Who is taking low dose statin?
Type, amount and dosing?
Thank you
Joseph
Who is taking low dose statin?
Type, amount and dosing?
Thank you
Joseph
atorvastatin 10mg per day, prescribed many years ago to reduce cholesterol
if anyone replies to Joseph’s post, could you also state if you are taking it to reduce cholesterol or for general longevity purposes if your cholesterol numbers are normal?
I took 5mg Crestor for a long time due to a high APO-B. I recently switched to 40mg to get the number down to the 5% level. My post 40mg blood levels are due back this week.
What do you mean by “the 5% level”? do you mean 5% under the upper level that is recommended for APO-B?
5th percentile. Which is 60mg/dl
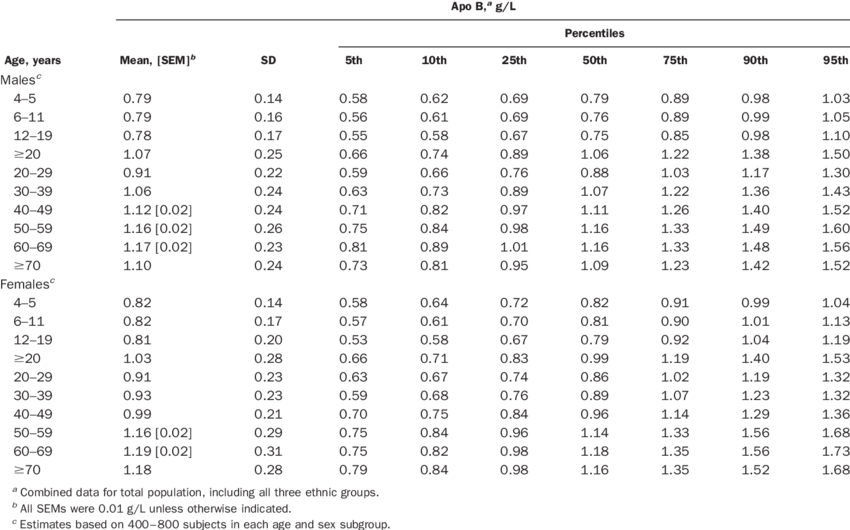
Do you have a different source for that info than this, which I just found on google (the NHANES study):
Or another one:
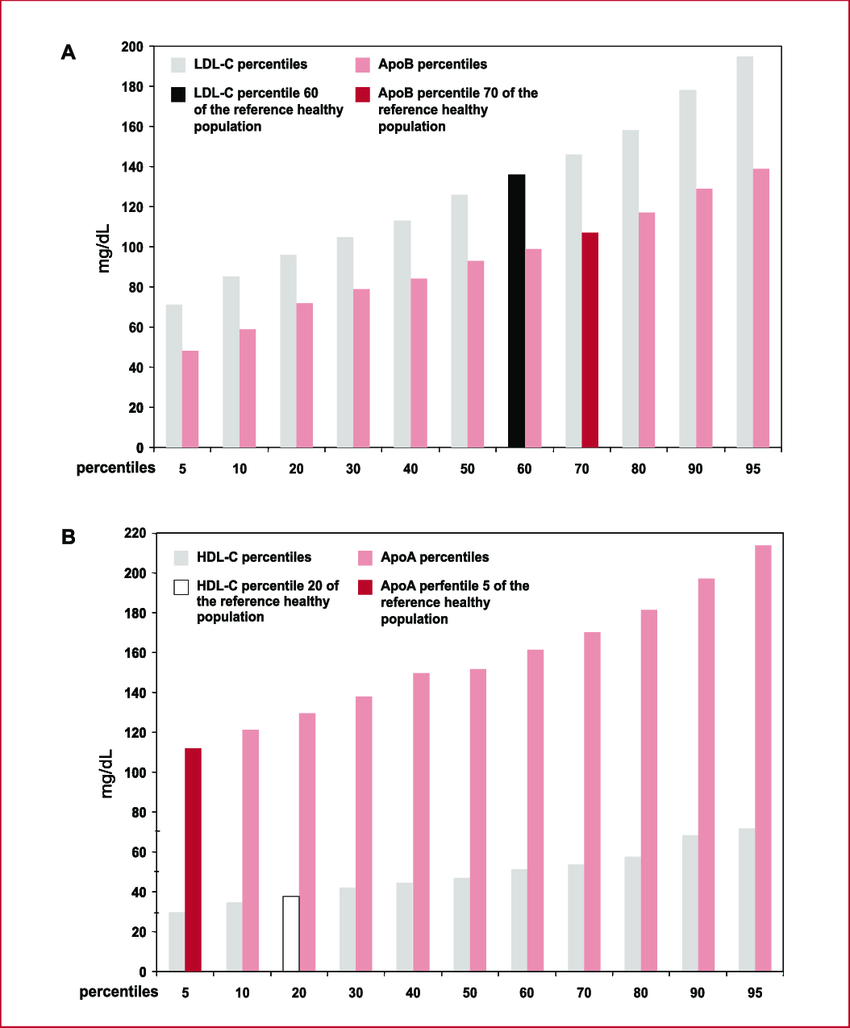
A. Comparison between the increasing percentiles of LDL-C with those of ApoB in a sample of healthy subjects. The mean level of LDL-C in patients with ACS corresponds to the percentile 60 of the healthy population (black column), while the mean level of ApoB corresponds to the percentile 70 (red column). This difference suggests that patients with ACS have smaller atherogenic particles. B. Comparison between the increasing percentiles of LDL-C with those of ApoA in the same population. The mean level of LDL-C in patients with ACS corresponds to the percentile 20 of the healthy population (light grey column), while the mean level of ApoA corresponds to the percentile 5 (light pink column). These findings suggest a marked abnormality in reverse cholesterol transport.
