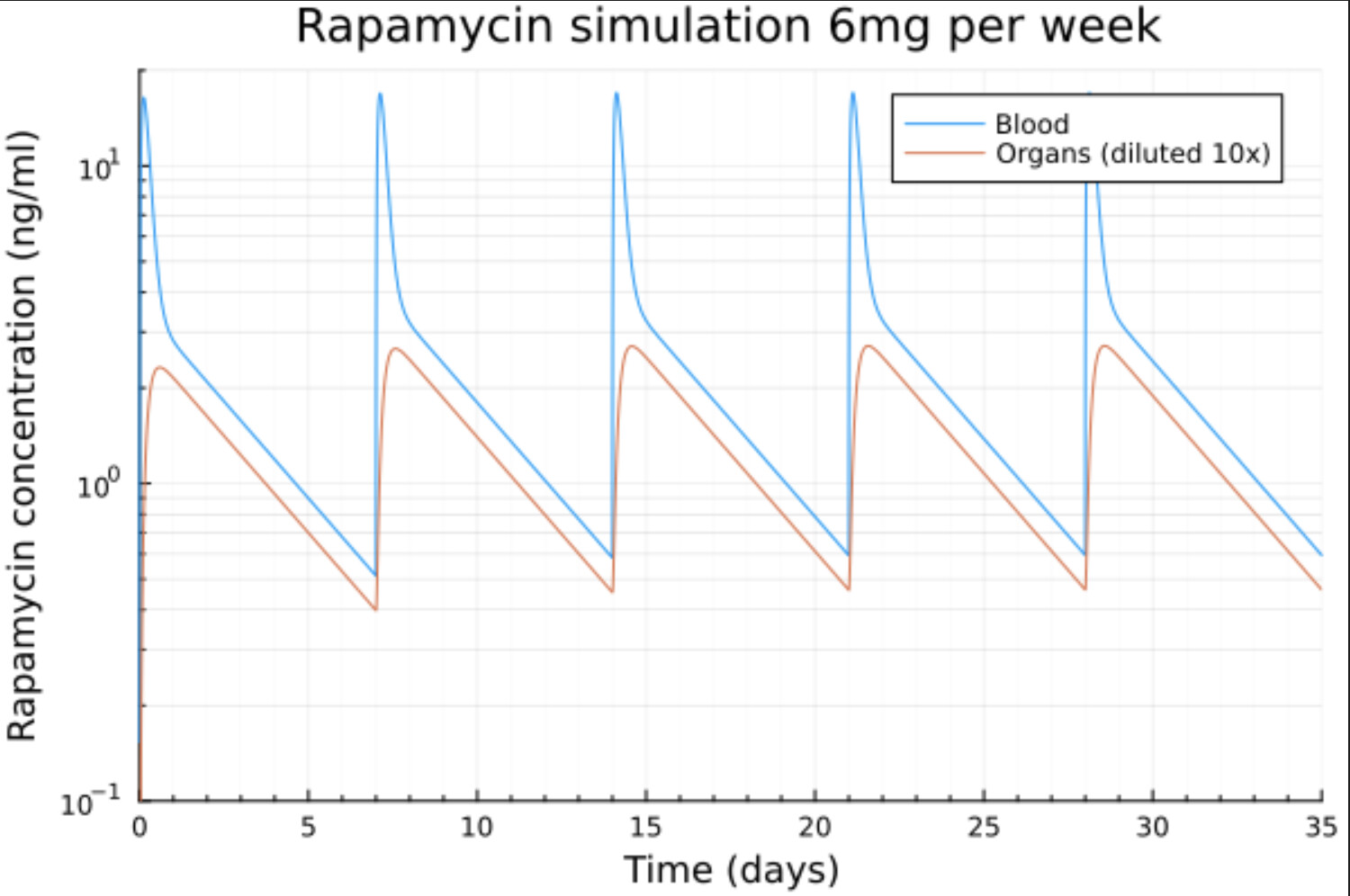
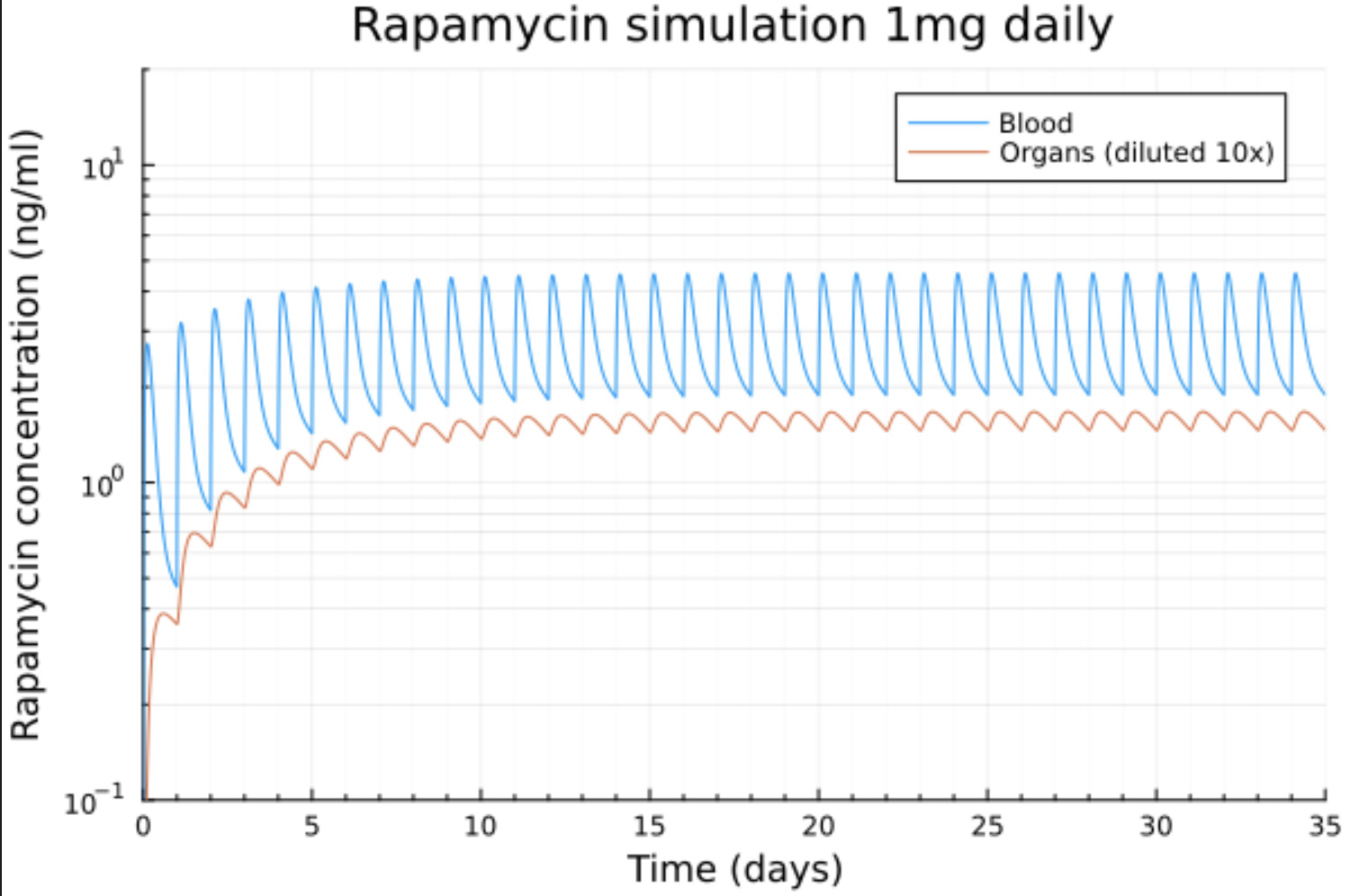
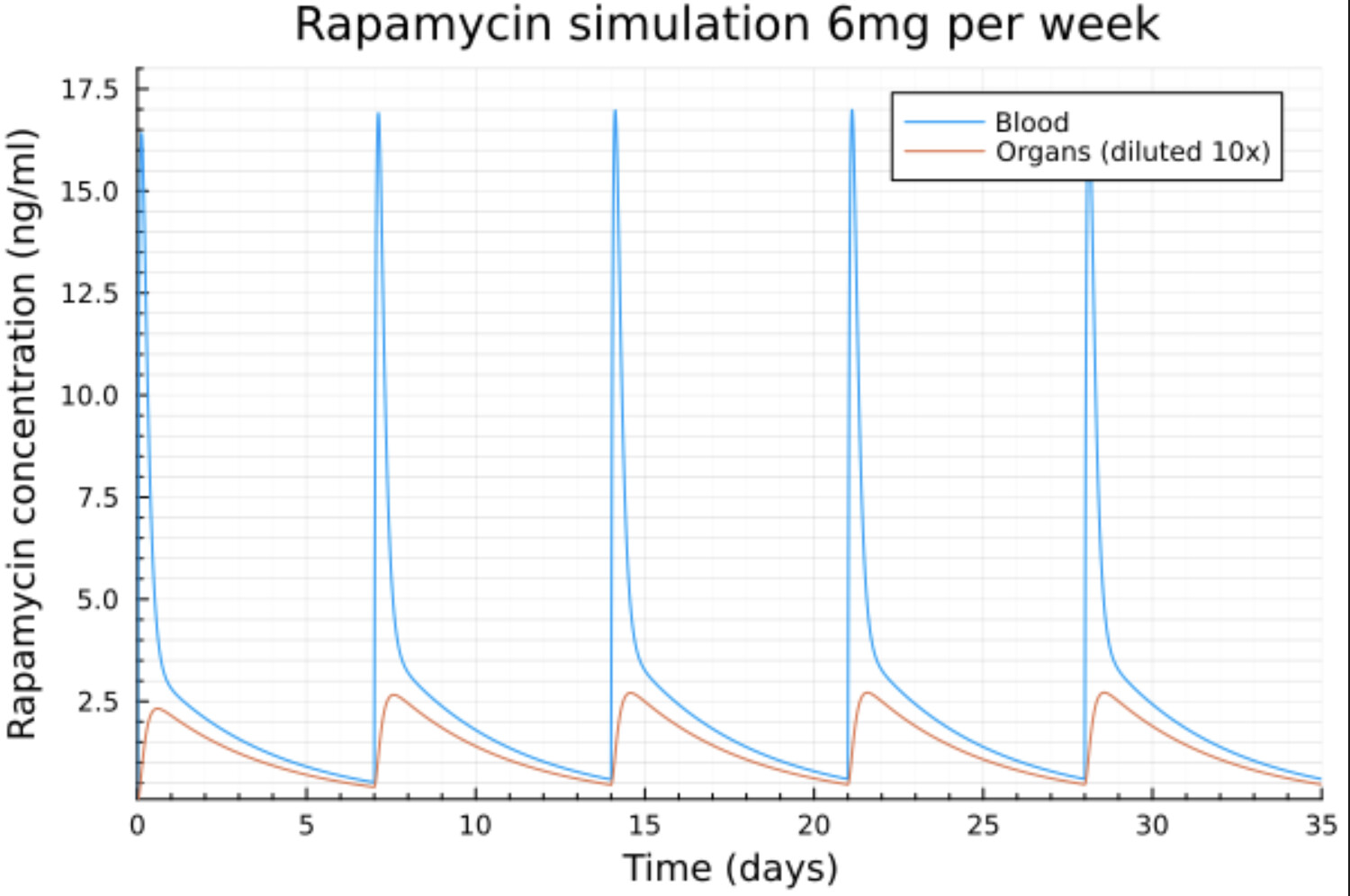
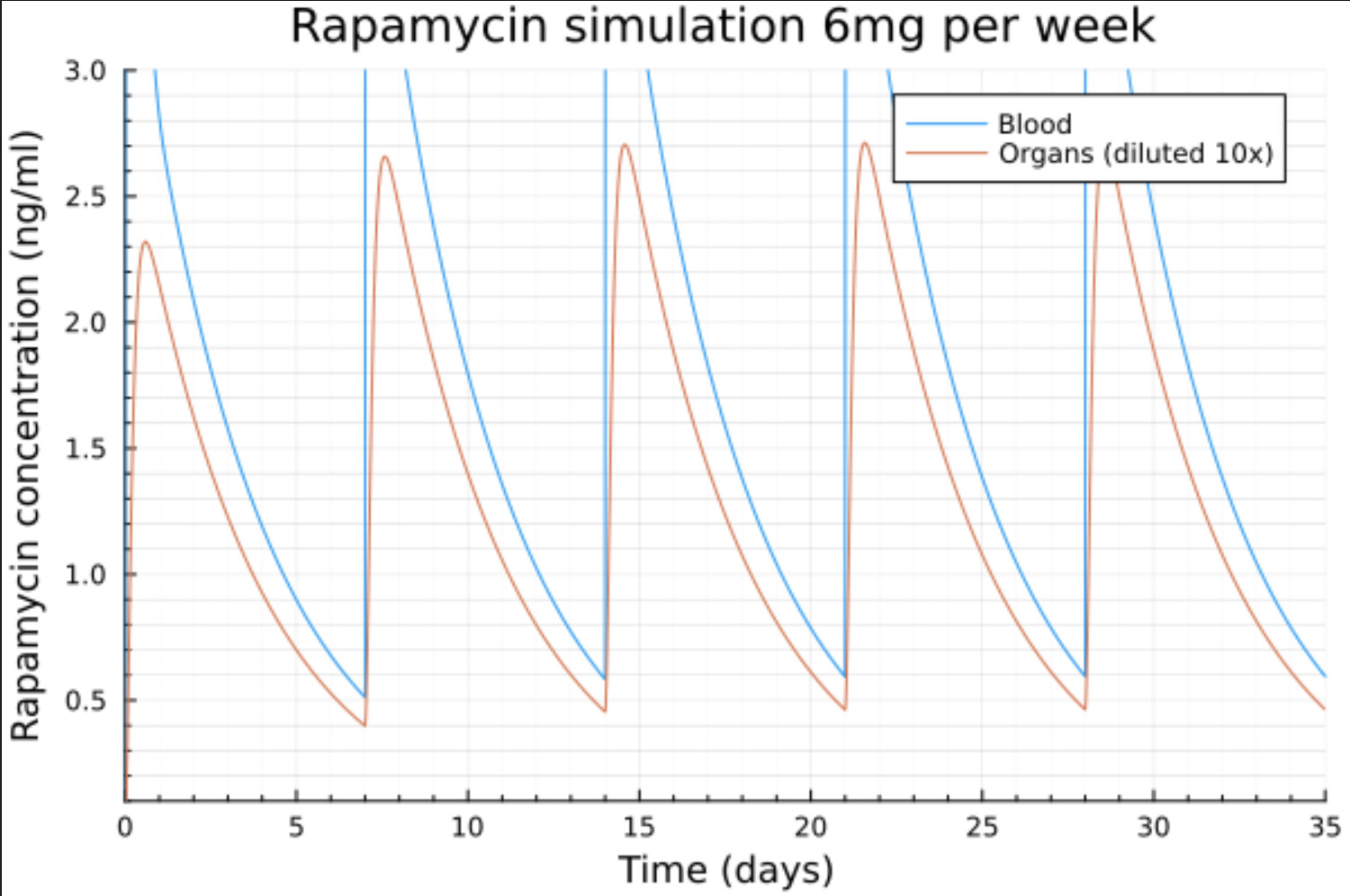
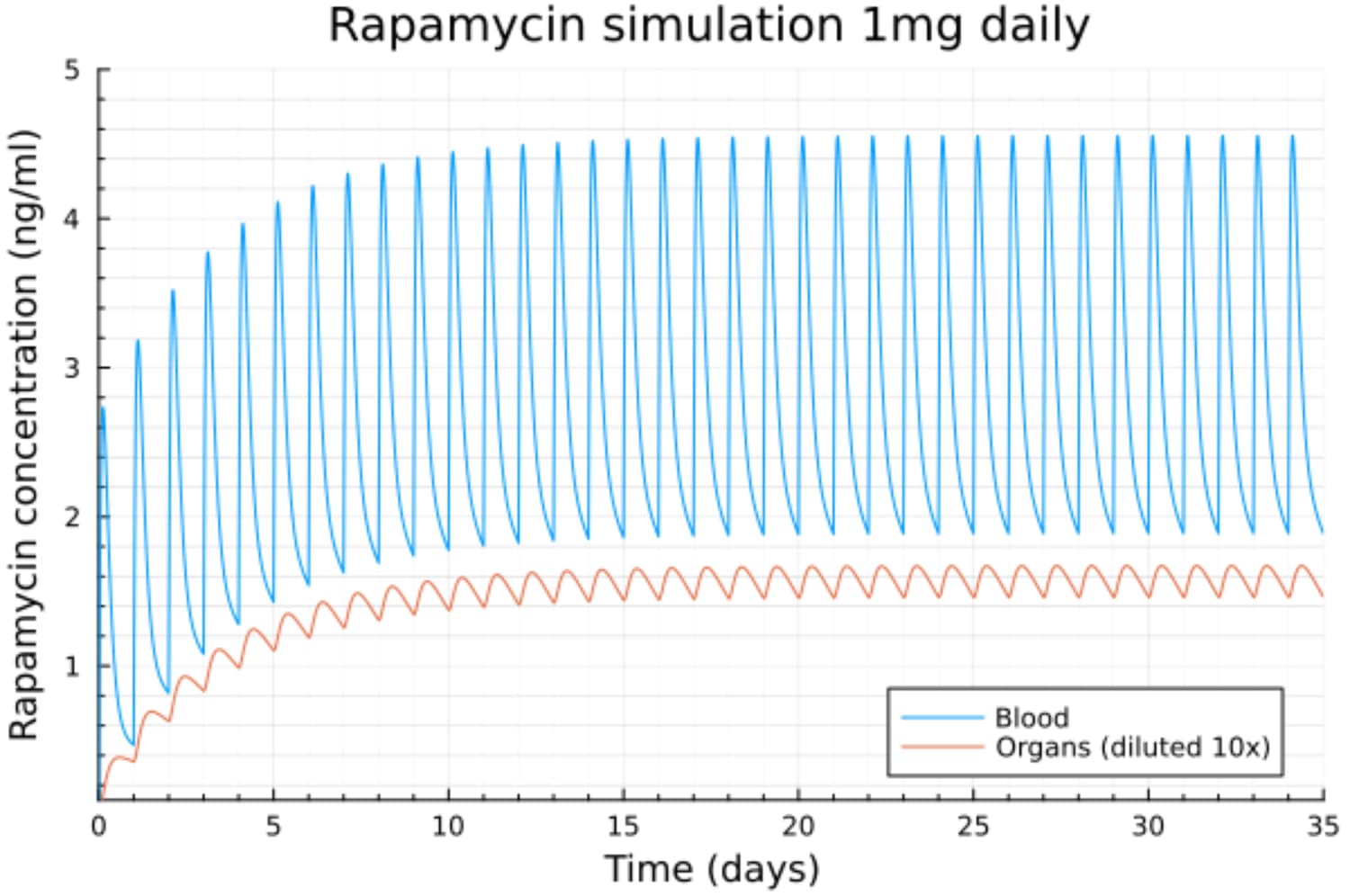
As this model is based on differential equations I can (and will!) use it to simulate some popular dosage scenarios.