Source:
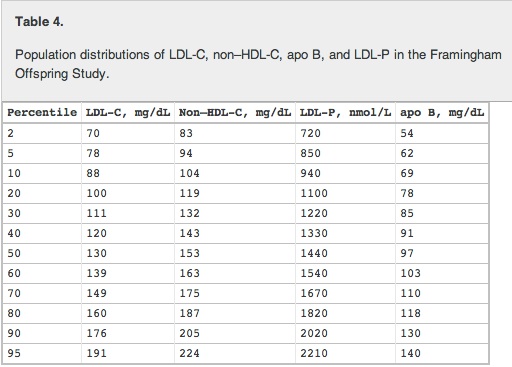
Or… here is the Framingham Offpsprings study results which seems closest to your citation:
My interest is for “longevity purposes”.
Looks like I have the wrong target in mind. Thanks for sharing!
And, I guess we should keep drinking our coffee:
I don’t know… those were just population studies… what I think I’d like to see is the level of APO-B that correlates to the lowest all-cause mortality rate… I would love to get people’s opinions on what the optimal APO-B target is for us, for lowest all-cause mortality.
I’m looking for that right now - here are some possible sources for this I’m reviewing.
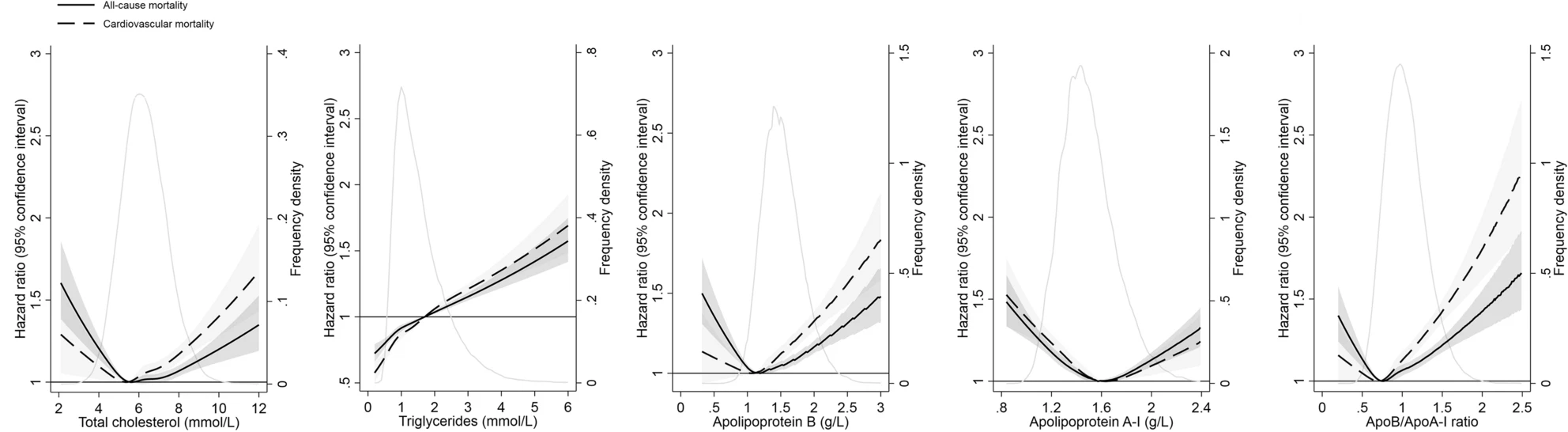
Here is something that looks like what I think I want - but it seems to suggest that the lowest all-cause mortality rate for APO-B is around 1.2 to 1.3 g/L (which coverts to around 120 to 130mg/dl - which seems high). Anyone have thoughts on this? See below…
Hazard ratios and 95% confidence interval for all-cause and cardiovascular mortality associated with concentrations of lipid biomarkers on a continuous scale over 25 years of follow-up (n = 98,270). Hazard ratios (solid line for all-cause mortality and dashed line for cardiovascular mortality) and 95% confidence intervals (gray area) are retrieved from Cox regression models with restricted cubic splines, adjusted for age, sex, and history of coronary heart disease, heart failure, atrial fibrillation, hypertension, diabetes, ischemic stroke, and transient ischemic attack. Solid gray line indicates the distribution of lipid biomarkers in the study population
Source:
https://www.nature.com/articles/s41598-021-03959-5
or, this one below, which seems to suggest that the lower APO-B, the better… I’m confused.