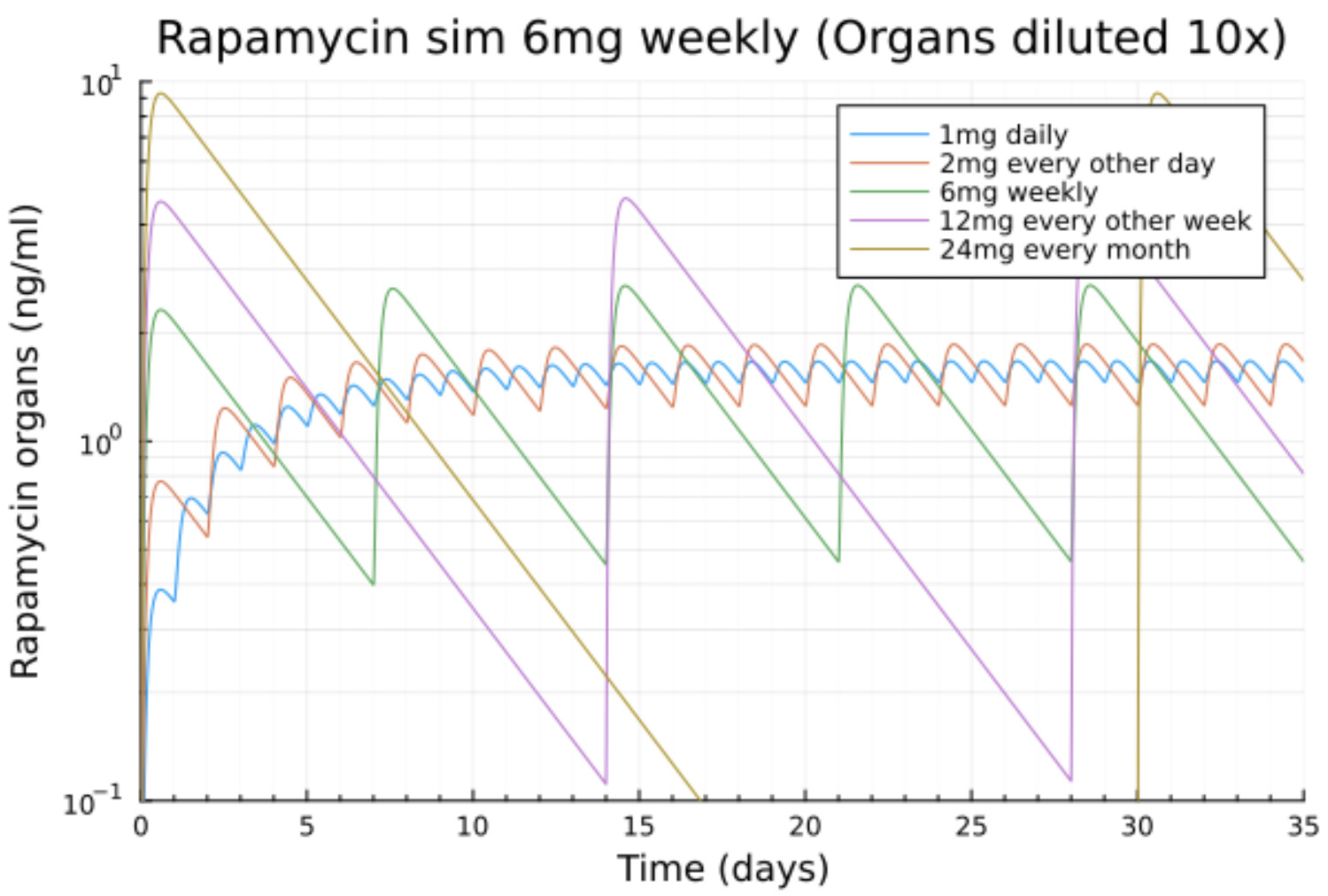
BTW in addition to the blood concentration this model gives the concentrations in the organs too, which if probably even more interesting, though there are some caveats here.
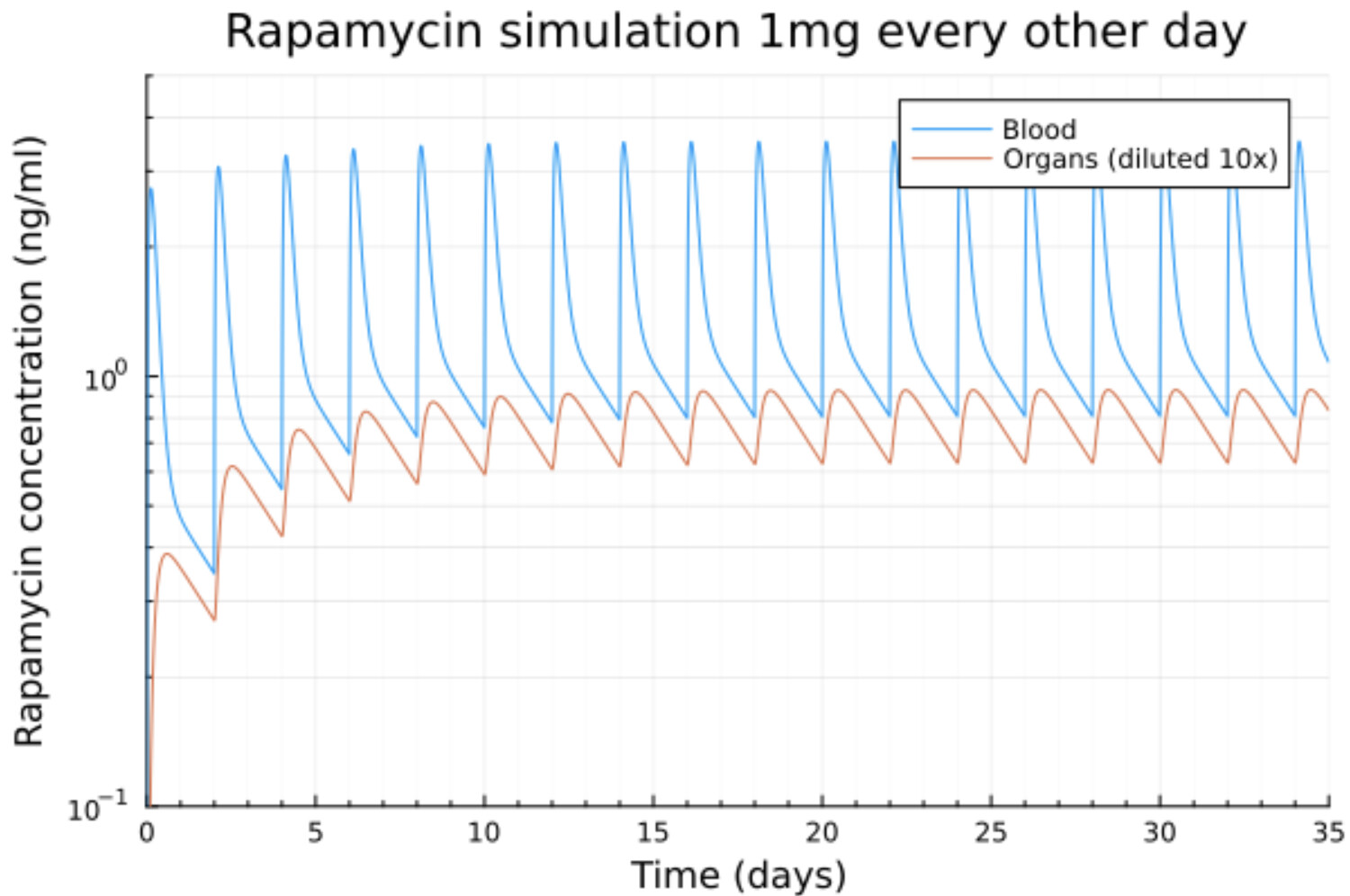
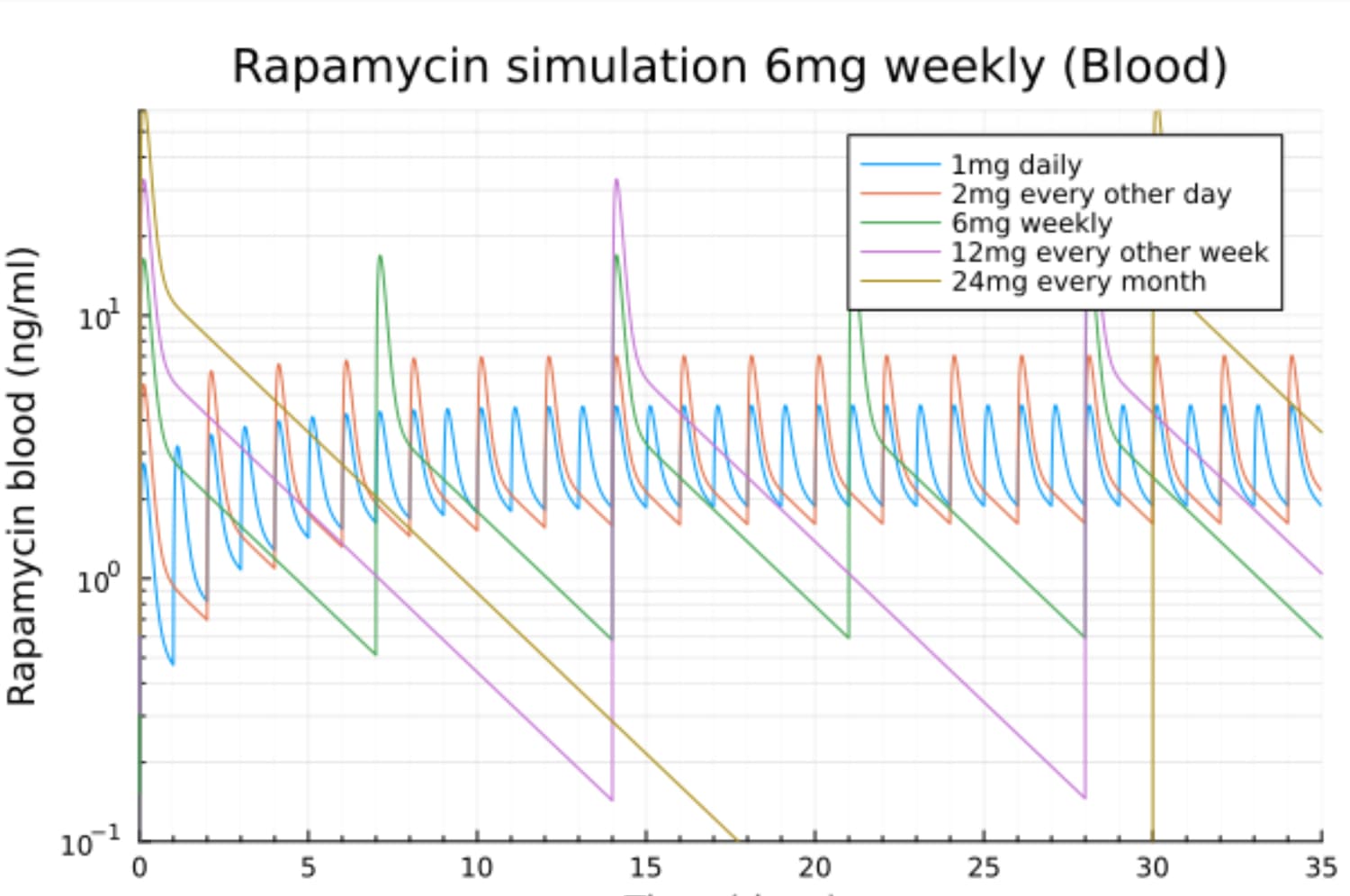
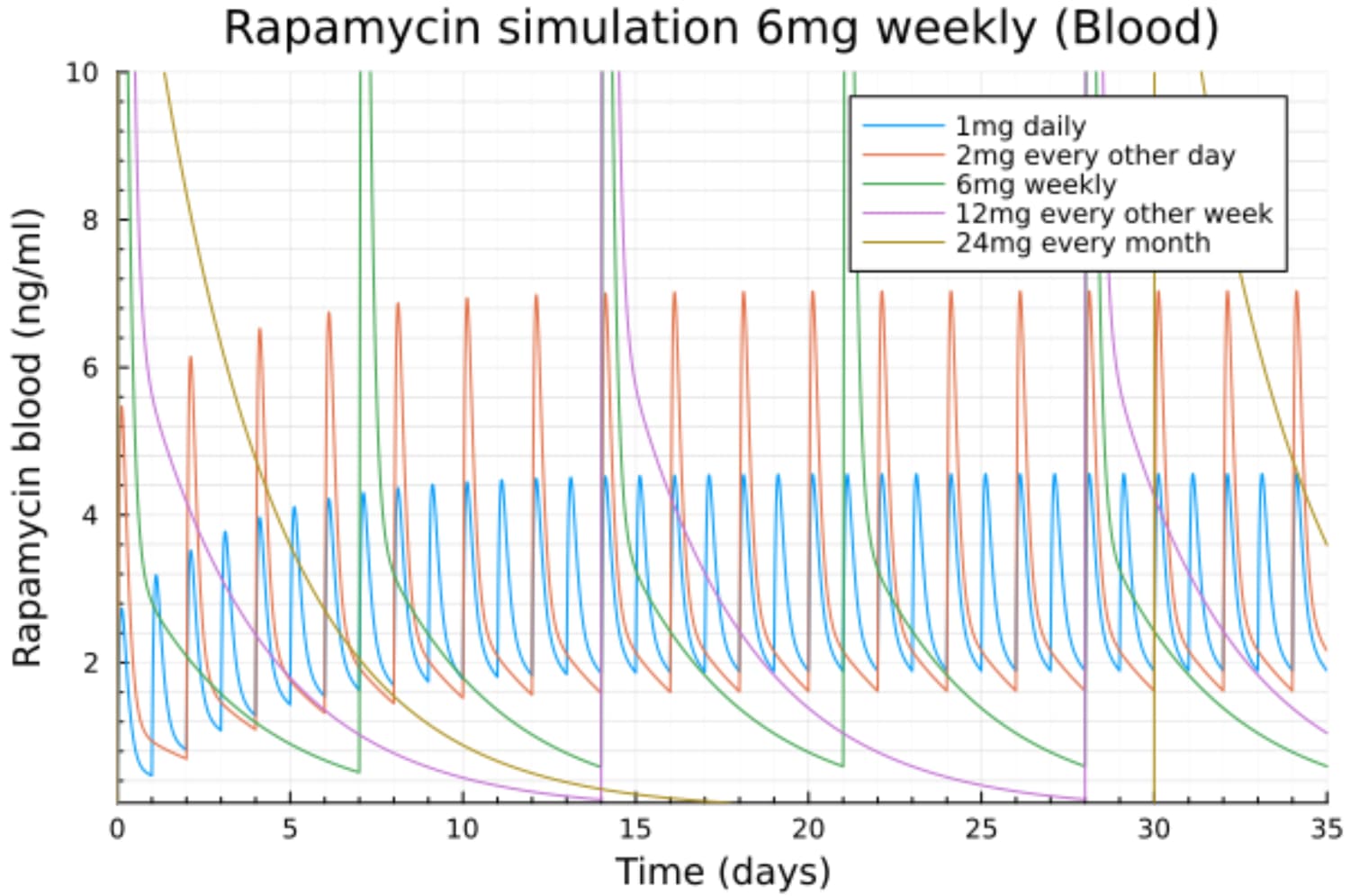
Can you do a simulation of 1 mg EOD (every other day)? As this is similar to the level in the 2014 Mannick paper at 0.5 mg everolimus a day and was as effective as 5 mg one time a week.