Conclusion: This study found a paradoxical association between baseline ApoB and long-term all-cause mortality. Malnutrition and bilirubin mainly mediate the ApoB paradox. Increased ApoB concentration remained linearly associated with an increased risk of long-term all-cause mortality.
And then in Medscape I find this:
Current guidelines define apoB greater than 130 mg/dL as a risk modifier in patients not using statins but, the authors write, “based on our results, the threshold for apoB as a risk modifier in statin-treated patients should be closer to 92 mg/dL than to 130 mg/dL.”
I personally take 5 mg. Crestor daily to reduce inflammation. It really works. Here is one video from Dr. Brewer, and he has many more on statins and how to measure inflammation in body. i.e. Microalbumin/Creanintine ratio in urine. LDL is not the main reason for taking a statin. Inflammation is the killer = plaque build up in arteries, turning calicified plaque into Hot plaque is killer.

Thank you for posting link.
I am have watched some of his videos, over the past year.
His video about Carotid Intima-Media Thickness (CIMT) testing and his own personal treatment for his plaque issue is what has me interested.
Have been considering taking 5mg rosuvastatin daily for “inflammation” / plaque control
What about liver issues with taking Statins? Any insights would be appreciated.
If you are a fan of Dr. Brad Stanfield you know he is a big fan of Cochrane reviews.
The evidence for adverse liver events is very low.
Statins reduce the risk of death from any cause
The link to the Cochrane review is in the article.
Here the idea of using a statin (as well as other drugs) in combination with rapamycin for life extension is spelled out by Mikhail V Blagosklonny, who was the first to propose the hyperfunction theory of aging.
Just to add to this idea that the direction of this Longevity Medicine field is definitely towards the idea of people ultimately taking a number of targeted drugs for the different biochemical pathways of aging, so as to optimize longevity.
I went to a talk by Kristen Fortney, co-founder of BioAge Labs here in the SF Bay Area last year.
Here is short summary:
For anyone else living in the SF Bay area - Loyal has some great aging science talks with local founders and scientists. This evening it was the founder of BioAge - they have three main drug targets in process right now. They use their proprietary proteomics / biomarker platform for identifying key pathways to target from longterm human blood etc. data , then do drug target validation using mice, then they in-license de-risked drugs from the major drug companies that have been safety tested already. Their first product, with a little luck, could be on the market in two years. When asked about their drugs in comparison to rapamycin, she suggested there are hundreds of likely targetable aging pathways that drugs will be developed for - so lots of opportunity for companies to develop new drugs and new businesses. She believes that the future will be an array of drugs that target many of these key pathways - and people will take a number of these drugs at once, so many of the drugs will be complimentary. The golden age of aging medicine is coming.
This was at the Loyal for Dogs Seminar series.
KB. This video was excellent. Regarding your 5 mg of Crestor, you notice any negative side effects? Also, why the 5mg daily and not say 10 mg? Just curious how you decided on that number?
This is an older Dr. Brewer video{How he treated himself] titled;
“How I Reversed 20 years of Arterial Plaque”

Statins have many side effects for some people. So you should only take a low dose statin. As dose goes up so does side effects. It is always a risk/reward decision. In this case, lower arterial inflammation in the body is most important. Some people get good results taking Crestor 5 mg., every other day, twice a week, and it still works to lower inflammation. 5 mg. dose came from Dr. Brewer. He has switched to Lovalo from Crestor, but too expensive here in Spain. STATINS SHOULD ONLY BE USED FOR PEOPLE WHO HAVE CONFIRMED THEY HAVE “PLAQUE IN ARTERIES.” (Calcium score, CIMT, or Cardiac Cath.) You can measure your inflammation with the HDL/Creantine serum ratio, and Microalbumin/Creantine ratio in a urinalysis. Get either of the above test, take low dose statin, and baby aspirin daily, and measure your progress via improvement in the scans. If you have plaque in part of body, let’s say heart, then you also have it in kidneys, and cartoid to brain.