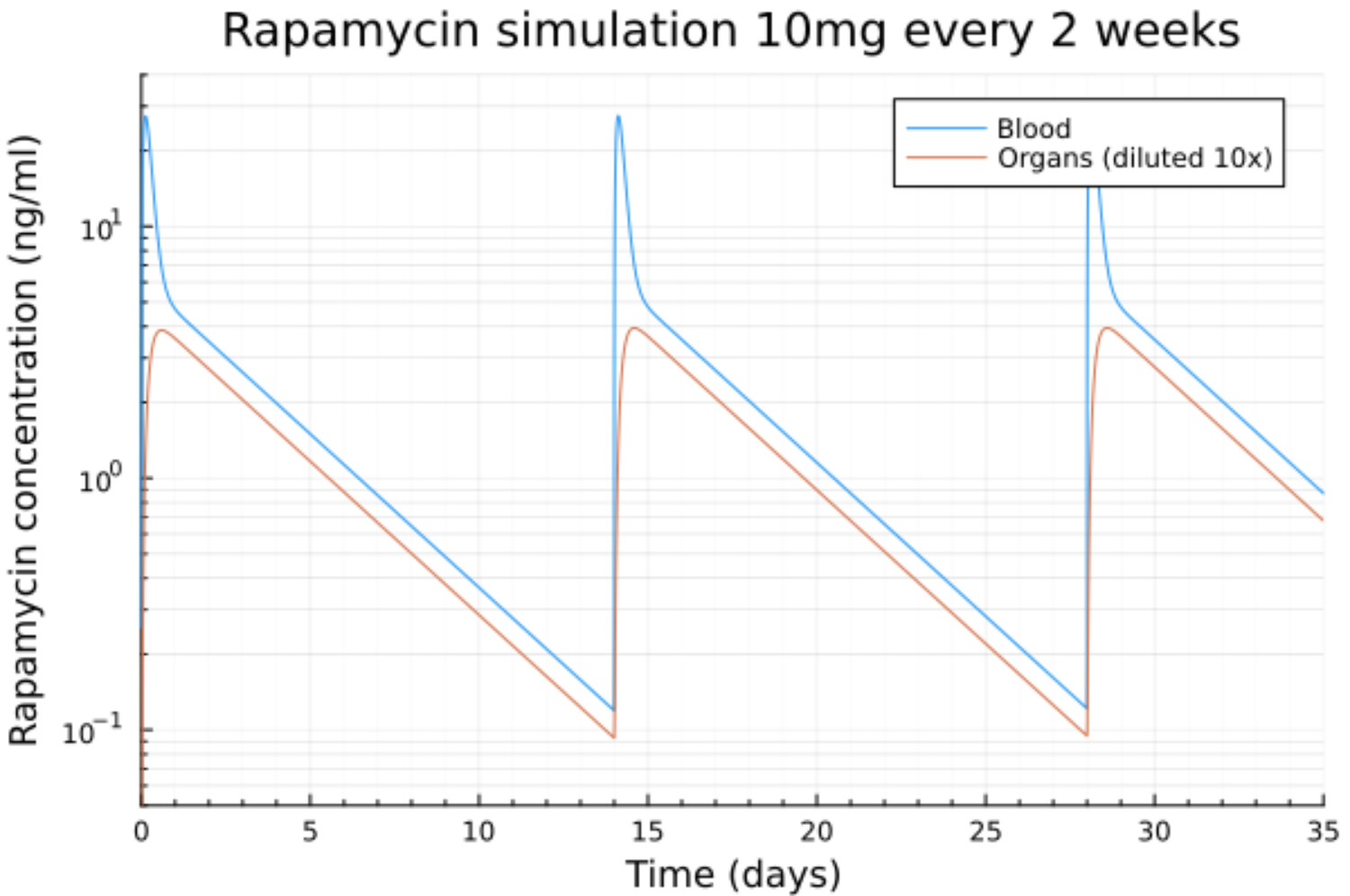
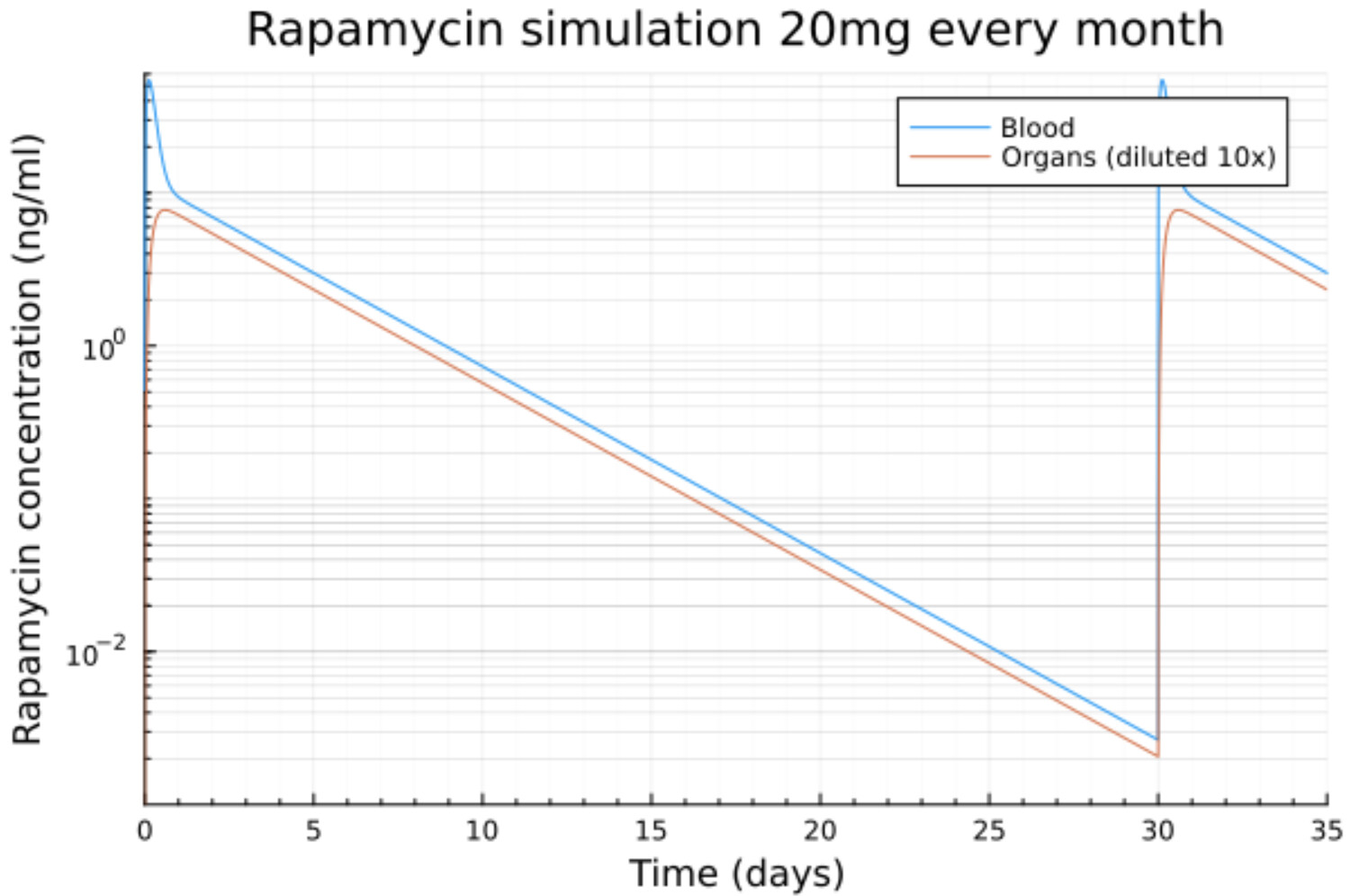
What about 10 mg every other week, and 20 mg one time a month?
It’s not an artifact. When the concentration is very low the elimination is also very low because the probability that a rapa molecule encounters an enzyme that will metabolize it is very low.
On the other hand the probability that this rapa molecule binds to mTOR is also very low.
That’s why some residual concentration will remain for a very long time but it will have no biological effects.
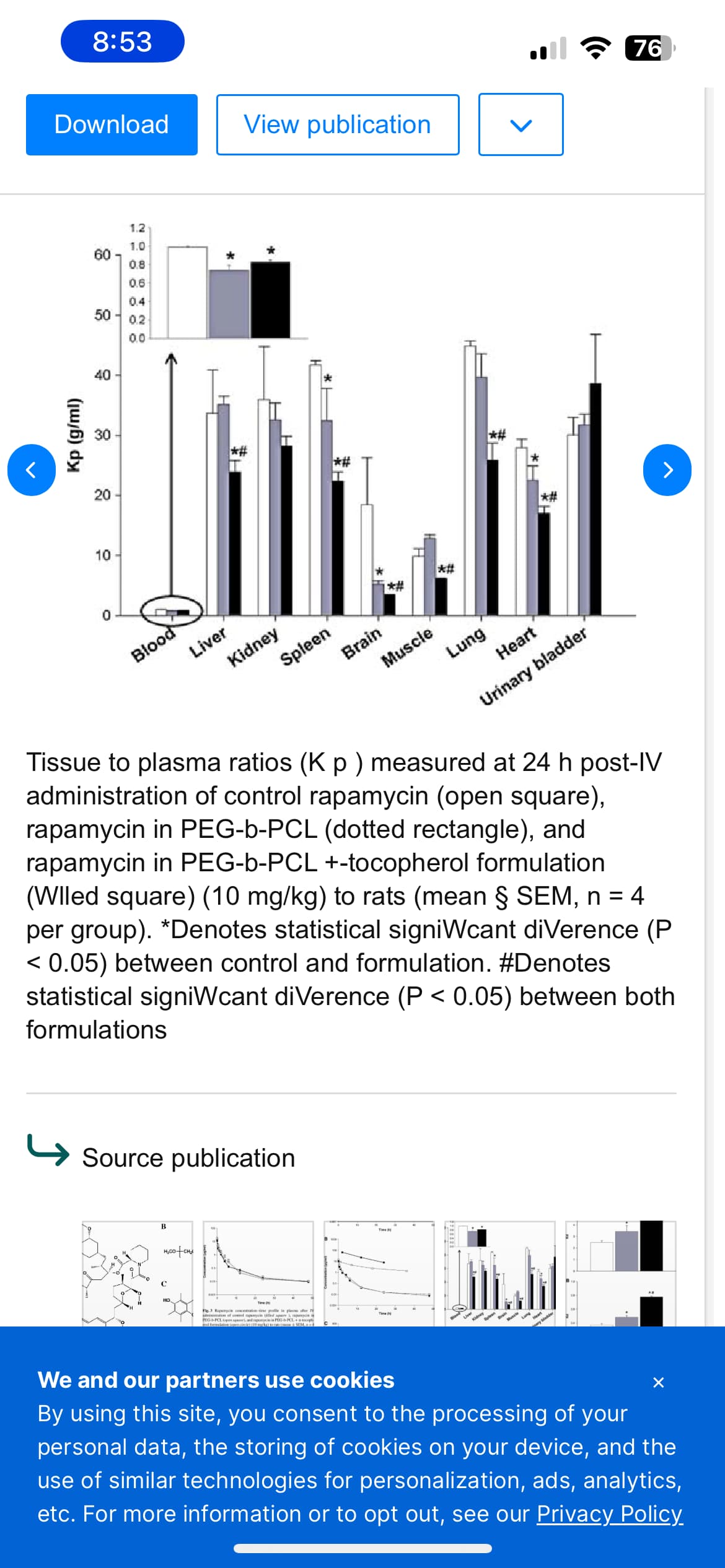
@cl-user where does the 10x dilution in organs come from?
I cannot find anything on people (who might not like having their organs assayed) but I found this paper on rat blood vs organs after 24 hours that was interesting. The rat clears its blood very fast but the organs retain the rapa longer, and of course the organs are fairly different in this function. I was surprised to see that muscle was low…would you think that is because it cleared faster or didn’t get in well like the brain (BBB effect)
Interpretation of the above needs to take into account the blood-to-plasma ratio (Rb)which is defined as Cb (blood concentration of compound) / Cp (plasma concentration of compound). Rapamycin exhibits a preferential distribution into red blood cells (94.5%) compared to plasma (3.1%), lymphocytes (1.01%) and granulocytes (1.0%) [30, 48]. Noted that Labcorp does whole blood level so edited.
For PK modeling after oral dosing, the frequency of sampling is critical, answering the question of what sampling times provide the most information to estimate the pharmacokinetic parameters. This requires some fancy schmancy math but greatly simplifying the issue: a) get enough time points around the a priori estimated Cmax/Tmax and b) the sampling frequency along the curve should be proportional to the magnitude of the absolute value of the second derivative of the log concentration time curve. This is an iterative process that requires several dosing experiments to gain familiarity with the pharmacokinetic behavior of a particular drug in a population of individuals with adjustment in sampling times based on the population variance results.
The volume of the body (all organs) is roughly 10 times the volume of blood + blood saturated organs so when N molecules of rapa go from blood to the organs they are diluted into a 10x greater volume.
The issue is that as shown in the paper you cite that distribution can be very different from one organ to another. The organs diluted by 10 is just the average concentration on all organs and there will be a lot of variations between different organs like brain vs liver for instance.
Unfortunately there is not enough data from just the blood concentration to calculate anything more meaningful than the average for all the organs.
@cl-user Thanks. I am learning today. One more big thing I do not understand about the model curves is related to blood vs organ rapa. What delay do you assume for human organs in clearing the rapa? The rat chart indicated that rat organs retained rapa after rat blood rapa was essentially (but not totally) gone after 24 hours. Would human organs retain rapa longer than a rat just as we seem to have longer half-lives of rapa in human blood?
No idea, it’s not a parameter of the model. Basically I use an optimizer to fit the parameters of the differential PK equations to fit the model to the measurements.
Maybe I can modify the model to estimate F though some data is missing like the volume of the blood compartment. I’ve seen estimates of 6l to 8l for that. A rough estimation for F here would be around 11%.